











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Schwannomas are benign tumors of the Schwann cells which produce the myelin sheath that covers the peripheral nerves which can be found in patients with neurofibromatosis or without it1-2.
Despite the great innervation of the penis, the presence of these tumors constitutes an atypical manifestation with < 200 cases reported in the literature since its first description in 19681-4.
Case presentation
This is a 40-year-old male patient who presented to the urology specialist with the following characteristics. Patient denies important family history, denies smoking, and reports occasional alcohol consumption. The patient denies chronic-degenerative diseases, as well as previous hospitalizations. As the only surgical history, he refers adenotonsillectomy.
Within sexual life, the patient refers being married and reports having four additional partners, denies history of sexually transmitted diseases, as a contraceptive method he uses condom occasionally. Patient denies anal sex.
He began his current condition 7 years before the consultation with multiple new lesions on the genitals, which caused him pain during sexual intercourse.
On physical examination, five nodular-looking lesions with sizes ranging from 2 mm to more than a cm in diameter are observed in the dorsal portion of the penis, which is why sebaceous cysts are suspected (Fig. 1). Options are discussed with the patient; a preoperative US Doppler of the penis was requested, and circumcision was scheduled with resection of the penile tumors with vasectomy.

The ultrasound reported the presence of hypoechogenic nodular images with a trajectory toward the lateral region of the penis with displacement of the vascular structures (Fig. 2). Rest of the penis within normal characteristics.

The patient underwent surgical treatment, where seven irregular nodular tumors of multiple sizes with a smooth, opaque surface, and a grayish-white appearance were removed, which were well defined (Fig. 3). During surgery, no invasion of the corpus cavernosum or corpus spongiosum was identified. Circumcision and vasectomy were completed, and the procedure was finished.

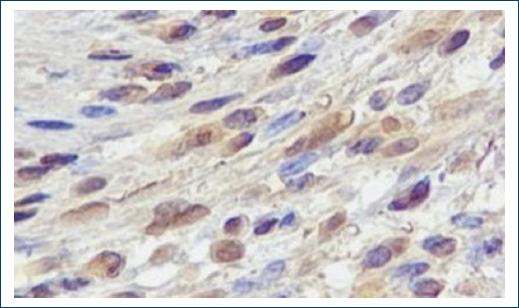
Histopathological report reveals benign well-defined mesenchymal neoplasms, with a capsule composed of spindle cells and poorly defined cytoplasmic boundaries, the cells form palisades and Verocay 1 and type 2 structures, elongated nuclei with granular chromatin without evident nucleoli, pleomorphism or atypical mitoses (Fig. 4). With the previous information schwannoma is suspected, so immunohistochemical staining is performed with PS 100 antibody, smooth muscle actin and CD 34, only the first one resulting positive, confirming the suspicion of schwannoma and ruling out the possibility of leiomyoma or benign fibrous histocytoma (Table 1 and Fig. 5).
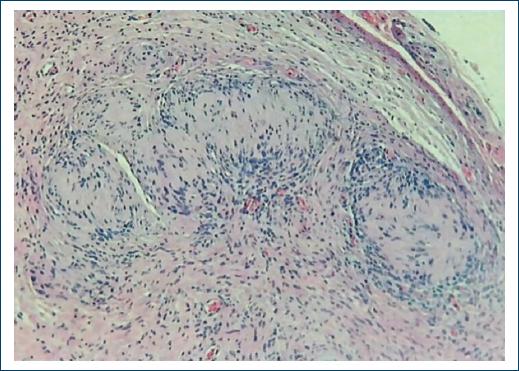
Table 1 Tumor immunohistochemistry
| Antibody | Interpretation |
|---|---|
| PS100 | Positive in the nuclei and the cytoplasm of all tumoral cells +++/´+++ |
| Smooth muscle actin | Negative |
| CD 34 | Negative |
The diagnosis of completely excised Schwannomas was integrated. The patient was informed about the importance of going to a neurologist to rule out neurofibromatosis.
The patient attends a follow-up consultation 7 days after and one month after surgery. The patient reported no sensory abnormalities or alterations in sexual function, so he was discharged from the urology service. He decides not to see a neurologist.
Discussion
Schwannomas are benign tumors of the Schwann cells which produce the myelin sheath that covers the peripheral nerves, which can be found in patients with neurofibromatosis or without it1-2. These tumors are frequent in extremities, face or head. Despite the great innervation of the penis, the presence of these tumors constitutes an atypical manifestation with < 200 cases reported in the literature since its first description in 19681-4. The average age of appearance is usually 39 years1.
They are encapsulated tumors of which different histological subtypes have been described based on the cells that compose them, the main ones being cystic, epithelioid, melanocytic, with psammoma bodies, and plexiform3.
These tumors have a very slow growth, so at diagnosis they can have several years of evolution5, within the differential diagnoses are the cysts of the middle raphe such as apocrine cystadenomas or mucous cysts which are remnants of the periurethral glands de Littre, other diagnoses to consider in the differential are warts, intentionally inserted foreign bodies, pearly penile papules, and penile carcinoma6,7. Pearly penile papules are lesions that correspond to normal glands which appear on the crown of the glans during adolescence. Another diagnosis to consider is the parafrenular glands which, as their name implies, generally appear three or four on each side of the frenulum6,7. Sebaceous cysts also tend to enter the differential which are usually discarded due to their rapid growth, these masses also usually appear in the scrotum.
Patients with Schwannoma of the penis usually seek help for erectile dysfunction or pain during sexual intercourse, other manifestations are pain on ejaculation or may debut as Peyronie’s disease. Pain is usually reported when the tumor grows between Buck’s fascia and the tunica albuginea5. These tumors are classified according to Antolini in Antolini A and Antolini B, being frequently mixed. Atolini A areas are composed of compact palisade cells with poorly defined cytoplasmic boundaries. Atolini B regions are made up of randomly distributed spindle cells4-8. In immunohistochemistry, these tumors are usually intensely positive for the S-100 protein, unlike median raphe cysts, which are usually positive for avidin-biotin peroxidase, epithelial membrane antigen (EMA) Human milk fat globule antigen 1 (HMFG1), proteases CK7, and CK135. Multiple imaging studies may be useful in the diagnosis, these neoplasms on magnetic resonance imaging are usually isointense on T1 sequences and hyperintense on T2 sequences with fat saturation, they usually have homogeneous gadolinium enhancement. On ultrasound, these tumors can be hyperechoic1-4.
The only curative treatment for these neoplasms is surgical resection, which is usually sufficient on its own in most cases; in extremely rare cases of malignant Schwannoma, penectomy plus adjuvant radiotherapy may be indicated3.
Conclusion
Schwannomas of the penis are a rare neoplasm with very few cases in the literature; the diagnosis is based on physical examination and imaging studies, with the histopathological study confirming it. In almost all cases, these tumors are benign, with surgical treatment being the treatment of choice, with no cases of recurrence reported to date.

