











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Peyronie's disease (PD) is a connective tissue disease that primarily affects the tunica albuginea of the corpora cavernosa of the penis. François De La Peyronie (1678-1747) first described this disease in a medical treatise addressing ejaculatory failure. It usually presents with a palpable induration of the penis, which causes deformity during erection.
The formation of fibrous plaques in the tunica albuginea and surrounding cavernous tissue alters the anatomy and causes deformities of the penis that is acquired during erection with different degrees of flexion and narrowing of the circumference of the MIMO. This condition can occur with or without pain and can cause erectile dysfunction. Currently, therapy remains a controversial matter. There is no consensus on the utility of medical and surgical treatment. This article aims to conduct a systemic review of PD and discuss currently available treatments.
Definition
PD is a congenital or acquired penile abnormality, which is characterized by fibrosis of the tunica albuginea1. The fibrous tissue in the tunica albuginea prevents the expansion of the latter during erection, resulting in shortening, flexion, and pain of the penis, which is associated with sexual dysfunction2 (Fig. 1).

Pathophysiology
The development mechanism of PD is unknown. However, one of its causes can be due to a prolonged and sustained inflammatory response, triggered by trauma, which allows extravascular protein deposition, inflammatory cell recruitment, fibrin deposition on the expression of inflammatory cytosines, and release of elastase1, which leads to a change of type I collagen into type III collagen. Overexpression of transforming growth factor (TGF)-B and interleukin (IL)-6 has been reported together with a lower number of blood vessels and reduced apoptosis in the histopathological samples of patients with PD3.
Currently, the active role of free radicals is recognized as inducing an important inflammatory response, favoring the first stage of this disease. There is an important expression of pro-inflammatory and pro-fibrotic cytosines, with subsequent activation of the NF-kB factor4.
Another hypothesis states that it is a scar tissue disorder developed by genetic susceptibility, based on documentary evidence of variations in the TGF-beta 1 gene and expression of SMAD transcription factors, which regulate the mechanisms of fibrosis2. The histological features of PD show lymphocytic and plasmacytic infiltrate of the tunica albuginea, as well as of the erectile tissues (fig. 2)3.
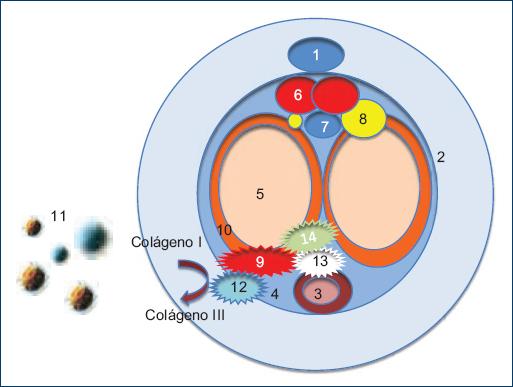
Figure 2 Peyronie's disease pathophysiology. 1: dorsal vein of the penis, 2: skin, 3: urethra, 4: Buck's fascia, 5: cavernous body, 6: dorsal artery, 7: deep dorsal vein, 8: dorsal nerve of the penis, 9: defect in the tunica albuginea, 10: tunica albuginea, 11: T and B lymphocytes, 12: fibrin deposit, 13: cytosine overexpression, 14: elastase release.
Epidemiology
PD mainly affects men aged between 40 and 70 years, mostly of Caucasian origin, with a prevalence of 0.4-9%, and an incidence of 0.39-3%3,4. The risk factor that is majorly associated with PD is trauma. Other associated factors to a lesser extent are peripheral vascular disease, smoking, alcoholism, and some invasive urological procedures (transurethral resection of the prostate and cystoscopy)5. Other studies comment on an inverse relationship, with high LDL levels and abdominal circumference, treatment with thiazides and Dupuytren's disease4.
Diagnostic approach
A thorough enquiry and physical examination should be performed for a basic evaluation, with an artificially induced erection to measure and document the degree of curvature, as well as document the fibrous plaque by ultrasound scan, if such procedure is available. Patient information should also be collected about the onset of the disease and duration, a history of trauma to the genitals and perineum, the development of penile deformity, curvature, penis shrinkage, erectile dysfunction, and subjective evaluation of the erectile and sexual function2.
Clinical presentation
We usually come across patients in their fifties, with a recent onset of curvature in the penis, which is related to mild to moderate pain. The erection is not affected at the beginning. However, the curvature can bring difficulties in sexual activity. It is worth mentioning that abnormalities in the flaccid penis are not palpable1. During the course of the disease, it can be classified as active and stable.
Pain or discomfort is reported in the active presentation, with or without an erection, associated with a history of penile injury during sexual activity, although most patients do not remember any incident. The erection may be intact or compromised. The disease stabilizes once no changes in symptomatology are reported within at least 3 months. This generally occurs around 12-18 months after the onset of symptoms. Pain rarely occurs and when it does, it is typically of mild intensity. The plaque is palpable or evident on ultrasound scans with an obvious deformity of the penis1.
Over time, the penile curvature will get worse in about 30-50% of patients with PD and will stabilize in 47-67% of cases. Pain occurs in about 35-45% of patients at an early stage of the disease and subsides in about 90% of cases at 12 months after the presentation of symptoms6. As for findings, comments during medical examinations state that 100% of the patients presented induration, 83% presented induration accompanied by angulation, 46% presented induration accompanied by pain, and only 32% of patients presented induration, angulation, and pain7.
Treatment
There are several types of treatment for PD, which must be chosen with moderation and according to the needs and response of the patient. In general, approaches to treatment should range from less to more invasive ones. Patients with active disease, instability or progression of the deformity should receive conservative treatment, as well as patients with painful erections (particularly on palpation) or those who are not interested in surgical treatment8.
Surgical treatment is recommended to those patients who have presented symptoms for at least 12 months or patients whose penile curvature or deformity has become stable for at least 3 months1. The invasive approach can also be offered to those who have not had a response to medical treatment; patients with unsatisfactory intercourse or those who desire faster results2. In its acute phase, nonsteroidal anti-inflammatory drug analgesics are recommended for pain management. Table 1 shows a summary of pharmacological treatment for PD.
Table 1 Pharmacological treatment of PD
| Pharmaceutical drug | Mechanism of action | Utility |
|---|---|---|
| Vitamin E | Reduction of free radicals | No evidence of its utility1 |
| Potaba | Inhibits the secretion of glycosaminoglycans | Decreases plaque size, without impact on curvature2,3 |
| Tamoxifen | Decreases fibrogenesis in the tunica albuginea | No improvement in plaque or curvature2 |
| Colchicine | Inhibits collagen deposition and decreases TGF-beta 1 expression | Decreases plaque size, without changes in curvature2,3 |
| Carnitine | Acetyl-CoA carboxylase inhibitor | Reduces pain, curvature, and stops progression3 |
| L-Arginine | cGMP increase | In animal models, it decreases the size of the fibrous plaque and the expression of type I collagen2 |
| Pentoxifylline | Nonselective phosphodiesterase inhibitor | Chronic disease improves curvature and plaque volume2 |
| Corticosteroid | Immune response | No improvement1 |
| Collagenase clostridium histolyticum | Interstitial collagen degradation | Decreases curvature, prevents progression2 |
| Interferon alfa-2b | Inhibits the production of fibroblasts and collagen | reduces plaque size and pain1,14 |
| Verapamil | Calcium channel blocker | No clinical improvement2> |
PD: Peyronie's disease; TGF: transforming growth factor.
Oral treatments
Vitamin E
A fat-soluble vitamin that acts as a natural antioxidant reducing the number of free radicals produced during metabolism. There is no evidence supporting its utility or demonstrating its therapeutic benefit in PD9. However, it is frequently prescribed due to its low cost, easy availability, minimal adverse effects, in addition to its placebo effect10.
Potaba
Potassium paraminobenzoate has anti-inflammatory and antifibrous properties, inhibiting the secretion of glycosaminoglycans by fibroblasts and stabilizing serotonin monoamine oxidase activity. Several studies have evidenced improvement in plaque size after 12 months, and improvement in pain, without having an effect on pre-existing curvature11.
Tamoxifen
Is an estrogen receptor antagonist whose mechanism of action in the tunica albuginea is the reduction of the fibrogenesis by the modulation of the release of TGF-beta 1. However, it does not generate significant improvement in pain management, penis curvature, or size12.
Colchicine
It reduces the contraction of wounds and inhibits collagen deposition by decreasing the expression of TGF-beta 113. Some studies comment that it helps in the management of pain in 95% of patient's decreases curvature in 30% of patients14 and decreases the density of the fibrous plaque in approximately 50% of patients6. Other contrast studies reveal that no significant difference has been demonstrated when compared to placebo trials15.
Carnitine
An Acetyl-CoA carboxylase inhibitor, which has anti-inflammatory properties16, presents greater benefits compared to tamoxifen in reducing pain, curvature, and stops progression though it does not reduce plaque size6.
L-Arginine
A nitric oxide precursor and its anti-inflammatory mechanism is assumed as due to the increase in cGMP. In animal models, it reduces the size of the fibrous plaque and the expression of type I collagen, although no studies have been conducted in humans17.
Pentoxifylline
Is a non-selective phosphodiesterase inhibitor that restricts fibroblast proliferation, it also contributes by the diminishment of collagen deposits and eslastogenesis18. It improves curvature and plaque volume in patients with chronic disease19. It is also believed to stabilize or reduce calcium content in the plaque20.
Intralesional treatment
Corticosteroids
Corticosteroids have an anti-inflammatory effect secondary to suppressing the immune response. Nonetheless, several studies state that it does not present statistically significant evidence for its administration21.
Collagenase clostridium histolyticum
Its mechanism of action is through the degradation of interstitial collagen2. It should be administered in patients with stable disease and/or curvature between > 30° and < 90° and intact erectile function1. It reduces penile curvature in patients with the curvature of 30°-90°, patients who present more than 2 years of evolution, those who do not develop plaque calcification and patients who have an IIEF > 17. It is thought to reduce sexual activity difficulties in patients with penile curvature ranging from 30° to 60°, disease history of more than 4 years of evolution, non-calcified plaque, IIEF 1-5, and IIEF > 1722. Important complications have been reported after the application of this treatment, such as penile hematoma and fracture, detected in up to 10% of patients23.
IL alpha-2b
IL alpha-2b regulates the immune response, inhibiting the production of fibroblasts and collagen, in addition to increasing collagenase activity. One study reports that it reduces plaque size in 13.5% of patients, and pain in 67.7%1. Another study reveals that sexual function improves in 30% of patients24.
Verapamil
Is a calcium channel blocker that contributes on the regulation of the inflammatory response and fibroblast proliferation25. However, it does not generate a significant difference with respect to the placebo effect, when plaque size, pain, penile curvature, and sexual function were compared3. One study reports that patients treated with intralesional verapamil for control purposes showed a decrease in plaque size in 17.5% of patients, pain reduction in 30%, reduced curvature in 17.5%, and improvement in sexual function in 5% of patients. One study states that topical verapamil applied for 9 months decreases penile curvature in 61.1% of participants, with plaque size reduction in 84% of them, pain reduction in 100%, and improvement in the quality perception of erection in 81% of patients26.
Hyaluronic acid
The use of hyaluronic acid has been recently described. Several intra-lesion therapeutic protocols have been proposed for the treatment of PD. A recent study compared the effectiveness of verapamil against hyaluronic acid, stating that the hyaluronic acid group had a greater decrease in curvature and better patient acceptance27.
Non-pharmacologic treatment
Stem cells
Stem cells prevent fibrosis, inducing immunomodulation, which produces phenotypic changes of fibroblasts. Some experiments have been conducted in animal models with induction, where stem cells are applied during its acute phase. These have prevented the development of plaque formation, though there are no studies evidencing its efficacy and safety in humans. Stem cells that have shown greater benefits in animal models are those derived from the adipose tissue. More prospective studies in humans are necessary for a thorough understanding of this therapeutic tool28.
Radiotherapy
Radiotherapy has been used for a long time for PD management because it was thought to help fibrous plaque degeneration. However, all current recommendations contraindicate it29.
Vacuum pump
It presents clinical and statistically significant improvement as PD therapy. Its effectiveness was evaluated in a study where it is commented that 67% of the participants reported a decrease in penile curvature, 10% had an increase in curvature, and 23% of participants did not present any modifications. In addition, 51% of participants declared that they were satisfied with the results, though other participants required surgical procedures. It is concluded that the vacuum pump improves or stabilizes the curvature of the penis, reducing the need for surgical treatment30.
Extracorporeal shockwave therapy (ESWT)
ESWT is viewed as effective for pain management and improvement of sexual function31 but should not be used to reduce curvature or plaque size1. A study commented that 85% of the participants reported improvement in pain symptoms compared to 48% of participants in the control group. Deviation worsened in 40% of participants and only in 24% of the control group patients. An increase in plaque size was found in 10% of the participants, with no patients in the control group reporting an increase in plaque size31.
Surgical treatment
Surgical treatment is aimed to correct penile curvature or deformity, by preserving or restoring erectile function and preventing shrinkage or loss of girth2. The most common inclusion criterion for performing the surgical treatment is that 12 months must have elapsed from the onset of symptoms and evidence of stable curvature for at least 3 months6. In addition, it can also be offered to those patients who do not have satisfactory intercourse, present failure in conservative treatment and those seeking quicker results6.
Some studies comment that conservative treatments of PD are useful for improving pain during erection, but only a small percentage of patients experience penis straightening6. There are multiple surgical techniques described for PD correction; however, the most used and most frequently cited are tunical plication, enlargement of the tunica albuginea (incision or excision) and the use of penile prosthesis2.
Tunical plication
Tunical plication is the most commonly used technique, representing approximately 50% of all surgeries performed for PD. It is used in patients whose erection is suitable for intercourse or who have erectile dysfunction that responds to medications or vacuum pump1.
The Nesbit technique is the most commonly used technique, which involves the excision of a portion of the tunica albuginea on the contralateral side of the curvature32. This procedure may result in a decrease in penis size2. Studies state that the direction and degree of curvature before surgery predicted this decrease in penis size33. A retrospective analysis was conducted in 52 patients undergoing penile plication for the treatment of PD or congenital curvature of the penis. This analysis was compared with techniques that involved degloving or not. Surgical success rates, complications, and patient satisfaction were evaluated with the treatment benefit scale. The overall surgical success rate was 92.3%, with an average follow-up of 18.84 ± 23.51 months. There were no intraoperative complications. In the degloving group, 42.6% of the patients were very satisfied and 42.6% reported better results. In the group that did not undergo degloving procedures, 61.5% of the patients were very satisfied and 30.8% reported better results. The comparison of the results was not statistically significant between the groups34. Currently, this technique is widely used because it is simple, minimally invasive, and preserves sexual function. However, it decreases penis size and does not correct the hourglass defect or hinge effect2.
Enlargement of the tunica albuginea
It is used in patients with adequate erection for intercourse and severe deformity (curvature > 60°, or articulation with severe plaque calcification)2. The most commonly used procedures for tunica albuginea enlargement include partial excision or incision and grafting. Partial excision has displaced complete excision because the latter is greatly associated with erectile dysfunction, and even partial excision can improve sexual function35,36.
The cut is made in the area of maximum curvature, using a double-Y or H incision37. The grafts commonly used are obtained from the dermis, saphenous vein, oral mucosa, proximal crura, tunica vaginalis, dura mater, temporal fascia, and fascia lata38. Synthetic grafts such as Dacron and polytetrafluoroethylene are currently used39. Recent studies comment that this surgical technique helps to straighten the penis in 80-100% of patients. The most frequently encountered complications are hypoesthesia, persistent or recurrent curvature, and erectile dysfunction6.
Penile prosthesis
It is used in patients with PD that have erectile dysfunction and/or sufficient deformity to prevent intercourse despite oral medication or vacuum pump1. It is also used in patients who present a complex deviation that cannot undergo corporoplasty or grafting to improve shrinkage40. Two types of prostheses are most frequently used, malleable prostheses and inflatable prostheses. The most accepted in the management of patients with PD are inflatable prostheses due to better sexual satisfaction for the patient, less residual curvature, and successful straightening41. An inflatable prosthesis can be used as an effective corrective tool in patients with an unstable penis due to indentation or hourglass deformity and minimal curvature3.
If proper straightening is not achieved with the use of inflatable prostheses, the first step is the manual modeling of the penis2. In case of failure of this penile straightening method, the next step is plication, with multiple incisions in the tunica albuginea or excision with or without graft39,42. The most commonly presented complications are penis shrinkage, hypoesthesia, paresthesia, difficulties in inflating and deflating the device, mechanical failure, erosion, and infections43.

