











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Sarcoidosis is a multisystem, inflammatory disorder of unknown cause characterized by the formation of epithelioid, non-caseating granulomas1. The presence of granulomas in the absence of other granulomatous diseases is characteristic of sarcoidosis2. It is usually diagnosed in patients between 20 and 40 years of age, with a greater incidence in female patients3. The lungs and lymphoid system are the most commonly involved sites, with a frequency of 90% and 30%, respectively4. Extrapulmonary involvement is observed in 30% of patients, with the abdomen being the most frequent site. However, peritoneal involvement is extremely rare5. Abdominal sarcoidosis can occur in the absence of lymphatic or pulmonary disease6. The lesions are uncharacteristic, mimicking more common neoplastic or infectious diseases such as lymphoma, peritoneal carcinomatosis, granulomatous, or mycobacterial infections7. Although usually asymptomatic, the presence of symptomatic abdominal involvement can affect prognosis and treatment options. Symptomatic abdominal sarcoidosis requires treatment with immunosuppressant agents1. We will describe a rare case of peritoneal sarcoidosis mimicking carcinomatosis in a young patient.
Case report
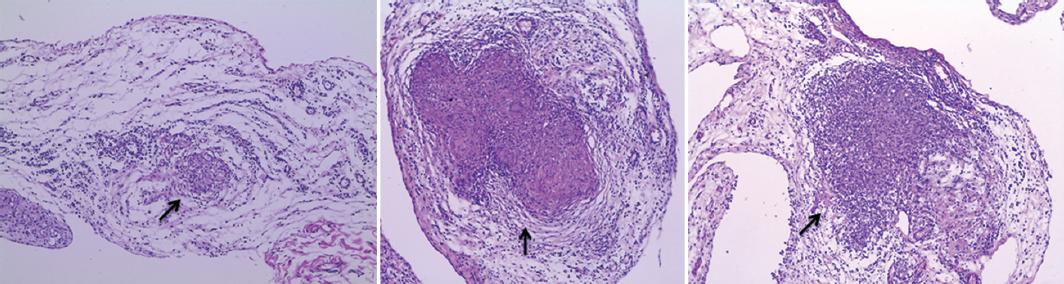
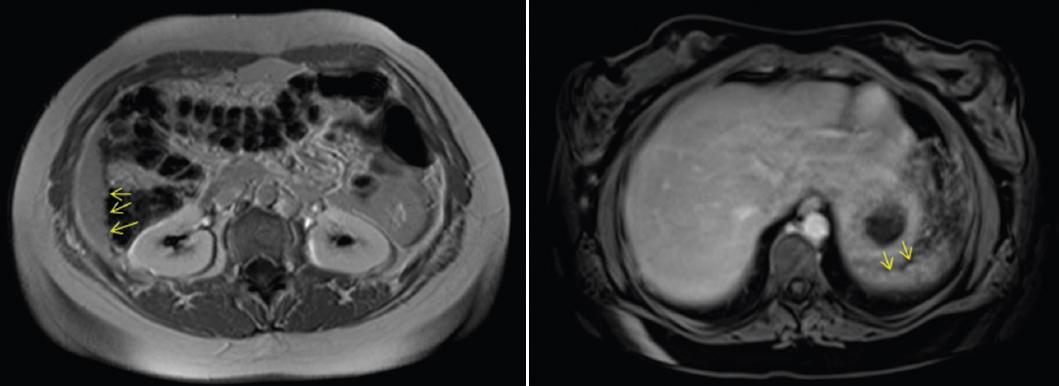
A 29-year-old female patient, with a history of slowly resolving pneumonia associated with pleural effusion 3 years earlier, attended at the Emergency Room with a moderate intensity generalized abdominal pain starting 3 h ago, predominantly located in the hypogastrium, continuous with colic exacerbations, associated with episodes of vomiting of gastro-bilious content. On physical examination, she was clinically and hemodynamically stable, with preserved vital signs and a soft lax abdomen with mild tenderness and guarding over the right iliac quadrant and hypogastric region without definite rigidity as in peritonitis. Laboratory tests showed 7300 white blood cells/dL, with 74% neutrophils and 0% eosinophils, CRP 0.49 mg/dL, erythrocyte sedimentation rate 25 mm/h, negative human chorionic gonadotropin, and normal urine test results. Abdominal and transvaginal ultrasounds were requested, both normal, and because she continued with symptoms, a CT scan of the abdomen and pelvis with intravenous contrast was requested, which showed diffuse thickening of the appendix with concentric reinforcement, homogeneous post-contrast, and inflammatory edematous appearance (Fig. 1). In addition, minimal thickening was visualized with increased density of the greater omentum on the left margin (non-specific) and a 3-mm calcification in the lower sector of segment 8 of the right hepatic lobe. The patient was admitted and underwent laparoscopic exploration, where multiple punctate lesions were observed throughout the peritoneum, proximal, and distal small intestine and in the colon (Fig. 2). The appendix presented the same characteristics. At the pelvis, both fallopian tubes were found with lesions of the same characteristics and serous free fluid was visualized at the bottom of the pouch of Douglas (Fig. 3). Samples were taken from the peritoneal right flank and from the hepatic adhesions, with seeding of lesions (Fig. 4), and the decision was not to perform appendectomy. The histopathological study revealed granulomatous peritonitis with non-necrotizing sarcoid granulomas, PAS, and ZN negative; and the cytological smear of the abdominal fluid showed mesothelial cells, lymphocytes, and neutrophils (Fig. 5). The post-operative period was uneventful without complications and the patient was discharged from the hospital 48 h after surgery. Evaluated by the Rheumatology Department, an immunological laboratory test was requested showing negative ANA, ENA, anti-DNA, ANCA, normal complement, Beta-2 microglobulin 1.7 mg/dL (normal range: 0.8-2.2), ECA 24.2 UI (normal range: 8-52), and normal proteinogram by electrophoresis with 1.5 g% of gamma globulin, normal both serum and urinary calcium levels. In addition, IgG4 was normal, and an MRI of the abdomen showed small hypointense nodules in very small numbers, visible in the right hepatic lobe and the subcapsular splenic medial border, associated with a small amount of laminar perihepatic and perisplenic fluid (Fig. 6). The patient started treatment with methotrexate 20 mg/week, folic acid 10 mg/week, and colchicine 1 mg/day, with clinical improvement.

Figure 1 Axial computed tomography scan where diffuse thickening of the appendix can be seen (yellow arrow).


Figure 3 Intraoperative findings: uterine tubes with punctate lesions and serous free fluid at the pouch of Douglas.

Figure 4 Intraoperative findings: hepatic adhesions with seeding of lesions from which samples were taken.
Discussion
Sarcoidosis is a granulomatous disease with predominant pulmonary involvement. Although abdominal sarcoidosis represents 30% of extrapulmonary manifestations, peritoneal involvement is rare, and the exclusive presence of peritoneal sarcoidosis without pulmonary involvement is exceptional8. Extrapulmonary involvement depends on gender, age at diagnosis, and ethnicity9.
Most cases occur in women between the second and fourth decades of life10. A literature search was performed in PubMed, where it was found that there are only 33 cases of peritoneal sarcoidosis reported to date, with the first case reported by Robinson and Ernest in 195411.
The most frequent clinical presentation is abdominal pain, but it is often asymptomatic12. It most commonly presents as ascites or granulomatous peritoneal nodules, requiring pathological examination by a biopsy to rule out peritoneal carcinomatosis or tuberculous peritonitis13.
In general, the diagnosis of peritoneal sarcoidosis is established when clinical and imaging findings are supported by typical histopathological findings in the peritoneum. Non-caseating granulomatous inflammation and other causes of granulomas, such as infectious diseases (tuberculosis, histoplasmosis, brucellosis, and toxoplasmosis), autoimmune disorders (granulomatosis with polyangiitis, primary biliary cholangitis, and Crohn's disease), occupational and environmental exposures (beryllium, talc, and fungi), delayed-type hypersensitivity to foreign agents, and neoplasms should be excluded14.
As the differential diagnoses of this granulomatous process are extensive, diagnostic laparoscopy is often required to reveal the involvement of granulomatous disease in the visceral and parietal peritoneum since imaging studies such as tomographies are often unable to detect them due to their small size15.
Laboratory studies are often unrevealing, and peripheral lymphopenia with CD4 depletion, hypercalcemia, and hypercalciuria may be found. Elevated CA 125 levels have been observed in some cases of peritoneal sarcoidosis, but it is still uncertain whether it would be a reliable marker of sarcoidosis activity5,16 since it is also present in other causes of benign and malignant peritoneal diseases16. Although elevated ACE levels have been repeatedly observed in patients with sarcoidosis, increased concentrations have not been directly correlated with peritoneal involvement15.
Most cases of peritoneal sarcoidosis have a benign course, resolving spontaneously or with a short course of corticosteroids17, sometimes with the addition of methotrexate18, as in the case of our patient.
Conclusion
Sarcoidosis is a multisystem, inflammatory disorder of unknown cause. Although peritoneal involvement is extremely rare, it may mimic peritoneal carcinomatosis and should be suspected as a differential diagnosis, especially in young women. The diagnosis is established when clinical and imaging findings are supported by typical histopathological findings. Most cases have a benign course.

