











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Surgical resolution of pregnancy through cesarean section is one of the most important advances in contemporary perinatal medicine. Cesarean section has had an extraordinary impact in reducing maternal and perinatal mortality1. It is the most frequently performed surgery in the world and is increasing every year. Reports have documented its increase in both developed nations and developing countries2,3. Frequencies exceed the 10-15% recommended by the World Health Organization for performing said surgery4. The experts have explained that the preference of the method for the convenience of the doctor, surgery at the request of the patient, and pathologies secondary to a first surgery are situations that have been added to the maternal, placental, and fetal indications that are ordinarily taken into account to perform a cesarean section5.
With this scenario, it is possible that the number and nature of complications during cesarean section also have some change compared to previous reports, particularly when the cesarean section is repeated one or more times6. Possible complications during caesarean section have been known for decades, including bleeding in the layer of the surgical bed, bleeding from the hysterotomy commissures, uterine infiltration, hematomas, accidental damage to arterial or venous vascular structures, injuries to the ureters, urinary bladder, and intestines7. Liver rupture during manual revision of the gland and splenic tear are rare or infrequent complications, but they can occur. In any case, all of them can force a subsequent intervention.
Surgical reintervention is a relatively frequent entity that is usually derived from a first surgical procedure that could have been unsatisfactory that detected a problem that was not resolved due to the hemodynamic or ventilatory conditions of the patient, due to post-surgical complications derived from intrinsic factors and/or extrinsic and even due to deficiencies in the surgical technique itself. A new operation constitutes an extra trauma with greater possibilities of imbalance of the patient’s homeostatic mechanisms, increased complications and higher mortality8-10. In addition, the number of reinterventions is part of the parameters used to evaluate the quality and efficiency of hospital services11. The objective of this research is to identify the prevalence, causes, and clinical course of patients with surgical reintervention due to complications during cesarean section.
Materials and methods
This is an observational, longitudinal, retrospective, retrolective, and descriptive study in a series of cases. The admission record to the Toco-surgery Unit of the Gynecology-Obstetrics Hospital No. 3 of the National Medical Center “La Raza” of the Mexican Institute of Social Security Mexico City was reviewed to know the total number of patients undergoing cesarean section in the period from January to December 2019. Patients who were reoperated due to complications during cesarean section were selected. Routinely, after their reintervention, all the patients were admitted to the intensive care unit (ICU) for surveillance and were later transferred to a general ward. The files were consulted to document general data, the cause of reinterventions, their clinical course, ICU stay, hospital stay, and mortality. Before conducting the study, authorization was obtained from the local Health Research and Health Research Ethics Committees (Registration R-2019-3504-11). Data were analyzed with descriptive statistical measures (mean, median, standard deviation, and range) using the statistical program SPSS version 20.
Results
It was found that during the year 2019, the cesarean section was performed on 3371 patients, of which 1.60% (54 cases) underwent a surgical reintervention, which were the subjects of the present study. Their mean age was 32.12 years and parity 3 with a pregnancy of 35 ± 3.5 weeks. The following comorbidities were found: Overweight 64.81% (35 cases), previous pregnancy with placenta previa 44.4% (24 cases), history of severe pre-eclampsia 20.37% (11 cases), type 1 diabetes mellitus 14.81% (8 cases), primary hypothyroidism 7.4% (4 cases), exogenous grade I obesity 7.4% (4 cases), previous pregnancy with HELLP syndrome 5.5% (3 cases), uterine myomatosis 3.7% (2 cases), congenital scoliosis 1.85% (1 case), exogenous obesity Grade II 1.85% (1 case), chronic systemic arterial hypertension 1.85% (1 case), and primary antiphospholipid antibody syndrome 1.85% (1 case). It was found that 51.85% of the patients had a previous cesarean section (28 cases) and 18.52% had two previous cesarean sections (10 cases). For 29.63% of the patients, the cesarean section was their first surgery (16 cases).
The indications for cesarean section in the 54 patients studied had the following distribution: Placental alterations 53.70% (29 cases), unreliable fetal status 27.78% (15 cases), and maternal indications 18.52% (10 cases). In no case was the cesarean section performed by the doctor’s preference or at the request of the patient. Complications during cesarean section that required reintervention were related to bleeding 94.45% (51 cases) followed by urinary bladder injuries 3.70% (2 cases) and large intestine injury 1.85% (1 case). Figure 1 in turn, the distribution of complications related to bleeding was as follows; Surgical bed bleeding 27.79% (15 cases), obstetric hemorrhage 20.37% (11 cases), persistent bleeding due to uterine atony 20.37% (11 cases), hemorrhage from a hysterotomy commissure 18.52% (10 cases), uterine infiltration 3.70% (2 cases), and bleeding due to accidental injury of a uterine artery 3.70% (2 cases). In all cases, the complications were corrected by performing only one reintervention table 1.
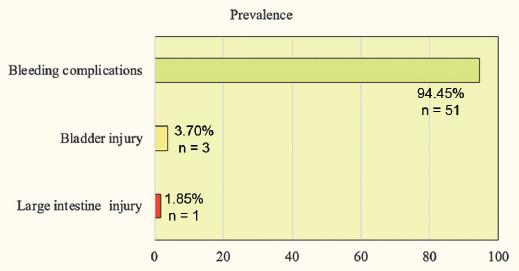
Table 1 Complications during cesarean section, prevalence, and reintervention in 54 patients
| Complications during cesarean section | Prevalence | Number of cases | Reintervention technique |
|---|---|---|---|
| Bleeding complications | 94.45 | 51 | |
| Of the surgical bed | 27.79 | 15 | Unpacking |
| Obstetric hemorrhage | 20.37 | 11 | Local hemostasis |
| Uterine atony | 20.37 | 11 | Hysterectomy |
| Commissure hemorrhage | 18.52 | 10 | Local suture |
| Uterine infiltration | 3.70 | 2 | Hysterectomy |
| Vascular injury | 3.70 | 2 | Uterine artery ligation |
| Bladder injury | 3.70 | 2 | Primary closure |
| Large intestine injury | 1.85 | 1 | Primary closure |
| Total | 100 | 54 |
The mean stay in the ICU was 3.79 ± 2.03 days and in the hospital was 13.67 ± 11.16 days. There were no patients transferred to other hospitals. Mortality was 1.85% (1 case), and it was a patient with an urgent cesarean section indicated for severe pre-eclampsia with HELLP syndrome and a bleeding ruptured hepatic hematoma that was managed during surgery with the Pringle maneuver, packing, and closure of the abdominal cavity. This patient had to undergo immediate surgical reintervention due to persistent bleeding that was uncontrollable and progressed to Class IV hypovolemic hemorrhagic shock, cardiorespiratory arrest, and death in the operating room.
Discussion
3371 women who underwent cesarean section in 2019 were studied. It was found that the prevalence of patients with reintervention due to complications during surgery was 1.60% (54 cases), a very low figure compared to data from series from other countries such as Holland 19977, Brazil 200412, Sudan 201413, and India 201614. As can be seen in table 2, the number of cases studied in this investigation is greater than the number of patients in any of the other series. It also highlights that the highest frequency of complications during cesarean section corresponds to the report by Umbeli et al.13 in patients from Sudan 49.80% and that the lowest frequency was that of our study. The data from this series showed that the main complications that led to reintervention were hemorrhagic, followed by bladder injury and colonic injury with very low percentages. Thus, the causes were not different from the type of intraoperative complications identified in previous reports7,12-14.
Table 2 Historical comparison of the prevalence of complications during cesarean section
| Author, country and year | Cases | Complications | |
|---|---|---|---|
| Prevalence | Type | ||
| Van Ham et al.7 Holland (1997) | 2,647 | 14.8% | Uterine laceration 10.1% Hemorrhage > 1,000 cc 4% Others 0.7% |
| Nomura et al.12 Brazil (2004) | 998 | 13.8% | Extend of hysterorrhaphy 7% Obstetric hemorrhage 6% Uterine atony 0.7% Bladder injury 0.1% |
| Umbeli et al.13 Sudan (2014) | 470 | 49.8% | Obstetric hemorrhage 23.1% Extended of hysterorrhaphy 22.7% Intestine injury 2.8% Bladder injury 0.6% Ureteral injury 0.2% |
| Jain et al.14 India (2016) | 1,349 | 2.5% | Obstetric hemorrhage 1.3% Extended of hysterorrhaphy 0.9% Uterine infiltration 0.3% |
| Vázquez et al.15 México (2019) Current study | 3,371 | 1.60% n 54* | Bleeding from the surgical bed 0.44%, n 15 Obstetric hemorrhage 0.33%, n 11 Uterine atony 0.33%, n 11 Commissure hemorrhage 0.29%, n 10 Uterine infiltration 0.060%, n 2 Accidental arterial injury 0.060%, n 2 Bladder injury 0.060%, n 2 Large intestine injury 0.030%, n 1 |
*The data are shown as the percentage and number of cases (n) for each type of complication since they are very small fractions.
The stay in the ICU of the 54 patients studied was similar to the average of other patients in the same highly specialized center, but the hospital stay was longer15. These data could have been a consequence of the longer post-surgical recovery time in a general ward, but not in the ICU, which imply a rapid recovery from his critical condition. Mortality in our series was very low (1.85%), and it was a patient with severe pre-eclampsia and HELLP syndrome with massive bleeding due to a ruptured hepatic hematoma, a situation of extreme severity, and poor prognosis in any scenario. In general, the data support the opinion that the clinical course of the patients studied was successful.
Finally, the following comments are pertinent. The data presented here correspond to patients from a highly specialized medical unit that concentrates the most complicated cases of high-risk pregnancy in Mexico City and the central zone of the country and does not necessarily have a general representativeness. The hospital that hosts this research belongs to an institution affiliated with the Mexican health sector (Mexican Institute of Social Security), so in no case was the cesarean section performed due to the doctor’s preference for the method or at the request of the patient. In addition, the casuistry corresponds to the year 2019, which represents the last regular year before the COVID-19 pandemic, a disease that changed the routine of humanity, so the frequency of cesarean sections may possibly be different due to the effect of viral illness such as a maternal factor, due to deterioration of the fetal state, due to the preference of the medical staff, or due to the express request of the patient. Thus, the reports on the frequency of the cesarean section and its intraoperative complications in times of the COVID-19 pandemic and after it will be relevant because they can show different results.

