











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Hemorrhoidal disease (HD) is a common anorectal condition consisting of asymptomatic enlargement and distal displacement of the typical anal cushions. Multiple factors are involved in HD development, including constipation and prolonged straining. The abnormal dilatation and distortion of the vascular channel, together with destructive changes in the supporting connective tissue within the anal cushion, is a paramount finding of the disease1. The anal cushions or hemorrhoids are healthy tissue inside the anal canal and are part of the internal hemorrhoidal plexus. There is also an external plexus from which external hemorrhoids come. The anatomical boundary that divides the internal from the external hemorrhoidal plexus is the dentate line2. Prolapsed hemorrhoids can achieve an overlap between internal and external, determining a new morphological appearance (mixed or only internal hemorrhoids) in which the anatomical subdivision between the two plexuses is theoretically correct but clinically not useful since the HD can manifest itself with prolapse of different degrees, bleeding, and pain3.
The pathophysiology of the HD is complex. The most widely accepted theory is a sliding anal canal, or cushion theory, which refers to the abnormal sliding of the cushions through the anal canal as the main pathophysiological event caused by increased abdominal pressure and a decreased venous return during defecation (constipation)2. Increased matrix metalloproteinases activity leads to increasing cushion congestion, and the supporting capacity of the vascular network is lost4. Aigner et al. suggested that a specialized vascular network is capable of controlling the filling and emptying of the anorectal vascular plexus, such as a sphincter. The disruption of this system due to changes present in the connective tissue is another cause of the disease5. The inflammatory process leads to erosion of the hemorrhoidal arterioles during defecation causing bleeding. Thrombosis leads to ischemia, ulceration, and necrosis of the tissue surface1.
Symptoms related to hemorrhoids are prevalent in the western hemisphere and other industrialized societies. The disease represents more than 2.2 million outpatient evaluations per year in the United States6. The HD has a prevalence of 4.4%, with 10 million patients worldwide. In both genders, a peak in prevalence is noted between 45 and 65 years of age7. The development of HD before the age of 20 is unusual, and Caucasians are affected more frequently than are African-Americans8,9. The real prevalence in Latin America is hard to estimate because we do not have real data to compare with information over the world. However, we can suppose by the similarities of the western dietary habits that we have similar cases in our environment10. Charúa-Guindic et al. reported that 30% of the colorectal consultation in our third level medical center in Mexico corresponds to HD, affecting both genres. The exact data are not available, but at least 5% of the adult Mexican population is affected (similar to that observed in the rest of the world)11-13.
A total of 40% of individuals with HD are asymptomatic. For internal hemorrhoids, bright red bleeding is the most commonly reported symptom. Another frequent symptom is the sensation of tissue prolapse and occasionally presents with secondary pain14,15. Anemia is not that rare, but it is important to identify the bleeding source before considering hemorrhoids. We recommend performing anoscopy and proctosigmoidoscopy in the office to rule out other causes of painless rectal bleeding6. When there are doubts, complete colonoscopy is indicated and should always precede surgery, especially in patients over 45 years of age16,17.
We usually use the Goligher classification for HD. The importance lies in the fact that the treatment depends on the degree and severity of the HD18. The common indications for intervention in patients with hemorrhoids include bleeding and prolapse. In patients who remain symptomatic despite conservative management, surgical treatment should be offered. An excisional hemorrhoidectomy is the best treatment for patients with large symptomatic external hemorrhoids and internal prolapsed internal hemorrhoids (Grade IV)17.
Information regarding emergency treatment for hemorrhoidal bleeding is very scarce. We must differentiate active hemorrhoidal bleeding (Fig. 1) from the so-called hemorrhoidal crisis where severe pain, bleeding, irreducible prolapse, or hemorrhoidal gangrene occur (Fig. 2)17,19. Non-surgical management of acutely thrombosed, ulcerated, or strangulated prolapsed hemorrhoids is widely employed because emergency hemorrhoidectomy (EH) is said to be associated with portal abscesses, secondary hemorrhage, anal stenosis, and incontinence. However, several studies have shown that EH is safe and is a suitable way of managing acutely ulcerated or gangrenous prolapsed thrombosed hemorrhoids20. Surgical options include hemorrhoidectomy, Doppler-guided hemorrhoidal artery ligation, and stapled hemorrhoidopexy21.


The objectives of the study are to describe the clinical and surgical characteristics of patients with HD and active bleeding in need of urgent surgery.
Methods
It is a descriptive, retrospective study of 510 patients at the General Hospital of Mexico between 2015 and 2019. Male and female patients (aged > 18 years) diagnosed with HD admitted to the colorectal surgery service. The records of these patients were reviewed, and we identified those who underwent emergency surgery due to active bleeding, anemia, shock, and other clinical problems. All the patients received an evaluation in the office by a colorectal surgeon. Those over 45 years of age had a complete colonoscopy as a study for detecting colorectal cancer. All patients underwent pre-operative studies that included complete blood count, basic metabolic panel, and prothrombin time and activated partial thromboplastin time. Those patients who, in addition to bleeding, had another type of anorectal disease, such as anal fistula, fissures, and infections, were not included.
The HD was classified according to Goligher classification:
– Bleeding without prolapse (first degree)
– Bleeding with prolapse that reduces spontaneously (second-degree hemorrhoids)
– Bleeding in conjunction with hemorrhoids that prolapse and manually reduced (third degree)
– Prolapsed internal hemorrhoids that cannot be reduced (fourth degree).
We also included patients with mixed HD and hemorrhoidal thrombosis.
The degree of anemia was classified according to the classification of the World Health Organization (WHO): Grade 0 or normal (> 11 g/dl); Grade 1 or mild (9.5-10.9 g/dl); Grade 2 or moderate (8-9.4 g/dl); Grade 3 or severe (6.5-7.9 g/dl); and Grade 4 or life threatening (< 6.5 g/dl).
Through a descriptive study with the use of means and medians, quantitative and qualitative variables were studied. Statistical analysis was carried out with the SPSS version 24 software.
Results
A total of 510 patients with HD were included. About 10.3% (53) met the criteria for presenting active hemorrhoidal bleeding at the time of review and clinical and biochemical data of anemia. All of these patients underwent urgent surgery within 48 h of hospitalization (Fig. 3).
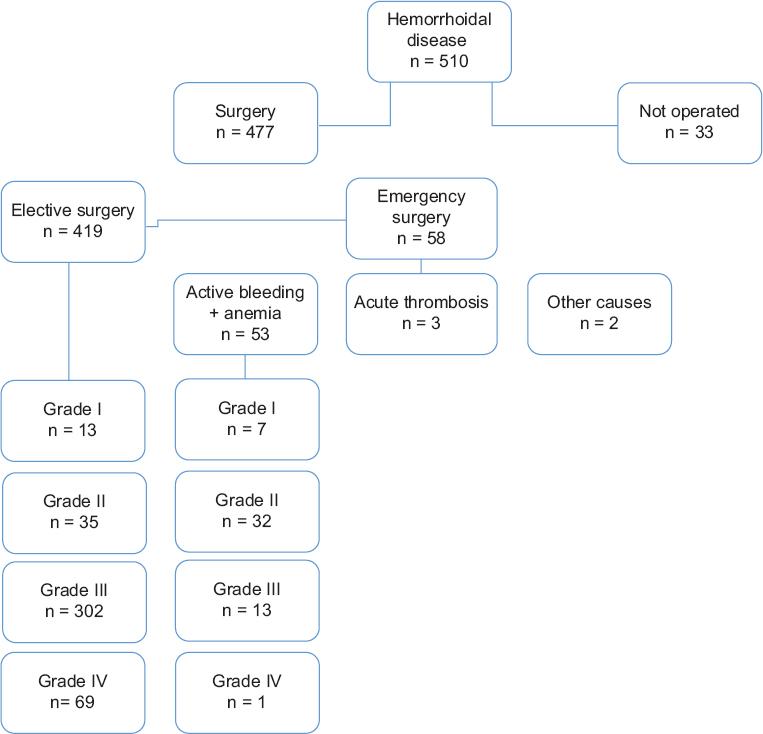
Figure 3 Characteristics and number of patients with different grades and presentation of hemorrhoidal disease.
About 39.6% (21) of the patients were female and 60.3% (32) were male. The mean age was 45 years old. About 52.8% (28) of the patients were older than 45 years, so they were taken to a diagnostic colonoscopy before surgery to rule out malignancy.
About 96.2% (51) of the patients presented internal HD and 3.7% (2) of the patients were classified as a mixed HD (internal and external component). Patients were classified according to the degree of HD as follows: Grade (I) 13.2% (7); Grade (II) 60.3% (32); Grade (III) 24.5% (13); and Grade (IV) 1.8% (1).
About 9.4% (5) presented hypovolemic shock at the time of hospitalization. All patients presented different degrees of anemia according to the WHO classification, with mean hemoglobin of 7.5 g/dl. About 79.2% (42) of the patients received a blood transfusion, while the remaining 20.8% (11) did not receive transfusion after consideration of the attending physician at the time of admission.
Among the accompanying diseases observed, 3.8% (2) of the patients had type 2 diabetes and another 3.8% had obesity. The rest of the patients did not have documented comorbidities.
The treatment received in 92.5% (49) of the cases was hemorrhoidectomy with the Ferguson technique; in 5.7% (3), a hemorrhoidectomy was performed with an advanced energy device, and 1.9% (1) underwent the Milligan-Morgan technique. It was not necessary to perform another type of surgical procedure in any case. The average length of stay was 3.1 days (SD 1.56). About 5.7% (3) of the patients presented post-operative bleeding in the first 24 h after surgery, which was resolved again in the operating room by applying hemostatic suture
About 41.5% (22) of patients never received treatment for HD before the surgery. The remaining patients received the following treatments before surgery: (1) 34% (18) had a history of receiving medical treatment (e.g., diet, fiber, etc.); (2) in 11.3% (6), a rubber band ligation was performed; (3) 7.5% (4) received sclerotherapy, and (4) 1.9% (1) had previously undergone hemorrhoidectomy at another hospital.
Discussion
It is essential to point out that there is no study evaluating the safety and feasibility of carrying out emergency hemorrhoidal surgery in massive bleeding cases. Research in the treatment of emergency HD generally focuses on thrombosis and the application of different techniques for its treatment17,19,21-23, however, there is not a study of EH in patients with severe active bleeding despite being a situation that is frequently observed in specialized services. In these types of cases, EH allows us to resolve the hemorrhoidal symptoms themselves and secondary anemia immediately20.
No statistically significant difference was found between the different degrees of HD and the patient's age, which means that regardless of the patient's age, it is possible to safely operate on the technique with a low percentage of complications. Yamamoto et al. and Haksal et al.'s work shows that hemorrhoidal surgery does not represent a higher surgical risk in elderly patients compared to younger patients24,25 (Fig. 4).
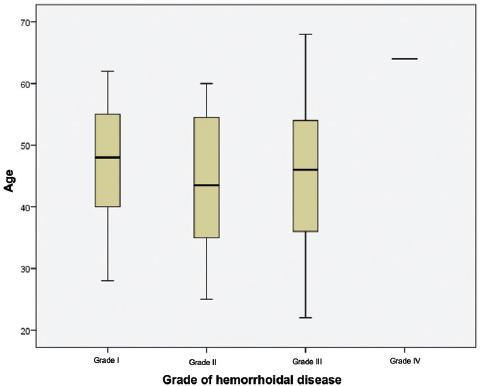
Figure 4 Grade of hemorrhoidal disease compared with the age of patients. The age of the patient is not a determining factor in making decisions to operate urgently on a patient with active hemorrhoidal bleeding.
There is no relationship between the length of hospital stay and the age of the patients. EH for active bleeding is safe for all patients since there were no significant complications that prolonged the stay (R of 0.002). Neither did we find a relationship between the length of stay and degree of HD, which also translates into safety and reliability in offering surgical treatment and is comparable to that reported by other authors17,25 (Fig. 5).
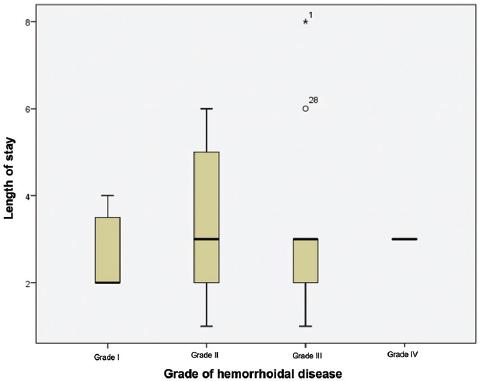
Figure 5 Grade of hemorrhoidal disease compared with the length of hospital stay. Emergency hemorrhoidectomy is as safe as elective surgery since there is no significant difference in the length of hospital stay.
Although there is no significant difference between the degrees of hemoglobin concerning the degree of HD, patients with Grade II disease tend to have a higher degree of anemia. There is no relationship between the patient's age and active bleeding (Fig. 6).
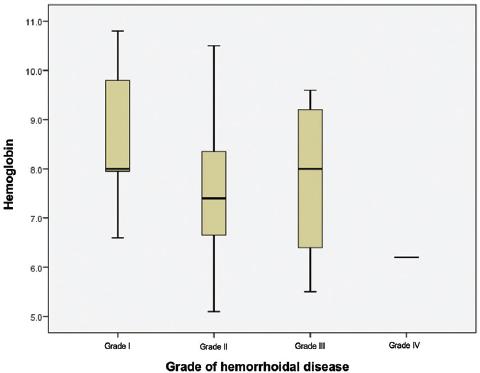
Figure 6 Grade of hemorrhoidal disease compared with the level of hemoglobin. The amount of hemoglobin does not translate into more serious disease. Most of the cases of active hemorrhoidal bleeding with anemia were grade II.
HD is not a rare cause of anemia; however, this finding is underdiagnosed and rarely reported, so there is no real incidence. At least in our hospital, this phenomenon is observed frequently (average Hb of 7.75 g/dl) and is similar to that reported by Kluiber and Wolff (average Hb of 9.4 g/dl)26. In general, these patients will require transfusion and surgery as soon as possible. All patients with lower digestive bleeding and anemia require a complete review before starting to manage the HD. In our study, all patients older than 45 years of age had a colonoscopy. Unlike what was reported in the literature, in our study, the percentage of patients with comorbidities was very low because the mean age identified was 45 years, and the screening for diabetes was not intentionally done in patients who did not have this precedent, because it was an acute presentation of HD. Therefore, it would be important to report these data in a complementary study to this one.
EH has not always been accepted due to possible secondary infection, high risk of anal bleeding and stenosis, incontinence, and recurrence of the disease. Furthermore, hemorrhoidectomy in these cases is usually more difficult due to the size of the packages, edema, and tissue necrosis. Mazier, in a 1973 study of 400 emergency surgery with closed hemorrhoidectomy to treat thrombosis, observed good results with few complications27. All patients with associated anal disease were excluded for a better validation of the data obtained, so no other surgical procedure not related to hemorrhoidectomy was performed. In a 204 emergency procedures study20, it was shown that the incidence of complications was not higher than that occurring in elective surgery. Similar results are observed in the study of Ceulemans et al.23. There is also no difference in the incidence of recurrence of HD. There are numerous advantages, such as offering a definitive treatment without requiring further management and avoiding the discomfort of conservative management19. Conventional closed hemorrhoidectomy is the most preferred treatment due to the few complications and low recurrence it presents28,29.
Ultrasound studies have been carried out, given the possibility of damage to the anal sphincter after emergency hemorrhoidal surgery30. The results show that when there are lesions, they are usually asymptomatic or have a lower degree of incontinence (generally flatus) and with an incidence no higher than that presented in elective surgery. Studies performed in surgery with the procedure for prolapsing hemorrhoids technique have shown to be a suitable option19, but unfortunately, we do not have this device regularly in our service. The use of ultrasonic energy instruments such as the LigaSure™ Vessel Sealing System (Medtronic-Covidien) or Harmonic Scalpel™ (Harmonic Focus; Ethicon, Johnson and Johnson) has proven to be safe and comfortable to use element in EH offering less post-operative pain, fast recovery, and fewer complications31 but they are not within reach of all patients due to their high cost.
Active bleeding can be treated by applying hemostats and cauterization in the office when it is impossible to take the patient to the operating room22. However, these measures only resolve the problem temporarily. Surgery is the definitive treatment. In this study, a follow-up was performed 12 months after surgery and no recurrence of rectal bleeding or hemorrhoidal symptoms was identified. According to the literature, once the surgical procedure is performed with the ideal surgical technique depending on the degree of HD, the complete remission of the symptoms associated with this disease is effectively achieved. With timely treatment, anemia and hemorrhoidal symptoms can be resolved permanently26. The patients operated on most frequently in our study correspond to cases of Grade II HD since it is these patients that are generally managed with conservative treatment, while patients with Grades III or IV are scheduled for surgery regularly.
The limitations of our study are (1) variability of the hemorrhoidectomy technique, (2) different colorectal surgeons, and (3) different criteria in deciding for pre-operative management. Our institution is a teaching hospital; residents of the specialty perform about 30% of hemorrhoidectomies. It is necessary to carry out a clinical trial that allows us to analyze the specific characteristics of patients who present massive hemorrhoidal bleeding. On the other hand, studies can be carried out to analyze the histological structure of the hemorrhoidal packages that present higher bleeding to compare them with patients with a lesser degree of bleeding. In the study by Serra et al., it was found that matrix metalloproteinases and neutrophil gelatinase-associated lipocalin can be useful as molecular markers in the evaluation of HD and determine the risk of developing a more severe form of the disease4.

