











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
In December 2019, an outbreak of the 2019 coronavirus (COVID-19) caused by SARS coronavirus 2 (SARS-CoV-2) occurred in Wuhan, China1,2; spreading worldwide3, with WHO declaring a COVID-19 pandemic on March 20203.
The COVID-19 pandemic has stressed every health system in the world. The impact on the surgical services has been profound and one of the first responses was to cease all non-essential surgical operations. Some elective surgery for time-sensitive conditions continued with prioritization of patients with resectable cancers at risk for progression and patients for whom alternative treatment modalities would be ineffective4,5.
Patients undergoing surgery are at risk of SARS-CoV-2 exposure in the hospital. They are particularly susceptible to pulmonary complications, due to pro-inflammatory cytokines, immunosuppressive response to surgery, and mechanical ventilation. Morbidity and mortality in COVID-19 patients are higher than patients without COVID-196-8.
Data on the effects of COVID-19 on surgical hepato-pancreato-biliary diseases (HPB) is yet to be fully reported. HPB centers worldwide have reported a reduction their surgical procedures4,5. Reported outcomes in HPB surgery during this pandemic are scarce9-11.
The impact of the virus in different health-care systems is of great interest in surgery, particularly on HPB surgery4,5,12-14. Such a scenario necessitates a snapshot of the management of HPB surgery. Therefore, the Mexican Hepato-Pancreato-Biliary Association (AMHPB) created and conducted a survey, aiming to gather the experience and opinions of HPB surgeons in Latin America to allow comparisons of healthcare, practice, and patient safety to identify chances for improvement and collaboration.
Methods
Survey
An online survey was distributed by email invitation to all members of the Mexican Hepato-Pancreato-Biliary Association(AMHPB) and attendees of the three previous Congresses of the Society (2017-2020) through a self-administered electronicquestionnaire(https://docs.google.com/forms/d/1qbp6stuXCWgvcKAuyr068DthM3FWcOsuctZiHbSFoHA/edit) developed by the survey administration application Google Forms (Google LCC, Mountain View, California, USA) (Supplementary material).
The survey consisted of 33 items based on demographics, preoperative COVID-19 triage/screening and COVID-19 hospital occupancy, patient referral, surgical practice (case volume and outcomes), and COVID-19 limitations/restrictions (surgical cancellations). Respondents were asked to register their names and institutions to prevent duplicate data. Answers were excluded if respondents were not from Latin America. Respondents were asked if they performed one of the following HPB procedures: (Liver resection/Liver transplantation; pancreatoduodenectomy/subtotal pancreatectomy/distal pancreatectomy/surgical procedures related to acute/chronic pancreatitis; choledochal cyst/bile duct resection/repair; and other hepato-pancreato-biliary procedures). Data were not included if the respondents did not perform any of the aforementioned procedures. No minimal cutoff in HPB surgical volume was established to enter the survey. A manual search was performed to find duplicate data. If duplicate data were found, the first fully answered questionnaire was given priority. Questions were open questions, closed-ended questions, or multiple-choice questions allowing the possibility to choose multiple answers. The survey was open for 2 months (April-May/2020) with regular reminders every 2 weeks.
Results
Demographics
After excluding 26 responses (three responses were discarded since the respondents did not perform any of the listed hepato-pancreato-biliary procedures and 23 were duplicated response data) a total of 88 participants were included for analysis. The mean age of the respondents was 47.5 ± 10 years (32-76 range). The majority were male (94.3%, n = 83), and 65.9% (n = 58) were Mexicans and the rest from other Latin American countries. Figure 1 shows the geographical distribution of survey responses across Mexico and Latin America.

Sixty-four respondents were working in both public and private hospitals (n = 64, 72.7%), 20.5% (n = 18) were working in private hospitals only, and 6 respondents (6.8%) in public hospitals only. Most of the respondents (n = 78, 90.9%) were working in an academic center (either public/private hospitals with medical students/residents/fellows). Twenty-nine (29.5%, n = 26) of the respondents were chief of department/division and the rest (n = 62, 70.5%) were attending. Then mean years of surgical practice were 14.9 ± 11.2 years (1-45 range).
Pre-operative COVID-19 triage/screening and COVID-19 hospital occupancy
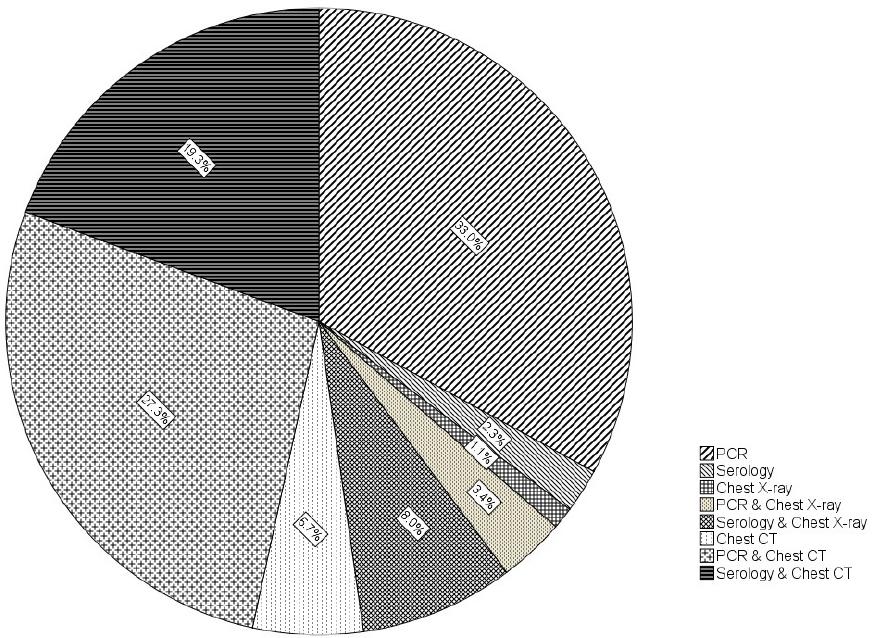
During 2020, seven respondents (8%) were working in COVID-19 converted hospitals, nine respondents (10.2%) were working in non-COVID-19 hospitals, and 72 respondents (81.8%) were working in hospitals with COVID-19 dedicated areas. Only one respondent (1.1%) did not routinely perform preoperative COVID-19 testing, 20 respondents (22.7%) only in patients with respiratory symptoms or SARS-CoV-2 suspected infection, and 76.1% (n = 67) respondents to all patients. The most common COVID-19 pre-operative testing strategy was polymerase chain reaction (PCR) (33%) followed by PCR and Chest CT (27.3%). Figure 2 display all COVID-19 preoperative testing strategies.
Patient reference and HPB surgical practice
According to the respondents, the number of patient referrals decreased 62.5% (n = 65) during 2020; 27.3% (n = 24) responded that patient referral was the same and 10.2% (n = 9) claimed that patient referrals increased. Thirty-six percent (36.4%, n = 32) of the respondents could not finish some of their patient´s surgical evaluations and preoperative workup. Sixty respondents (72.7%, n = 60) had at least one patient who developed COVID-19 infection during surgical evaluation and preoperative workup (4.8 ± 6.6 patients). 26 respondents (29.5%) had at least one patient who died from COVID-19 while surgical evaluation and pre-operative workup were performed.
Forty-six respondents (52.3%) reported that they changed their preoperative workup in their procedures and the most common change was COVID-19 testing/screening (67.4%) followed by changes in hospitalization routes (17.4%).
The mean surgical case volume performed by the respondent before 2020 was 47.7 ± 47.5 (1-250 range). The most common type of surgical procedure performed by the respondents was biliary in45.4% (n = 40). In 2020, 64.7% of the respondents (n = 57) answered that their surgical case volume decreased. The mean estimated decreased percentage was 52.5 ± 20.4%. Fourteen respondents (n = 14, 15.9%) answered that their surgical case volume increased by a mean estimated percentage of 29.6 ± 20.5%. Respondents who were working in both public and private hospitals (n = 64) answered that changes in their practice were in hospitals where they have their busiest practice (38.6%) and in both hospitals in which they worked (public/private) (37.5%). Figure 3 details HPB surgical case volume and volume changes.

Based on their answers, 72.7% of the respondents (n = 64) considered that the surgical morbidity of their HPB surgical practice stayed equal to prior years, 15 respondents (17%) considered that their surgical morbidity increased and 10.2% (n = 9) considered that their surgical morbidity decreased. Reasons related to hospital area and resources were the most common causes of morbidity changes (increase/decrease) according to the respondents (Fig. 4).
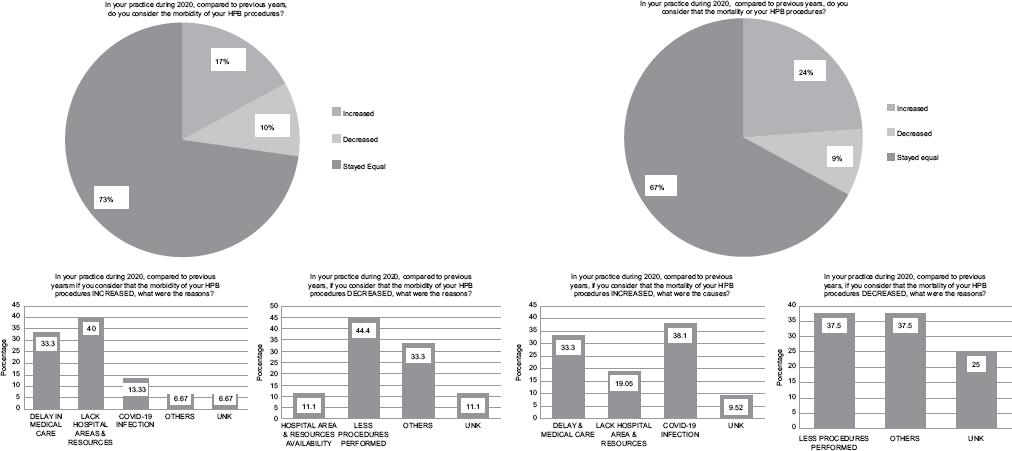
Sixty-seven (67%) of the respondents (n = 59) considered that the surgical mortality of their HPB surgical practice stayed equal to prior years, 21 respondents (23.9%) considered that their surgical mortality increased and 9.1% (n = 8) considered that their surgical mortality decreased. COVID-19 infection was the most common cause of increased HPB surgical mortality, based on the respondent’s answers. The reasons to which the respondents attributed their changes in HPB surgical morbidity and mortality were grouped and exemplified in figure 4.
In 2020, 46.6% of the respondents (n = 41) had at least one patient who underwent an HPB procedure who developed postoperative COVID-19 infection. According to their answers, 53.7% of the patients who underwent an HPB procedure who developed post-operative COVID-19 infection had an uneventful postoperative course besides COVID-19 infection, 17.1% had a complication related to COVID-19 infection, and 24.4% died because of COVID-19 infection.
COVID-19 limitations/restrictions on HPB surgical practice (cancelled surgeries)
The most common cause of HPB cancelled surgeries was a decrease in ICU capacity (beds) in 54% of the cases, followed by hospital policy in 42%. Table 1 shows all answered reasons for HPB surgical cancellations during 2020.
Table 1 Causes of HPB surgical cases cancellation
| Item | Total (n = 234) Percentage |
|---|---|
| Lack of ICU bed | (48) 20.5% |
| Hospital Policy | (37) 15.8% |
| Patient declined surgery | (33) 13.9% |
| Lack of OR capacity | (25) 10.6% |
| Lack of OR personnel | (25) 10.6% |
| Country policy | (20) 8.4% |
| Lack of Blood Products | (18) 7.5% |
| Patient fear for COVID-19 infection | (13) 5.5% |
| Lack of In-Hospital personnel | (11) 4.7% |
| Others | (4) 1.7% |
ICU: intensive care unit; OR: operating room.
Discussion
The results of this survey evidence the significant negative impact of COVID-19 in HPB surgery practice during 2020 in Mexico and Latin America. In most of the cases (above 50%), there was an important decrease in patient reference. The preoperative surgical evaluation and workup suffered delays and cancellation due to COVID-19 patient´s infection and death, and subsequently, the surgical case volume dropped. HPB surgeons quickly adapted to COVID-19 pre-operative screening and testing. Surgical morbidity and mortality increased during the midst of the pandemic and finally, most of the surgical cancellations/restrictions were hospital-related (lack of hospital facilities, hospital policy, and lack of personnel).
A retrospective view of the ongoing COVID-19 pandemic showed an initial cancellation of all elective surgical activities worldwide, and HPB surgery was not the exception. This cancellation generated a backward influence in the reference of patients, as two different surveys conducted in Europe described, in which patient reference dropped 60%-90% in all HPB centers across the continent4,5,12. Only few centers (10%) considered that their reference stayed equal and some brief reports described an increased number of HPB procedures performed11. The results of this survey tell us that patient reference similarly decreased in our continent as occurred in Europe; however, we encountered 10% of HPB surgeons stating that their actual patient reference increased. This number is similar to the number of HPB who worked in 2020 in non-COVID-19 hospitals, raising the chance that these were the HPB surgeons who increased their patient referrals as well. In addition to a slow down pace of patient reference, the patient´s COVID-19 infection during surgical evaluation and pre-operative work-up, resulted in a reduction of the surgical case volume in most of the cases. Furthermore, there was not a specific pattern in terms of a particular type of HPB procedure that changed (either decrease or increase) during 2020.
Studies assessing delays in HPB surgery during the first COVID-19 wave showed that patients waited more days for surgery than usual and predictors referral pathway, and presenting pathology15. In the case of hepatocellular carcinoma, the first wave of the COVID-19 pandemic had a tremendous impact on the routine care of patients. Modifications in screening, diagnostic, and treatment algorithms significantly impaired the outcome of patients16. Cancer surgery systems worldwide were fragile to lockdowns, with one in seven patients who were in regions with full lockdowns not undergoing planned surgery and experiencing longer preoperative delays17.
The results of the survey state that the majority of HPB surgeons in Mexico and Latin America performed some sort of preoperative COVID-19 screening and testing. This is similar to several surveys such as the Italian survey focused on minimally invasive HPB surgery that reported an 87% COVID-19 patient screening12, the European-African Hepato-Pancreato-Biliary Association survey of HPB surgery that informed that 35% of the participants did not perform any COVID-19 testing5 and the global survey conducted by 7 international pancreatic associations and study groups on pancreatic surgery during the COVID-19 pandemic in which they described that 87% of the participants screened their patients for COVID-1913, and had a 75% agreement that COVID-19 preoperative testing/screening is recommended but not mandatory13. COVID-19 PCR (nasal swab) and chest CT was the most common testing strategy in our study, which is the most common test, performed either individually or in combination in different places4,5,12-14 in almost the same proportion (40%).
The survey results suggest that the morbidity and mortality of HPB surgery raised during 2020 (around 20%) was attributable to COVID-19 infection and directly related COVID-19 causes, such as lack of hospital areas and resources as well. It is well known that COVID-19 infection increases surgical morbidity and mortality6-8. Nevertheless, some initial experiences on HPB procedures did not describe augmented morbidity and mortality9-11; although they are small single-center series, which permits to think that the smaller number of procedures performed, less morbidity and mortality will occur (one of the answers in our survey about why morbidity and mortality on HPB procedures did not change according to the respondents). Finally, the analysis of the survey regarding surgical cancellations reveals an indirect problem, such as hospital overcrowding, with limited personnel, in limited resources countries regarding supplies availability to handle health-care challenges during the COVID-19 pandemic.
The major drawback of the study is the low survey responses, which offers limitations to the data and conclusions collected and obtained in a single shot survey. Nevertheless, the low response rate leaves blank the fact that impact of COVID-19 in HPB surgery could have been worse instead. Despite the aforementioned limitation, several issues merit attention after reading the results of this survey: i) A consensus should be made to support the mandatory routine testing of patients to reduce potential complications of surgery regarding COVID-19 infection in HPB surgery in the new COVID-19 era; ii) a clear guidance on the prioritization of HPB treatments depending upon the availability of local resources and regional infection rates should be established; and iii) a defined strategy should be implemented to restore patient reference and surgical evaluations in HPB centers.
Conclusion
COVID-19 had a negative impact on HPB surgery in Mexico and Latin America. There is an urgent need for new strategies, guidelines, and consensus to revert this impact.
Supplementary data
Supplementary data are available at Cirugía y Cirujanos online DOI: https://10.24875/CIRU.22000063. These data are provided by the corresponding author and published online for the benefit of the reader. The contents of supplementary data are the sole responsibility of the authors.

