











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Gunshot-induced spinal cord injuries (GSISCI) have become increasingly frequent in the civilian population. Globally, these injuries have become a public health problem because they significantly impair a patient’s quality of life, functional status, and social independence.
In the United States, each year near 30,000 to 50,000 people die secondary to gunshot wounds (GSWs) and they represent the first cause of death in the first two decades of life; In addition, it is estimated that for each death there are at least three disabling gunshot wounds1,2. Spinal cord injury (SCI) is one of the catastrophic consequences of GSWs. They represent the third most common cause of SCI, after motor vehicle accidents and falls from height representing 43% and 13%, respectively.
As of 2011, there was a significant increase in violence in the city of Monterrey (Nuevo León, Mexico)3,4. With this increase, the epidemiology of the emergency services in our city took a turn an unexpected that resulted in an increase in the admission of patients with gunshot injuries.
Treatment requires significant health-care resources and places a financial burden on patients, their families, and the community. These high costs are associated with a need for high-level acute care in the short-term along with complication management in the long term5.
Due to the recent increase in the admission of patients with spinal gunshot injuries in our hospital (level III trauma center), the purpose of this study is to report epidemiological and clinical data of the patients that were admitted with spinal gunshot injuries.
Methods
An observational, retrospective study in which patients who had a spinal injury secondary to a gunshot wound that was admitted to our hospital (level III trauma center) from July 2018 to July 2020 were included in the study. A review of medical records and radiological studies of all patients with a spine injury secondary to a gunshot wound was conducted by the authors. Patients with incomplete information were excluded from the study.
Demographic and clinical data including age, gender, civil status, occupation, level of injury (cervical, thoracic, or lumbar), degree of neurological impairment at admission6, associated injuries, treatment established, length of hospital stay, and mortality rate were recorded.
Results
In the years included in the study, a total of 503 fractures (spine and non-spine) secondary to gunshot wounds were admitted to our hospital, of which 55 (10.93%) consisted of vertebral fractures. Fifty-five patients were admitted to our hospital with gunshot injuries to the spine (with and without neurological deficit) from July 2018 to July 2020. No patients were excluded from the study.
A total of 55 patients were included in the study, of which 50 patients (90.9%) were men and five female patients (9.09%). The average age was 30.2 years. Three patients died during hospitalization representing a mortality rate of 5.45%. The causes of death were multi-system organ failure (Table 1).
The thoracic spine had the highest frequency of injury in our series with a total of 26 (47.27%) injuries, 25 (45.45%) lumbar spine injuries, 3 (5.45%) cervical spine injuries, and 1 (1.81%) sacral injury (Table 2).
Table 2 Injury distribution
| Region | n | % |
|---|---|---|
| Cervical | 3 | 5.45 |
| Thoracic | 26 | 47.27 |
| Lumbar | 25 | 44.45 |
| Sacral | 1 | 1.81 |
| Total | 55 |
Thirty patients (54.53%) had neurological deficits at admission of which 2 (3.63%) were cervical spine injuries, 18 (32.72%) were thoracic spine injuries, and 10 (18.18%) were lumbar spine injuries. The patient who had a sacral injury had no neurological injury (Table 3). Of the 30 patients with neurological injury, 29 had a complete injury (ASIA A), and only one patient arrived with an incomplete injury (ASIA B) (Table 4).
Table 3 Neurological injury at admission
| Region | n | % |
|---|---|---|
| Cervical | 2 | 3.63 |
| Thoracic | 18 | 32.72 |
| Lumbar | 10 | 18.18 |
| Sacral | 0 | 0 |
| Total | 30 |
Table 4 Degree of neurological impairment
| Degree of injury | n | % |
|---|---|---|
| Incomplete injury (ASIA B) | 1 | 3.33 |
| Complete injury (ASIA A) | 29 | 96.66 |
| Total | 30 |
Forty-five patients (81.81%) had associated injuries of which two (3.63%) were patients with cervical spine injuries, 24 (43.63%) were patients with thoracic spine injuries, and 19 (34.54%) were patients with lumbar spine injuries (Table 5).
Table 5 Associated injuries
| Region | n | % |
|---|---|---|
| Cervical | 2 | 3.63 |
| Thoracic | 24 | 43.63 |
| Lumbar | 19 | 34.54 |
| Sacral | 0 | 0 |
| Total | 45 |
Twenty-seven patients (49.09%) had only one associated injury, 16 patients (29.09%) had two associated injuries, and only two patients (3.63%) had three associated lesions.
In the cervical spine, the most common associated injury was vertebral artery injury in two cases (4.44%). In the thoracic spine, the most common associated injury was hemopneumothorax with 24 cases (39.34%) and in the lumbar spine the most common associated injury was liver injury with nine cases (14.75%). The patient with a sacral injury did not have associated injuries (Table 6).
Table 6 Overall incidence of associated injuries
| Associated injuries | n | % |
|---|---|---|
| Hemopneumothorax** | 24 | 39.34 |
| Liver*** | 9 | 14.75 |
| Spleen | 7 | 11.47 |
| Fracture | 5 | 8.19 |
| Colon | 5 | 8.19 |
| Small intestine | 3 | 4.91 |
| Renal | 3 | 4.91 |
| Vertebral artery* | 2 | 3.27 |
| Diaphragm | 1 | 1.63 |
| Pharynx | 1 | 1.63 |
| Cava vein | 1 | 1.63 |
*Most common associated cervical spine injury.
**Most common associated injury to thoracic spine.
***Most common associated injury to the lumbar spine.
The average hospital length of stay was 11.4 days, being the longest stay for patients with thoracic spine injuries with an average of 12.96 days. Cervical spine injury patients had an average of 5.33 days, patients with lumbar spine injuries had an average length of stay of 10.8 days, and the only patient we had from sacral spine injury lasted 4 days in the hospital.
Discussion
Emergency services are increasingly having admissions for gunshot injuries due to the increasing violence that is taking place in today’s societies. In a 2-year period, we evaluated a total of 55 patients with gunshot injuries to the spine. Patient distribution by age and sex was similar to the reported in the literature, with a high incidence in the young male population. Cybulski et al. had a male predominance distribution with 83 male patients and five female patients with an average age of 24.7 years7. Heary et al. reported a male predominance and an average of 26 years old8. We also found two reports in Mexican population, Cabrera et al. reported an incidence of 54 patients in a period from January 2001 to November 20069 and Hernández-Téllez et al. reported an incidence of 14 patients in a period from 2009 to 201310.
The approach to a patient with a spine injury secondary to a gunshot wound should always follow the ATLS (advanced trauma life support) protocol before managing any kind of spinal pathology in the trauma patient11. The initial radiologic evaluation should start with two plane radiographs (Fig. 1) even though many centers today advocate the minimal utility of radiographs and prefer using the computed tomography (CT) scan as the initial radiographic study (Fig. 2). CT scan with reconstruction should be considered in every gunshot injury to the spine to determine the integrity of the spine elements. In our center, we do not routinely request an MRI in gunshot spine injuries. The use of magnetic resonance imaging (MRI) in patients with gunshot injuries to the spine remains controversial. Dedini et al. reported that the use of MRI in a patient with retained projectile fragments requires knowing their composition; concluding that alloy and copper fragments are safe to continue the study, while steel is not12.

Figure 1 Lumbar AP and lateral radiograph. A: clinical images. B and C: an 29 y/o male patient with a gunshot injury in T11 (ASIA E).

Broad-spectrum antibiotics should be started as soon as the patients arrive to the emergency department (Fig. 3), regardless of patient status, and injury location. A minimum of 3 days to 14-day course (depending if there is transcolonic injury or not) of broad-spectrum intravenous antibiotics is effective at preventing spine infections5. Several authors have found that the risk of developing a postoperative spine infection in higher in patients with transcolonic injuries7. In our center, antibiotic prophylaxis is administered in all the spinal gunshot injured patients. In cases with no gastrointestinal tract perforation a third-generation cephalosporin (ceftriaxone) at a dose of 1 g IV twice daily, and metronidazole 500 mg IV twice daily for 3 days was administered. In cases of gastrointestinal tract perforation, the antibiotic treatment is extended for a period of 10 days8. Tetanus prophylaxis is administered according to the vaccination status. None of the patients received steroids for the management of spinal cord injury since the literature reported no-benefit with their use9.

Figure 3 Lumbar AP radiograph. A: clinical images. B and C: an 9 y/o patient (ASIA A) with a gunshot injury to the spine at arrival to the emergency department.
The thoracic spine had the highest frequency of injuries in our series with 26 patients (48.5%), followed by the lumbar spine with 25 patients (45.5%), three patients (6%) with cervical spine injuries, and one patient with a sacral injury (1.81%). Injury distribution was similar to the reported in the literature by Benzel et al.13 and by Simpson et al.11, with the thoracic spine having the highest frequency of injuries. Of the total patients assessed in our study, 30 (54.53%) presented with a neurological injury. The prevalence of neurological injury is similar to the data reported in the literature. Kupcha et al. in their study of 28 patients reported that 75% presented with neurological injury14. According to Waters and Adkins in their prospective study of surgical treatment for gunshot wounds to the spine, there is evidence of recovery in patients with incomplete deficits, especially in the T12 to L4 region, so decompression should be performed as soon as possible in a patient with incomplete injury. The general consensus in patients with complete spinal cord injury is that there is no neurological benefit with surgical intervention15. In our patient series, only one patient was surgically managed: 26 y/o male patient with an L1 fracture (Fig. 4) and an incomplete neurological injury (ASIA B). He was taken to surgery within <24 h of evolution. During follow-up, the patient showed no neurological improvement. Patients without neurological deficit were treated with broad-spectrum intravenous antibiotic therapy, wound debridement and immobilization according to the level of injury (e.g., Philadelphia collar, Jewett, or Taylor brace) (Fig. 5).
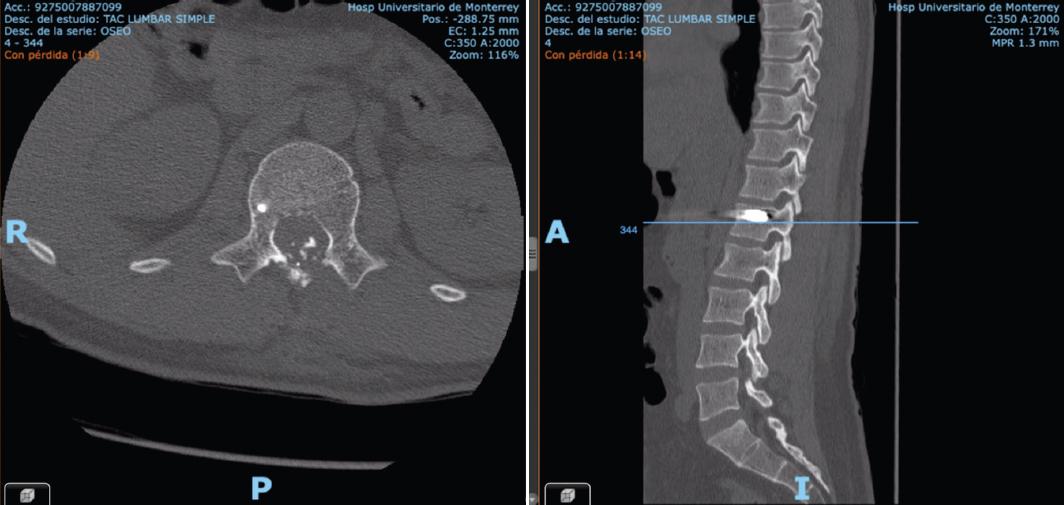
Figure 4 CT scan images of a 26 y/o male patient (ASIA B) showing vertebral body compromise and medullary canal involvement at L1.

Figure 5 Twenty-six y/o male patient with an L1 fracture without neurological injury who was treated with antibiotic therapy, wound debridement, and immobilization with a Jewett brace.
In our series, a total of 45 (81.81%) patients had associated injuries (Table 5). Associated injuries such as visceral or vascular injuries are more life-threatening and must take precedence over diagnostic workup, imaging, and management of any kind of spine trauma or cord injury16. Noorulain et al. reported in their series of 122 patients with gunshot injuries to the spine, 13.93% patients had associated cranial injuries, 24.59% chest wall injuries, and 25.4% abdominal wall injuries17. Sidhu et al. concluded that the most common associated injuries were abdominal visceral with an incidence of 24%18.
Conclusion
Spinal gunshot injuries are associated with significant sequelae, requiring long and costly treatments. This study obtained one of the highest incidences of gunshot injuries to the spine reported in the literature. Based on our data they are more prevalent in the male population with an average age of 30.2 years old. The highest incidence of spinal gunshot injuries was at the thoracic spine and the most frequent associated injury was hemopneumothorax.

