nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Due to the increased incidence and comorbidities leading to high mortality, obesity has become an ever-serious health problem. Although many factors may contribute to the development of obesity, the two most important influences are eating habits and a lifestyle lacking exercise. Nutritional change, physical activity, and some herbal products that are frequently applied in weight gain, as well as medications and surgical interventions in obese and morbidly obese patients, constitute substantial treatment options. Although there are various methods of obesity surgery, sleeve gastrectomy is a highly preferred choice1. After this surgical procedure, where a large part of the stomach and corpus is resected along the greater curvature, the resected gastric tissue is routinely sent to the pathology laboratory for histopathological examination2. Histopathological evaluation, includes inflammation, atrophy, intestinal metaplasia, presence of Helicobacter pylori and other findings beyond these.
Although the most common type of anemia caused by nutritional deficiencies is iron deficiency, anemia due to vitamin B12 deficiency, which is encountered with scarcity or lack of intrinsic factor released from the stomach, is also common3. The anemia that is seen in vitamin B12 deficiency is megalobastic anemia and it can be seen also in folic acid defiency. In the clinical evaluation of megaloblastic changes midcorpuscular volume (MCV) can be used in hemogram. Because of its role in the melatonin metabolism, apart from anemia, pigmentation disorders, skin and mucosal symptoms including atrophic glossitis, and neuropsychiatric findings may be observed in vitamin B12 deficiency4. With its nonspecific nervous system findings, vitamin B12 deficiency may cause permanent damage if not treated5-6. Etiologically evaluated, the presence of atrophy in the stomach and some surgical stomach procedures are in the forefront among the causes of vitamin B12 deficiency7-10.
Patients undergoing partial resection of the stomach may have some vitamin and mineral deficiencies11. There are several theories12 about the frequencies and the pathophysiological mechanisms of these deficiencies that vary in severity. One reason for vitamin and mineral deficiencies encountered in patients undergoing sleeve gastrectomy may be reduced food intake as a result of decreased gastric volume13.
Another important point is that the nutrients stay less in the stomach due to the lack of optimal conditions for absorption14. Besides, the reduced volume will decrease the amount of iron and vitamin B12 absorption, as it will decrease the number of cells and this, in turn, will diminish intrinsic factor and hydrochloric acid production. Additionally, the frequent use of proton pump inhibitors in obese patients undergoing surgery also leads to similar results15. A different point of view is that sleeve gastrectomy can affect absorption by decreasing intestinal hormones such as gherlin, peptide YY, and glucagon-like peptide-1. Due to the single or combined effects of the above mechanisms, the use of prophylactic vitamin B12 appears as a choice in many cases.
In this study, we aimed to evaluate the effect of atrophy observed in the histopathological examinations of the stomach before and after sleeve gastrectomy, an increasingly common surgical procedure, on the response to preventive vitamin B12 treatment. Folic acid levels and MCV levels are also reviewed int terms of potential megaloblastic changes.
Materials and Methods
Sixty patients who underwent sleeve gastrectomy for morbid obesity between 2014 and 2017 were included in this study. Cases with no records in the pathology archive and those who did not receive vitamin B12 and/or folic acid supplementation were not included in the study. Demographic data, vitamin B12 supplementation situation, and vitamin B12, folic acid and midcorpuscular volume (MCV) values were obtained from the hospital management system. Preoperative levels of vitamin B12, folic acid and MCV were measured within the week of operation, and postoperative levels of vitamin B12, folic acid and MCV were measured at 6 months after the procedure. Deficiency was defined as values less than 200 pg/mL for vitamin B1216 and 4 ng/mL for folic acid 17. The MCV values between 80 fL- 100 fL was considered as normal while >100 fL was megaloblastic18.
Hematoxylen& eosin (H&E) stained pathology preparations of resection materials and preoperative endoscopic biopsies were re-evaluated in terms of atrophy. Atrophy was accepted as positive regardless of its severity and magnitude. Preoperative and postoperative vitamin B12 levels, folic asid levels and MCV values were compared with the presence of atrophy. Preoperative and postoperative levels of vitamin B12, folic asic and MCV were also compared. The SPSS 18.0 package program was used for statistical analysis. The analysis were made with 95% confidence intervals; Mann Whitney-U and one way ANOVA tests were used.
Results
The mean age of the cases was 35.5 ± 9.3 years (median 34) and 45 (75%) of 60 cases were female and 15 (25%) were male. All of the patients were using a daily multivitamin tablet containing 2.5 mcg vitamin B12 and 200 mg folic acid. When serum data are examined, the mean values, standard deviations, minimum and maximum levels of preoperative and postoperative vitamin B12, folic acid and MCV are given in table 1 While 55 (91.7%) cases with preoperative vitamin B12 level below 200 pg/mL were observed, this number was observed to be 19 (31.7%) in the postoperative 6th month. When the folic acid levels were examined, the preoperative case with folic acid level below 4 ng/mL was not observed, but it was found in 3 (5%) postoperative cases. While preoperative 16 (26.7%) and postoperative 15 (25%) cases with MCV below 80 fL were detected; preoperative or postoperative cases with MCV above 100 fL were not observed.
Table 1 The mean values, standard deviations, minimum and maximum levels of preoperative and postoperative vitamin B12 (pg/mL), folic acid (ng/mL) and MCV (fL)
| Mean | STD | Minimum | Maximum | |
|---|---|---|---|---|
| Preoperative vitamin B12 | 111,48 | 55,42 | 40 | 255 |
| Postoperative vitamin B12 | 247,69 | 123,67 | 38 | 542 |
| Preoperative folic acid | 10,62 | 3,85 | 4,31 | 22,19 |
| Postoperative folic acid | 7,51 | 3,18 | 3,25 | 23,03 |
| Preoperative MCV | 82,63 | 6,46 | 60,0 | 94,0 |
| Postoperative MCV | 81,5 | 12,30 | 34,5 | 94,0 |
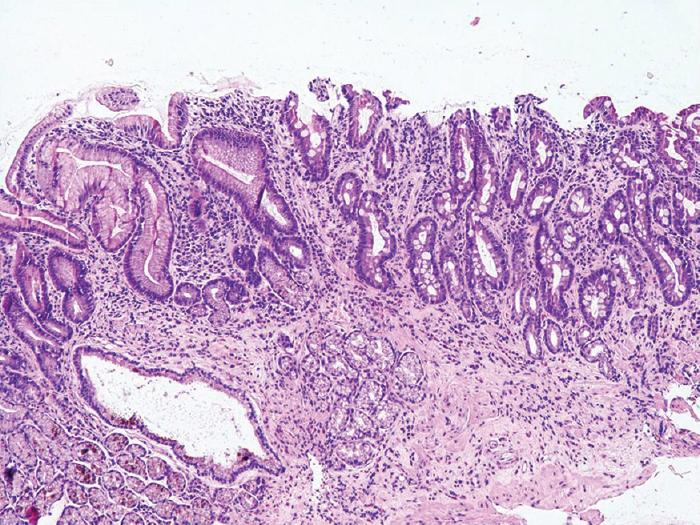
Atrophy was present in 37 cases (61.7%) and absent in 23 (38.3%) in resection materials. Atrophy was observed in 26 (57.8%) of the females and in 11 (73.3%) of the males. A case of atrophic gastric tissue is given in figure 1. When all patients were evaluated for vitamin B12 levels after the operation; in the cases with atrophy in the operation material, despite the administration of vitamin B12, statistically significant lower vitamin B12 levels were found after the surgery compared to cases with no atrophy (p=0.024). When men and women were analyzed separately, the significance continued among females (p= 0.023), while there was no significant difference in males (p=0.480). In the analyzes performed in terms of vitamin B12 deficiency, it was found that preoperative and postoperative vitamin B12 deficiency was not associated with atrophy (p values 0.862 and 0.121, respectively).
The preoperative and postoperative levels of vitamin B12, folic asid and MCV is given in the table 2 in terms of atrophy in the resected tissue and in the preoperative endoscopic gastric biopsy. When preoperative gastric tissue was examined, 36 (60%) of 60 cases did not have atrophy, while 24 (40%) were observed to have atrophy. In the analyzes performed, it was observed that atrophy observed in the resection material correlated with atrophy detected in preoperative endoscopic biopsies (p = 0.000).
Table 2 The preoperative and postoperative levels of vitamin B12 (pg/mL), folic acid (ng/mL) and MCV (fL) in atrophy in the resected tissue and in the preoperative endoscopic gastric biopsy
| Resection | Endoscopic biopsy | |||
|---|---|---|---|---|
| With atrophy | No atrophy | With atrophy | No atrophy | |
| Preoperative vitamin B12 | 113,22 ± 59,67 | 108,7 ± 48,96 | 113,04 ± 64,24 | 110,44 ± 49,63 |
| Postoperative vitamin B12 | 219,62 ± 124,81 | 292,84 ± 109,84 | 200,71 ± 129,19 | 279,01 ± 110,86 |
| Preoperative folic acid | 10,78 ± 3,71 | 10,36 ± 4,14 | 10,81 ± 3,92 | 10,50 ± 3,85 |
| Postoperative folic acid | 7,43 ± 3,62 | 7,61 ± 2,38 | 7,47 ± 4,15 | 7,53 ± 2,41 |
| Preoperative MCV | 83,45 ± 6,37 | 81,80 ± 6.66 | 82,51 ± 7,61 | 82,70 ± 5,68 |
| Postoperative MCV | 82,09 ± 12,24 | 80,61 ± 12,61 | 82,47 ± 11,97 | 80,89 ± 12,64 |
In the statistical analyses atrophy in the resected stomach tissue showed no significant correlation with preoperative and postoperative MCV levels (p values were 0.220 and 0.447 respectively. Similarly preoperative folic asic levels and postopertative levels revealed no statisticaly significant difference compared to the atrophy in resected stomach tissue (p values were 0.621 and 0.475 respectively).
Histopathological findings observed in the preoperative gastric endoscopic biopsy material are presented in table 3. In statistical analyzes, no statistically significant relationship was found between preoperative and postoperative vitamin B12 levels, with Helicobacter pylori, intestinal metaplasia, lymphoid follicule and lymphoid aggregate observed in the stomach. Statistical evaluation could not be made because gastritis was seen in all cases. In the analyzes performed with atrophy observed in preoperative endoscopic biopsy, as in the resection material, preoperative vitamin B12 levels were not correlated (p = 0.706), while the difference between postoperative vitamin B12 levels was statistically significant (p = 0.010). Besides, like atrophy observed in the resection material; there was no statistically significant relationship between preoperative and postoperative MCV and preoperative folic acid and post-operative folic acid values and atrophy in the endoscopic biopsy material (p values 0.751, 0.571, 0.734 and 0.323, respectively).
Table 3 Histopathological findings observed in the preoperative gastric endoscopic biopsy material
| Histopathological parameters | Present (N/%) | Absent (N/%) |
|---|---|---|
| Gastritis | 60/100% | 0/0% |
| Atrophy | 24/40% | 36/60% |
| Helicobacter pylori | 43/71.1% | 17/28.3% |
| Intestinal metaplasia | 55/91.7% | 5/8.3% |
| Lymphoid follicule | 17/28.3% | 43/71.7% |
| Lymphoid agregate | 25/41.7% | 35/58.3% |
In the evaluation of preoperative MCV and postoperative MCV values, there was no statistical relationship between values (p = 0.269). Similarly, it was noted that preoperative vitamin B12 levels and postoperative vitamin B12 levels were not significantly significant (p = 0.125), but preoperative and postoperative folic acid values were correlated (p= 0.018).
Discussion
Obesity, which is widely prevalent all over the world, is a disease that needs to be prevented and treated because it is associated with comorbidities which can have mortal courses. One of the methods used in the management of obese patients today is the effectively applied surgical approach19. Gastric tissue removed after surgery is sent to the pathology laboratory for routine examination. Many studies are reporting on the histopathological findings of sleeve gastrectomy materials2, 20, 21. Vardar et al. from Turkey2 said that they observed atrophy in 4.3% of the sleeve gastrectomy materials. Atrophy was found in 61.7% of the patients in resected stomach tissues in our study, where we included all patients with atrophy, regardless of the extent and severity. It is noteworthy to mention that there is more atrophy among males (73.3%) compared to female patients (57.8%). While the frequency of atrophy was observed as 40% in gastric endoscopic biopsies performed preoperatively, it was noted that the atrophy found in resection material and endoscopic biopsy materials was correlated.
Nutritional deficiencies including many vitamins and minerals have been evaluated by various studies after obesity surgery7-10. However, studies mostly focus on determining the prevalence of failure, evaluation of the frequency, severity, and duration of the disabilities, or revealing the superiority of the methods and types of selected interventions. Moreover, there is also a meta-analysis of studies comparing obesity surgery methods concerning nutritional insufficiency10. On the other hand, literature examining the predictivity of the possible nutritional deficiencies after obesity surgery and responses to treatment is scarce.
Our cases were evaluated regarding vitamin B12 deficiency. The proportion of vitamin B12 deficiency pre- and postoperatively was 91.7% and 31.6%, respectively. In the literature, preoperative B12 vitamin deficiency is reported between zero and 16%22-25, while postoperative insufficiency ranges between 12 and 33%26. In their study evaluating vitamin B12 deficiency preoperatively, one year, and four years after the operation, Ben-Porat et al.7 reported proportions of 7.7%, 13.6%, and 15.4%, respectively. Gillon S et al.27, on the other hand, point to an increase of the preoperatively 6.4% vitamin B12 deficiency to 19% at 12 months followed by a decline at 24 months to 12.8%.In a study published in 201825, it was reported that vitamin B12 deficiency was 16% preoperatively but decreased to 11% after 6 months of regular B12 treatment.
Although vitamin B12 deficiency causes many effects, anemia has an important place among them. Another etiological factor in vitamin B12 deficiency anemia with megaloblastic character is folic acid deficiency. MCV measurement, which can be called old school methods today, is still used as an indicator of megaloblastic changes18. In our study, it was observed that preoperative and postoperative MCV values were not at the megaloblastic level in the investigations performed to reveal megaloblastic changes due to the possibility of vitamin B12 deficiency. MCV values were also not associated with atrophy examined histopathologically. Similarly, folic acid has not been found to be associated with atrophy. Since folic acid absorption is provided from the small intestine, gastric tissue reduction and/or atrophy are not expected to be directly involved in the etiology of low folic acid. However, in studies, folic acid deficiency that develops after obesity surgery varies by months, and varies between 3.4% and 32% in the 12th month8,13,27. It is thought that the decrease in folic acid intake due to the decrease in gastric volume as well as the increased gastric emptying rate are the basis of this deficiency. However, the effect of low folic acid levels that are monitored preoperatively should not be ignored. It has been reported that folic acid deficiency is observed 1.2% -5.1% preoperatively13,23,27 and this low levels of folic acid is predictive of low postoperative levels8. Similarly, in our study, it was noted that postoperative folic acid levels correlated with preoperative folic acid levels (p = 0.018).
In this study, the effect of gastric atrophy, which is in the etiology of vitamin B12 deficiency in the normal population, on sleeve gastrectomies was evaluated, and a statistically significant relationship between atrophy found in resected gastric tissue and vitamin B12 deficiency was not shown. However, it was noted that the response to vitamin B12 supplementation was statistically significantly lower in cases with atrophy in the resection material in these cases, all of whom received vitamin B12 supplements (p=0.024). We think that the atrophy present in the stomach tissue, combined with the intrinsic factor deficiency resulting from the chief cell loss, increase in gastric emptying rate and narrowing of the gastric surface area, which are the results of sleeve gastrectomy, reduces the absorption efficiency of oral vitamin B12. Considering the level of atrophy in the resected gastric tissue that correlates with preoperative endoscopic biopsies, it can be suggested that patients with atrophy in preoperative gastric endoscopic biopsy materials have a low response to postoperative vitamin B12 supplementation. When the predictive value of preoperative vitamin B12 levels for postoperative vitamin B12 levels was examined, no relationship was found between the two values (p=0.125). However, Ben Porat et al. stated that preoperative levels were significant in predicting postoperative vitamin B12 deficiency, as in folic acid8.
Conclusion
Like many nutrients, vitamin B12 deficiency is a condition that should be observed after bariatric surgery and precautions should be taken. In addition to the function restriction of sleeve gastrectomy, supplements are used prophylactically against nutrient deficiencies that occur as a result of other negative factors such as increased gastric emptying rate and decreased stomach cells, and it is very important to observe the response to supplements as well as the use of supplements. Although it has been reported that the most important factor to predict deficiencies after bariatric surgery is preoperative status, studies on this subject are limited. There is no study conducted to predict the response to nutrient support. In this study, the effect of atrophy, which is known to be important in the etiology of vitamin B12 deficiency, in predicting the response to oral therapy in sleeve gastrectomy cases was demonstrated (Figure 2). When the data of the present study were evaluated, it was concluded that the effect of parenteral vitamin B12 support would be more efficient than oral vitamin B12 support used prophylactically in sleeve gastrectomy cases.