











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Volvulus refers to the torsion of a segment of the intestinal tract; this often leads to intestinal obstruction and vascular compromise of the affected segment. The most common sites of volvulus are the sigmoid colon and cecum. In the United States, sigmoid volvulus is more common in men older than 70 years old, and it represents less than 10% of intestinal obstruction.1,2 In Mexico, there is a predominance of female sex.3
Colonic volvulus is more common in some areas of the world; these areas are known as the “Volvulus belt” including Middle East, India, South America, Africa, and Russia. In the Andean area, sigmoid volvulus represents more than 50% of all intestinal obstruction.4 Andean Dolichomegacolon, an acquired condition that causes Andean people who live at an altitude of 3,000 m over sea level to have larger and thicker colon than usual, predisposing this population to colonic volvulus. Also, a fiber-rich diet causes gas formation and distension of the colon, contributing to an elevated incidence of colonic volvulus.5
Colonic volvulus can lead to vascular compromise of the affected bowel segment, leading to septic shock and death. The diagnosis and treatment should be made promptly to avoid such complications.
Synchronic colonic volvulus of the cecum and sigmoid represent a diagnostic and treatment challenge. Only 7 cases, including this one, have been reported in the literature. It is essential to compare the diagnosis, management and different outcomes in these cases.
Case Report
102 year- old female, with a past medical history of chronic constipation and sigmoid volvulus one year ago, with a colonoscopic resolution, presented to our institution with a two-day history of abdominal distension, asthenia, adynamia, and poor appetite. Afterward, she developed intermittent abdominal pain and an inability to pass flatus. Examination revealed a woman in mild painful distress—normal vital signs, with moderate dehydration. The abdomen's inspection revealed a markedly distended abdomen, augmented peristalsis, with mild tenderness to palpation on the left side, without guarding or rebound tenderness. No abnormal laboratory values were found. An x-ray of the abdomen revealed sigmoid volvulus, with dilation of up to 10 cm (Fig. 1). A nasogastric tube was placed, resuscitation and colonoscopic decompression with rectal tube placement was performed without complications. No mucosal patching was seen on colonoscopy.

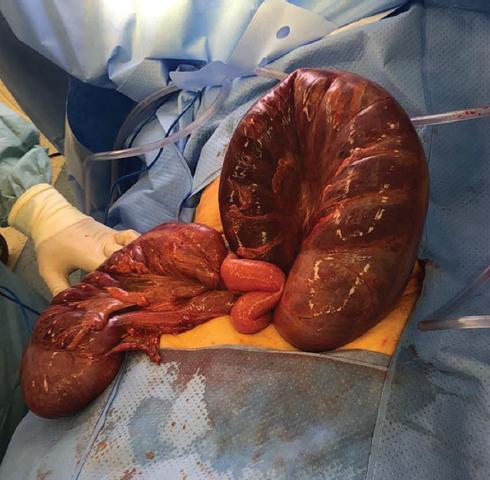
The patient presented clinical and radiographic improvement, with decreased abdominal distention. Parenteral nutrition and liquids were started. On her third day after colonic decompression, she presented abdominal distension, with little tolerance to enteral nutrition and leukocytosis of 14,700 U/L; a CT scan revealed persistence of sigmoid volvulus, with free fluid and indirect data of vascular compromise (Fig. 2). Laparotomy was performed, where sigmoid and cecal volvulus was found, with no evidence of cecal vascular compromise (Fig. 3). A cecal detorsion and a cecopexy were performed, and an extended left hemicolectomy with a terminal colostomy to treat the sigmoid volvulus. Given the patients' malnourished state, added to an acute inflammatory state, no anastomosis was attempted. The postoperative period was uneventful, and the patient was discharged on postoperative day 9. She returned to the hospital with abdominal distension and no output from the colostomy. No radiological evidence of bowel obstruction was found. The diagnosis of acute colonic pseudo-obstruction was made; she was treated with neostigmine and was discharged eleven days later. Three months later, the patient was in good clinical condition, eating normally without any complication.

Discussion
The most common site of colonic volvulus is the sigmoid colon, followed by the cecum. Sigmoid volvulus is more frequent in the sixth to eighth decades of life; it is mostly associated with chronic diseases, neuropsychiatric disorders, and constipation. It is two times more common in men than in women. This pathology generally presents with insidious onset of progressive abdominal pain, nausea, abdominal distension, and constipation.6 It may not be as apparent in older adults, who will generally present mild symptoms.7 The diagnosis is usually established with imaging. On abdominal radiographs, the typical findings include the presence of a u-shaped, distended sigmoid colon, customarily known as the coffee-bean sign. On abdominal CT scan, diagnostic findings of sigmoid volvulus include whirl pattern, caused by dilated sigmoid colon around its mesocolon, and bird-beak appearance caused by progressive narrowing of colon around torsion point.8
Treatment depends on the clinical status of the patient. If the patient is stable and there is no clinical suspicion of bowel necrosis or perforation, a rigid or flexible colonoscopic detorsion should be performed. This allows for the evaluation of the viability of the sigmoid colon. This is effective in 60-95% of patients6, but various studies have demonstrated a recurrence rate of up to 48% in 5 months. 9, 10 The definitive treatment is always surgical. Sigmoidecotmy with primary anastomosis offers better results than non-resective surgical treatment.6
Cecal volvulus is responsible for 1-3% of bowel obstruction. It is more common in younger patients than sigmoid volvulus, generally presenting in patients 35-50 years-old. The incidence is estimated at 2.8 to 7.1 per million people per year. It is also more common in women than in men.11 In Mexico, it represents 21% of colonic volvulus.3 There are three cecal volvulus types; type I is a clockwise axial torsion along its long axis, the cecum remains in the right lower quadrant. In type II, there is torsion of the cecum and the last portion of the terminal ileum, counterclockwise, related to ectopic location, usually in the left upper quadrant. Type III, also known as cecal bascule, is an upward folding of the cecum; this is more common in young women, and it does not cause a vascular compromise in most cases.11
Treatment of cecal volvulus is always surgical. Non surgical reduction is only successful in less than 4% of the patients; plus, it is known that it increases the risk of perforation; bowel ischemia can go unnoticed in 25% of the patients.2, 12 Surgical treatment depends on hemodynamic stability and bowel compromise. If the bowel is compromised, the volvulus should not be untwisted to avoid reperfusion injury.2 An ileocolic resection or right hemicolectomy should be performed, with or without anastomosis. If there is no bowel compromise, then a detorsion can be performed, followed by resection or cecopexy.13 A cecopexy should only be done if a resection cannot be tolerated, for it has a high morbidity and mortality rate, with up to 14% recurrence.14
Synchronous volvulus of the cecum and sigmoid colon is an infrequent entity; to the best of our knowledge, only six cases have been reported in the literatura (Table 1) 15- 20, this one being the seventh. In none of the patients was the diagnosis made preoperatively. The majority of them had a preoperative diagnosis of sigmoid volvulus. 16, 19, 20 While in one case, the preoperative diagnosis was Chilaiditis syndrome.17 All of the patients were male, and the average age was 68.3 years. Detorsion and cecostomy were performed on only one patient.18 A subtotal colectomy was performed in the rest of the patients. Two of the patients (40%) died.16,20 The patient in which a cecostomy was performed was reported stable nine months later.18
Table 1 Synchronous volvulus of the cecum and sigmoid colon
| Author | Age | Gender | Preoperative diagnosis | Preoperative treatment | Surgery | Complication |
|---|---|---|---|---|---|---|
| Moore et al. 13 | 62 | Male | Bowel obstruction- cecal volvulus | NG Tube | Subtotal colectomy + Ileorectal anastomosis | No |
| Roy et al.14 | 77 | Male | Sigmoid volvulus | Colonoscopy + rectal tube | Subtotal colectomy + terminal ileostomy | death |
| Isalm et al. 15 | 80 | Male | Chilaiditis syndrome | - | Subtotal colectomy + ileorectal anastomosis | Anastomosis leak terminal ileostomy |
| Singh et al. 16 | 60 | Male | Bowel obstruction | - | Detorsion + cecostomy | No |
| Berg et al. 17 | 69 | Male | Sigmoid volvulus | - | Subtotal colectomy + terminal ileostomy | - |
| Elsharif et al. 18 | 62 | Male | Stomach, cecal and sigmoid volvulus + situs inversus | Death |
NG: nasogastric
Multiple cases of synchronous volvulus of other parts of the gastrointestinal tract have been reported (Table 2).21- 25 Most of them included the sigmoid colon 21, 22, 24, 25, 26, and another organ, including the gallbladder 21, transverse colon 22, 24, 26, and terminal ileum25, while another presented with cecal and splenic angle volvulus.23 A subtotal colectomy was performed in those patients, that the volvulus was in two segments of the colon 22- 24, while segmental resection was performed in the others. 21, 25, 26
Table 2 Synchronous volvulus of GI tract
| Author | Age | Gender | Preoperative diagnosis | Involved segments | Surgery | Complication |
|---|---|---|---|---|---|---|
| Chittal et al. 19 | 71 | Female | Sigmoid volvulus | Sigmoid colon + Gallbladder | Cholecystectomy + sigmoidectomy + colorectal anastomosis | Postoperative AMI |
| Motsumi et al. 20 | 26 | male | Sigmoid volvulus | Sigmoid and transverse colon | Subtotal colectomy + colostomy | No |
| Islam et al. 21 | 56 | Female | Internal hernia vs. tumor | Cecum and splenic angle | Subtotal colectomy + ileocolonic anastomosis | No |
| Lianos et al. 22 | 81 | Female | Bowel obstruction | Sigmoid and transverse colon | Subtotal colectomy + terminal ileostomy | No |
| Rivera 23 | 33 | Female | Recurrent sigmoid volvulus | Distal ileum + Sigmoid colon | Ileal resection + anastomosis + Hartman procedure | No |
| Ndong et al. 24 | 74 | Male | Bowel obstruction Sigmoid and transverse colon Left hemicolectomy + Loop colostomy |
No | ||
AMI: acute myocardial infarction
The synchronous volvulus of the colon is an unusual pathology that can be easily missed. The diagnosis is almost always done surgically, and the treatment varies according to the location and hemodynamic stability. Prompt surgical intervention determines the prognosis.

