











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Hypopharyngeal neoplasms account for 8-10% of all neck cancers, with an incidence of 1/100,000 inhabitants per year. They occur predominantly in males (20:1)1-7. Populations with high tobacco, cigarette, and alcohol consumption have a higher incidence7-9. Head-and-neck malignancies are characterized by significant esthetic and functional deficits. Surgical resection is associated with oropharyngeal dysfunction, resulting in poor quality of life and malnutrition, among other complications8,9. Most patients are diagnosed at an advanced stage of the disease and often require different types of neck surgeries with esophageal reconstruction. These are challenging procedures for oncological surgeons.
Radial forearm free flap was reported by Nakatsuka et al.10 and the subsequent advancements in microsurgery have contributed to successful single-stage reconstruction of complex oropharyngeal, laryngeal, and cervical esophageal defects with minimal complications. The use of free flaps has been considered as a common reconstructive technique since involved tissues have increased vascularization, lightweight, malleability, and versatility. The anterolateral thigh (ALT) flap is supplied by perforating vessels of the descending branch of lateral circumflex femoral artery. Despite its favorable characteristics, tissue volume can limit its use to large defects11. The radial forearm free flap, due to its pliability, thinness, and length of the vascular pedicle, is an ideal flap for esophageal reconstruction12. Herein, we present our experience with radial forearm and anterolateral thigh (ALT) free flap for advanced reconstruction of neck defects.
Materials and Methods
Study design
This was a retrospective study of patients who underwent hypopharyngeal and cervical esophageal tumor resection followed by functional reconstruction with radial forearm or anterolateral thigh (ALT) flap at our center, between February 2010 and December 2017. All patients above the age of 18 years who underwent the above procedures were included for analysis. Patients with other malignant neoplasms, history of gastrectomy, reconstruction for benign esophageal disease, uncontrolled diabetes mellitus type II, pulmonary disease, liver cirrhosis, or unresectable esophageal tumors were excluded from the study.
Inclusion and exclusion criteria
Patients over 18 years of age underwent radial forearm or ALT free flap for esophageal reconstruction after oncological cervical exenteration of advanced tumors of pharyngeal and esophageal tissues. The exclusion criteria were defined as the coexistence of other malignant neoplasms, history of gastrectomy, reconstruction for benign esophageal disease, uncontrolled comorbid disease such as diabetes mellitus type II, pulmonary disease, or liver cirrhosis, and an unresectable esophageal tumor. Out of a total of 55 patients who underwent the previously described procedures, 38 patients were found to be eligible for analysis. All patients were managed by a multidisciplinary team of oncological, general, plastic/reconstructive, and head-and-neck surgeons. Operative procedures in all cases included laryngopharyngectomy or esophagectomy with lymph node dissection followed by reconstruction. Data collected included clinical characteristics, stage of disease, histology, age, sex, operative workup, complications, ICU admission, length of hospital stay, pathology, reintervention, follow-up, and mortality (Table 1). Anastomotic leakage was defined as extravasation of contrast material during water-soluble contrast swallow or visualization of anastomotic breakdown on endoscopy. Benign anastomotic stricture was defined as stenosis that precluded passage of a 9 mm endoscope in the absence of recurrent cancer. All patients were offered post-operative endoscopy and evaluation for dysphagia after 3, 6, and 12 months. The median follow-up was 3 years (range, 24-48 months). The study protocol was approved by the Institutional Ethics Committee. The protocol was implemented in accordance with the provisions of the Declaration of Helsinki and Good Clinical Practice guidelines.
Tabla 1 Sociodemographic characteristics
| Sociodemographic characteristics (n = 38) | ||
| Age (years) | Mean (SD) | 52.7 (12.8) |
| Medium (IQR) | 54 (46.2-61.2) | |
| Gender, n(%) | Male | 8 (20) |
| Female | 30 (80) | |
| Previous pathology, n (%) | Papillary thyroid cancer | 22 (60) |
| Follicular thyroid cancer | 4 (10) | |
| SCC larynx | 12 (30) | |
| Radiation therapy, n (%) | Yes | 8 (20) |
| No | 30 (80) | |
| Chemotherapy, n (%) | Yes | 4 (10) |
| No | 34 (90) | |
| Days in intensive care unit | Medium (SD) | 10.1 (4.5) |
| Median (IQR) | 9.5 (6-14.5) | |
| Hospitalization days | Medium (SD) | 16.2 (6.7) |
| Median (IQR) | 16 (10-21.2) | |
Statistical analysis
All data were entered into Microsoft Excel databases and analyzed using SPSS 1 (Statistical Package for the Social Sciences) version 22.0. Variables were described as mean (range), median, minimum and maximum values, percentages, standard deviation (SD), and interquartile range (Table 2).
Tabla 2 Surgical intraoperatory variables
| Surgical intraoperatory variables (n = 38) | ||
| Type of defect, n (%) | Laryngopharyngoesophagectomy | 31(80) |
| Laryngopharyngoesophagectomy hypopharynx | 7 (20) | |
| Circumferential, n (%) | Yes | 24 (60) |
| No | 14 (40) | |
| Type of flap, n (%) | ALT | 24 (74) |
| Radial | 14 (26) | |
| Monitoring flap, n (%) | Yes | 27 (70) |
| No | 11 (30) | |
| Oral feeding, n (%) | Yes | 34 (90) |
| No | 4 (10) | |
| Supply type, n (%) | Gastrostomy | 4 (10) |
| Semisolid | 10 (30) | |
| Solids | 24 (60) | |
| Gastrostomy, n (%) | Yes | 19 (50) |
| No | 19 (50) | |
Microsurgical flap reconstruction technique
After confirmation of adequate tissue perfusion with Allen test and Doppler ultrasound of the cubital artery, the non-dominant forearm was chosen for the radial forearm free flap; similarly, a normal Doppler ultrasound blood flow was used to determine suitability for ALT flap. Either anterolateral thigh or radial forearm flap was chosen according to the defect to be reconstructed. We chose a radial forearm technique in patients with a BMI less than 30 kg/m2 and ALT flap technique in those with a BMI of 30 kg/m2 or above.
Radial forearm free flap
After placement of a 240 mmHg ischemic bracelet, dissection is started at the subaponeurotic level from the radial to the cubital extremities up to the media line including the superficial cephalic vein, radial artery, and the two concomitant veins (Fig. 1). The plane of dissection was kept just deep to the fascia and fasciocutaneous flap carefully developed to preserve the lateral intermuscular septum and its perforators from the radial vessels, and also to isolator and preserve the superficial veins are required. The cephalic vein and the superficial nerve were dissected into the deltoid and upper arm, respectively, to obtain greater length, elevation of the flap subfascial exposed muscle proximally, and tendons with paratenon intact distally for skin graft. The palmaris longus tendon which lays within a condensation of the deep fascia was freed or included as required; if it was freed, taking care to preserve it paratenon. Care was taken to preserve the superficial branch of the radial nerve by dissection from the underface of the flap (Fig. 2).


Anterolateral thigh flap
First, a line joining the anterior superior iliac spine and the upper outer border of the patella is marked. This line corresponds to the intermuscular septum between the rectus femoris and the vastus lateralis muscles. Skin vessels supplying the anterolateral thigh flap are usually located along this line or slightly lateral. The midpoint of this line is then marked. Additional perforators are located 5-10 cm proximal and distal to the midpoint perforator. After the flap is raised in the direction proximal to the vascular point, the perforating veins are carefully ligated, and the flap design is completed using a 37 Fr bougie. Simultaneously, another team performs an oncological exenteration of the neck (total pharyngeal laryngectomy along with cervical esophagectomy), permanent tracheostomy, and dissection of receptor veins and arteries. The distal esophageal anastomosis is performed first using a 1.5 cm longitudinal incision in the esophagus to match the diameter of the flap using unique interrupted sutures with PDS 3-0 (Ethicon, Inc., Cincinnati, OH, USA). Thereafter, oropharyngeal anastomosis is performed using the same suture technique. Finally, microvascular anastomosis is performed to the receptor vessels of the internal jugular veins and branches of the external carotid artery as superior thyroid, facial and superficial temporal arteries using continuous non-interrupted sutures with Ethilon 9-0 (Ethicon, Inc., Cincinnati, OH, USA)2,3. The anterolateral thigh flap length and diameter are set at 9.5 cm and 3 cm, respectively, to create a functional neopharyngeal tube. Follow the pedicle proximally until a decent caliber artery and vein are identified, large branches to the undersurface of rectus are encountered. Significant variation in vascular anatomy is encountered especially of the vein. The two venae comitantes often merge into a single vein before entering the deep femoral vein. With gentle blunt dissection, separate the fascia lata from the vastus lateralis lateral to the perforator. Two perforating arteries should be included in the reconstruction design of the flap, one for the monitoring flap and the second to reconstruct the pharyngeal defect2,3. All patients undergo a Stamm gastrostomy for enteral nutrition in the immediate post-operative (PO) period. Oral feeding is reinstituted after confirming adequate anastomosis by upper GI radiography on PO day 7.
Results
A total of 38 advanced cervical esophageal reconstructions were performed using radial forearm or ALT free flap technique. Mean age and sex distributions were similar in both groups. About 80% of participants were female, and the mean age was 51 years. Primary diagnoses included papillary thyroid tumors (60%), squamous cell carcinoma of the larynx (30%), and thyroid follicular cancer (10%) (Table 1). The defects were either laryngoesophageal (80%) or hypopharyngeal-esophageal (20%). Total circumferential reconstruction was required in 60% of patients, while 40% required a partial reconstruction. Radial forearm flap was used in 26% of patients and anterolateral thigh flap in 74% (Table 2).
An elliptical monitoring flap is outlined near the graft in 70% of the cases, the main reconstruction flap is outlined proximal to the monitor flap. Clinical assessment of tissue color, turgor, capillary refill, and bleeding is done in the standard fashion. Graft microvascular anastomosis was performed to the superior thyroidal artery in 60%, transverse cervical artery in 20%, facial transverse artery in 10%, and right carotid artery in 10% of cases. Tumor recurrence was not reported in the study patients during the 24-month post-operative follow-up, and no flap failure was reported in both techniques.
Post-operative complications
Twenty-two (57.9%) patients had an uneventful PO recovery. Early complications were recorded in 30% of patients and mainly included fistula formation (overall, 20%; radial forearm flap, 20%; and ALT free flap, 8.3%). The other significant complication (10%) was superficial surgical site infection (ALT flap, 16%; radial forearm flap, none). There were no cases of suture site breakdown or need for reintervention at the donor site. Late complications, including stenosis and distal graft lumen obstruction, were seen in 20% of study patients. The mean time to appearance of these complications was 7.5 months postoperatively. No patient deaths were observed either in the immediate post-operative phase or during their follow-up. Mean post-operative ICU stay and hospital stay were 10 and 16 days, respectively. About 50% of the patients needed more than 7 days gastrostomy in the post-operative, only 10% of the patients were unable to tolerate oral feeding and needed definitive gastrostomy (Tables 3 and 4).
Tabla 3 Surgical complication
| Surgical complication (n = 38) | ||
| Fistula, n (%) | Yes | 8 (20) |
| No | 30 (80) | |
| Dehiscences, n (%) | Yes | 2 (5.2) |
| No | 36 (94.7) | |
| Infections, n (%) | Yes | 4 (10) |
| No | 34 (90) | |
| Flap constriction, n (%) | Yes | 8 (20) |
| No | 30 (80) | |
Tabla 4 Descriptive analysis between ALT versus brachial-radial graft
| Variables | ALT (n = 24) | Radial (n = 14) |
|---|---|---|
| Sociodemographic characteristics | ||
| Age (years) | 58 (53-70) | 44 (25-54) |
| Chemotherapy, n (%) | 4 | 0 |
| Days in intensive care unit, days (min-max) | 7(5-10) | 14 (10-18) |
| Hospitalization days, days (min- max) | 17 (10-25) | 15 (6-26) |
| Outcomes and complications | ||
| Fistula, n (%) | 2 (8.3%) | 6 (42,8%) |
| Dehiscences, n (%) | 2 (8.3%) | 0 |
| Infections, n (%) | 4 (16.6%) | 0 |
| Flap constriction, n (%) Gastrostomy, n (%) | 2 (8.3%) 11 (45.8%) | 6 (42,8%) 8 (57,1%) |
Discussion
Advances in microsurgery and plastic surgery have enabled tissue reconstruction and tissue transfer for complex defects with increasingly esthetic results. It is important to employ functional techniques wherever possible to provide the best patient outcomes. Early pharyngeal reconstruction techniques were reported by Czerny et al. in 1877, and Trotter in 188813-15. In 1942, Wooky's16 use of flaps initiated a new era in cervical reconstruction. Subsequently, Seidenberg in 195917, used jejunal flaps for esophageal reconstruction by employing microsurgical techniques. Furthermore, Bunke described an omental flap technique in 1927, while Daniel and O'Brien demonstrated an inguinal graft technique18,19. Several aspects of the treatment of hypopharyngeal carcinoma have remained controversial, including the choice of radiotherapy, which is beneficial for tumor control but is associated with complications such as dysphagia, stenosis, and paralysis. Recently, studies show that only chemoradiotherapy offers similar survivorship compared to surgery in advanced disease, however, it still in debate, advance hypopharyngeal carcinoma always benefits from an integral management thus being the ideal chemoradiotherapy treatment associated with surgical management with reconstruction, as seen in this case series20,21. There are variables that the multidisciplinary surgical team should take into account before surgery. These include vessel integrity and vessel anatomy, identifying vessels previously exposed to inflammation or radiation, considering the possibility of anastomosis, and remembering to avoid tension and torsion (Fig. 3). The superior thyroid artery can be 10 used for end-to-end anastomosis and the internal jugular vein for end-to-side anastomosis (Fig. 4). The determination of the surgical technique is influenced by the type of defect (partial or total). As a matter of compromise, it is preferable to use the jejunal graft reconstruction with lower rates of fistulas. Radial forearm flap is more resistant and has better vascularization, but with a 50-100% higher rate of stenosis and fistulae in comparison to jejunal flaps. The primary cause of fistulae is longitudinal sutures in cervical reconstruction, the use of jejunal flaps reduces fistula22. The anterolateral thigh free flap is a cutaneous or fasciocutaneous flap vascularized by one or several perforating arteries arising from the descending branch of the lateral circumflex femoral artery. Venous drainage occurs through the perforators or a similar route to the deep femoral system or the femoral vein.

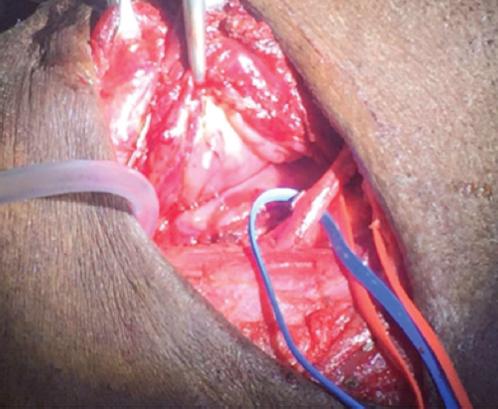
Figure 4 Pharyngolaryngoesophagectomy with vascular dissection; jugular vein and superior thyroid artery.
The underlying principle of hypopharyngeal reconstruction is to reintegrate the digestive tube and maintain phonation while avoiding stenosis and fistulae. Large defects require large grafts, as illustrated by several patients in our study. Patients with advanced stages of hypopharyngeal tumors require single-stage surgery with immediate reconstruction so as to avoid functional complications18-19. The addition of esophageal reconstruction to radical oncological resection offers patients better results both in terms of function and esthetics. We have demonstrated that the use of advanced microsurgical techniques and grafts in performing cervical reconstruction in our patients was associated with a lower fistula rate (20%) compared to cases reported in literature (24%)19,23. The incidence of fistula formation was lower with ALT flaps (8.3%) compared to radial forearm flaps (20%). Jejunal graft reconstructions had a higher rate of failure (>7.5%) compared to no failures with ALT or radial forearm flaps in our study23.
The choice of the type of flap depends on the size and location of the defect. Small and partially covered defects, benefit from the use of a radial flap, and for larger and circumferential pharyngeal reconstructions benefit from an ALT flap. It will also depend on the pharynx, larynx, and esophagus tumoral compromise, and the condition of the donor tissue in terms of vascularization and adipose muscular tissue amount. However, Denewer et al.23 recommend that flap choice should depend on the location of the defect with respect to the clavicle.
In our study, we chose a radial forearm technique in patients with a BMI < 30 kg/m2 and ALT flap technique in those with a BMI of 30 kg/m2 or above. Radial forearm and ALT flap are useful for reconstruction due to their robust nature and excellent perfusion. They are versatile, flexible, resistant to ischemia, and adapt to different tissues. As described by Tornero in 2014, these grafts can facilitate reconstruction based on a single pedicle of 12-14 cm in size, with a skin free area of 70%.24 We always included a multidisciplinary surgical team as part of our approach to perform resection, and functional and esthetic reconstruction. The limitations of our approach are loss of cosmesis at the graft site, tendon exposure during resection, changes in local sensitivity, and skin loss. The benefits included gain of function with a low fistula rate of 20%. Further, there is evidence that the use of muscular grafts (radial forearm and ALT) preserves muscular function and maintains swallowing function of the esophagus following secondary radical oncological resections23-25. According to published literature, myocutaneous flaps contribute to 40% preservation of deglutition 24-25 compared to 90% preservation in our series. This may be due to the type of flap and preservation of adequate blood supply. In our study, except for four patients in the radial forearm group, all patients had preserved deglutition. Recent case series report stenosis rates of 5-40% and 6% with radial forearm flaps and ALT, respectively. Jejunal flaps have a stenosis rate of 15-22%23-27. Our results demonstrate stenosis rates of 8.3% for the ALT group and 20% for the radial forearm group. These could be due to the quality of flap, tension-free anastomosis, and excellent flap blood supply with our technique26,27.
The main limitation of our study is its retrospective design, which may have contributed to selection bias. Furthermore, despite being a national referral center, the number of patients is limited due to inadequate health coverage by the state. The regular patients treated at our institution are of low socioeconomic status, from rural cities or distant towns outside the capital district, that difficult the continuation of post-operative outpatient care. This special social condition of our patients made that they needed more length of hospital stay to guarantee their adequate nutritional support, pain management, and rehabilitation.
In addition, our sample size and complication rates are too small to accurately calculate the incidence of complications. A prospective randomized trial with adequate sample size may provide reliable results. The procedure can be performed with low mortality, acceptable morbidity, and a short hospital stay. It has now become the preferred method of reconstruction in this type of patients at our institution. However, because of the relative paucity of large series applying free flap in esophageal reconstruction and the lack of direct comparison with other reconstructive tools, no definitive conclusions can be made regarding its apparent superiority versus less morbid reconstructive procedures such as myocutaneous free flaps. Further studies will be necessary to compare the use of chemoradiotherapy, larynx preservation, and surgery in terms of overall survival and quality of life, especially the ability to continue oral feeding.
Conclusions
ALT and radial forearm flaps have high success rates with low incidence of complications in hypopharyngeal and cervical esophageal reconstruction. The head-and-neck surgeon must know the different indications and precautions of each technique to choose the right flap technique for the right patient, to provide the best reconstructive alternative and recover the functionality of the pharyngoesophageal tract.

