











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The emergence of a pandemic can cause psychosocial disruption in response to a threat. The World Health Organization (WHO) warns that at least a third of the population exposed to a pandemic may suffer a psychopathological manifestation, according to the magnitude of the event and the degree of vulnerability1. The first reaction is panic, a sudden and extraordinary fear that can influence behavior and decision-making2. There is a psychosocial impact that has been observed in the history of infectious diseases: for example, that produced by the AIDS pandemic in the 1980s. The fear of being infected by the human immunodeficiency virus (HIV) brought discrimination and isolation as a social problem3.
Humanity has faced infectious diseases that have caused millions of deaths, such as the 1346 black plague4; smallpox that arrived in Mexico along with the Spanish in the 16th century, which become the most devastating pandemic in America5; the H1N1 influenza of 1918 (Spanish influenza)6; AH1N1 influenza in Mexico that started in 2009, until it was declared a pandemic7 and now the 2019 coronavirus disease (COVID-19).
In December 2019, the first case of pneumonia of unknown origin was reported in the city of Wuhan (Hubei, China), which spread rapidly8,9. The identified pathogen was an RNA-wrapped beta-coronavirus that was initially named as COVID-19, and later as coronavirus-2 of the acute respiratory syndrome (SARS-CoV-2)10, because it shares phylogenetic characteristics with the severe acute respiratory syndrome coronavirus (SARS-CoV) responsible for the epidemic in China and later in Hong Kong in 2002. On January 30, 2020, the WHO declared an international public health emergency, and on March 11, 2020, due to alarming levels of spread, the coronavirus was characterized as a pandemic11.
In 2003, Peng et al.12 conducted a study evaluating the post-crisis psychological distress of the SARS outbreak in Taiwan, correlating psychological distress with the perception of the epidemic. On the other hand, Goulia et al.13 evaluated the psychological distress of health care workers during the 2009 AH1N1 influenza pandemic, in which a moderate degree of anxiety and concern was found that correlated with their psychological distress.
To identify these emotional states, a psychological evaluation is of utmost importance and in some cases allows planning of the intervention. Psychometry is a field of psychology that allows us to explore and analyze the behavior of a person or a group of people, using psychometric tools such as tests14. The Depression Anxiety Stress Scale (DASS-21) is a 21-item questionnaire that has been validated for the Hispanic population (Cronbach's alpha = 0.96)15 and has been applied in diverse groups such as health care workers and university students16,17. Furthermore, the State-Trait Anxiety Inventory (STAI), consists of two self-assessment scales that are used to measure two different dimensions of anxiety (anxiety as a trait and anxiety as a state)18, also validated for the Mexican population (Cronbach's alpha = 0.87)19. The emotional state generated by the COVID-19 pandemic in society should not be ignored. That is why the objective of this work was to assess the state of anxiety, depression, and stress that permeated society during the development of the COVID-19 pandemic.
Methods
The mixed methods study was carried out from March 22 to 30, 2020. We included, by non-probability sampling determined by time, Mexican subjects of legal age, any gender, who had access to an electronic device that allowed them to answer a survey, and who previously agreed to participate in the study through a digital informed consent; this adult population sample was recruited using social media platforms. All personal data were treated confidentially.
A digital questionnaire divided into three sections was developed (Google Forms, Google LLC, USA) to determine the perceptions, emotions, and behaviors related to the COVID-19 pandemic. The recruited subjects were asked to answer a series of questions structured specifically for this study, seven of demographic characteristics (age, gender, academic degree, and socioeconomic status), and 11 multiple-choice questions grouped as follows: (a) general perceptions of COVID-19, (b) general perceptions of the 2009 AH1N1 influenza epidemic in Mexico, (c) concerns and emotions related to the current situation, (d) perception of information about the pandemic, and (e) care of children during the contingency.
The second section consisted of the 21-item Depression, Anxiety, and Stress Scale (DASS-21) developed by Lovibond and Lovibond20, which proved to be reliable and consistent when compared to other similar scales21,22. This instrument made with the Likert technique, measures the states of depression, anxiety, and stress through three scales of 7 items each, and four possible responses classified as follows: (a) did not apply to me at all, (b) apply to me to some degree or some of the time, (c) apply to me to a considerable degree a good part of the time, and (d) apply to me very much or most of the time.
In addition, the Spielberger STAI questionnaire was included23-26, which consists in two segments of 20 items each designed with the Likert technique, in which anxiety is measured as a state (A/S) operationally defined as anxiety experienced in a given moment or situation and anxiety as a trait (A/T) that refers to the level of anxiety in general. Punctuation was determined through four possible responses for each item: (a) not at all, (b) somewhat, (c) moderately so, and (d) very much so and (1) almost never, (2) sometimes, (3) often, (4) almost always, respectively. The score of each test was calculated by summarizing the points of each answer, and it was evaluated according to its standardized severity indices.
Statistic analysis
For demographic variables and questionnaires, proportions and 95% confidence intervals (C.I. 95%) were calculated. A comparison of the proportions between gender and the severity indices of the DASS and STAI A/S and A/T tests was performed using the Chi-square test. A p-value < 0.05 was considered statistically significant. The results were stored and analyzed in the SPSS software version 25 for Windows.
Results
Six-hundred and thirteen subjects with a mean age of 26.77 ± 10.30 standard deviation were included. The demographic characteristics are shown in table 1. About 77% (n = 472) had an education equal to or higher than a bachelor's degree, and < 15% (n = 92) were located in a socioeconomic status different to the mean. Of the total of surveyed subjects, only 15% (n = 92) expressed having any disease associated with a risk factor for having COVID-19.
Table 1 Demographic characteristics in the sample (n = 613)
| Variables | Percentage % (n) |
|---|---|
| Gender | |
| Female | 76 (466) |
| Male | 24 (147) |
| Academic degree | |
| Primary | 0.8 (5) |
| High school (junior) | 1.5 (9) |
| High school (senior) | 11.4 (70) |
| Technical career | 4.9 (30) |
| Incomplete career | 4.4 (27) |
| Bachelor's degree | 60.8 (373) |
| Postgraduate | 16.2 (99) |
| Socioeconomic status | |
| Low | 13.2 (81) |
| Medium | 85.3 (523) |
| High | 1.5 (9) |
| Systemic diseases | |
| Hypertension | 4.9 (30) |
| Diabetes | 3.2 (20) |
| Autoimmune | 5.4 (33) |
| Respiratory | 1.5 (9) |
| Allergy | 1.6 (10) |
| Gastritis | 0.7 (4) |
| Others | 6.2 (38) |
| None | 76.5 (469) |
| Habits | |
| Drinking alcohol | 17.1 (105) |
| Smoke | 11.6 (71) |
| Drug's use | 1.5 (9) |
| None | 69.8 (428) |
| Residency | |
| Mexico city | 56.5 (346) |
| Mexico state | 15.7 (96) |
| Oaxaca | 7.2 (44) |
| Puebla | 5.5 (34) |
| Guerrero | 2.6 (16) |
| Others | 12.5 (77) |
| Children | |
| Yes | 23.3 (143) |
| No | 76.7 (470) |
The pandemic perception questionnaire (Table 2) showed that 82.9% (79.9-85.9) of people had the feeling of concern and chaos, but only 10.8% (8.3-13.3) considered that COVID-19 is a dangerous and serious disease. Regarding AH1N1 influenza, more than half agreed that there was a lot of misinformation during the 2009 pandemic in Mexico, but only 27.4% (23.9-30.9) could locate someone who suffered from this disease. Even though the greatest concern of the sample was there could exist more deaths derived from COVID-19 (37.4%, 33.6-41.2), only 17 subjects claimed to know someone infected with the coronavirus. Five-hundred and forty-four people reported having an emotion other than "indifference," which had a proportion similar to the perception that the preventive measures applied against the pandemic are exaggerated (11.3% [9.8-13.8] and 9.8% [7.4-12.2], respectively). Of the 143 people who mentioned having young children, 74.4% (70.9-77.9) recognized that a woman was in charge of caring for them during the health contingency due to COVID-19.
Table 2 Perceptions, emotions, and behaviors related to pandemics
| Questions | Answers | Percentage (C.I. 95%) |
|---|---|---|
| When you hear the word "pandemic," what do you think? | Chaos | 27.4 (23.9-30.9) |
| Exaggeration | 5.2 (3.4-7.0) | |
| Deaths | 11.9 (9.3-14.5) | |
| Concern | 55.5 (51.6-59.4) | |
| Regarding COVID-19, do you consider | Is something that must be taken seriously | 78.6 (75.4-81.8) |
| It is a government invention | 0.7 (0.0-1.4) | |
| It is just a flu | 4.2 (2.8-5.8) | |
| It is a worldwide conspiracy | 5.7 (3.9-7.5) | |
| It is a serious and dangerous disease | 10.8 (8.3-13.3) | |
| What do you remember of the outbreak of Influenza AH1N1? | At first it was thought to be a government invention | 13.9 (11.2-16.6) |
| There was fear, panic, and deaths | 26.9 (23.4-30.4) | |
| There was a lot of misinformation from the beginning | 50.4 (46.4-54.4) | |
| People supported each other to get ahead | 8.8 (6.6-11.0) | |
| Did you know someone who has suffered from AH1N1 influenza? | No | 65.7 (61.9-69.5) |
| Yes | 27.4 (23.9-30.9) | |
| Maybe | 6.9 (4.9-8.9) | |
| What worries you most about the coronavirus? | Do not let me work | 26.4 (22.9-29.9) |
| I do not have health insurance in case I get sick | 7.3 (5.2-9.4) | |
| That there may be more deaths | 37.4 (33.6-41.2) | |
| Make it a very serious illness | 28.9 (25.3-32.5) | |
| Does any family member or acquaintance currently have coronavirus? | No | 93.5 (91.5-95.5) |
| Yes | 2.8 (1.5-4.1) | |
| Maybe | 3.8 (2.3-5.3) | |
| Select which emotion best describes how you feel about the COVID-19 | Distress | 61.2 (57.3-65.1) |
| Anger | 7.7 (5.6-9.8) | |
| Indifference | 11.3 (8.8-13.8) | |
| Fear | 10.4 (8.0-12.8) | |
| Sadness | 9.5 (7.2-11.8) | |
| Do you consider preventive measures against coronavirus? | No | 90.2 (87.8-92.6) |
| Yes | 3.3 (1.9-4.7) | |
| Maybe | 6.5 (4.5-8.5) | |
| Do you think you are well informed about the COVID-19? | No | 20.6 (17.4-23.8) |
| Yes | 46.2 (42.3-50.1) | |
| Maybe | 33.3 (29.6-37.0) | |
| What are the sources of information you use? | Scientific articles/scientific sources | 51.7 (47.7-55.7) |
| Newspaper/printed sources | 2.0 (0.9-3.1) | |
| Social media/internet | 34.3 (30.5-38.1) | |
| TV/radio | 12.1 (9.5-14.7) | |
| In case of having small children, who cares for them mainly during the contingency? | Mother | 71.9 (68.3-75.5) |
| Father | 7.0 (5.0-9.0) | |
| Grandparents | 12.1 (9.5-14.7) | |
| Aunts | 2.5 (1.3-3.7) | |
| Older brothers | 3.8 (2.3-5.3) | |
| Kindergarten | 1.3 (0.4-2.2) | |
| No one | 1.3 (0.4-2.2) |
The proportions between the different levels of depression, anxiety, and stress are shown in figure 1. The scores of the DASS-21 showed that, of the subjects with a moderate anxiety level (n = 89), 82% (79.0-85.0) had mild depression and 18% (15.0-21.0) moderate. In addition, of the subjects with very severe anxiety (n = 114), 8.8% (6-6-11.0) also had moderate depression, 36% (32.2-39.8) severe, 55.3% (51.4-59.2) very severe depression, 40.4% (36.5-44.3) moderate stress, 28.1% (24.5-31.7) severe, and 31.6% (27.9-35.3) very severe. Only 50 of those with severe anxiety showed mild (82%, 79.0-85.0) and moderate stress (18%, 15.0-21.0). The female gender had a higher proportion of depression (p = 0.04), anxiety (p = 0.01), and stress (p = 0.02) when compared to the male gender.

Figure 1 Proportions of levels of depression, anxiety, and stress according to the DASS-21. A higher proportion of subjects with a very severe degree of anxiety is observed compared to the states of depression and stress.
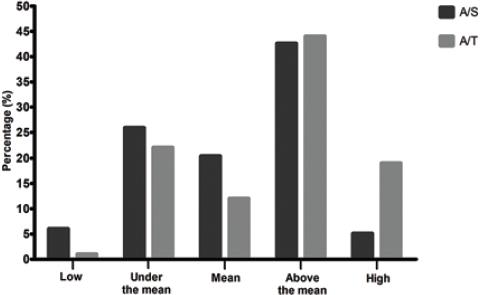
Figure 2 shows the proportions between anxiety levels as a state and as a trait. Of the total sample, 42% (38.1-45.9) had anxiety as an emotional state about the COVID-19 pandemic. Of these, 70 (26.8%, 23.3-30.3) showed high anxiety as a trait, and 132 (50.6%, 46.6-54.6) were above the mean. The proportion of subjects with A/S above the mean was higher in the male gender compared to the female (57.1% [53.2-61.0] vs. 38% [34.2-41.8], p <0.0001), and this difference also existed between genders when A/S was high (9.5% [7.2-11.8] vs. 3.6% [2.1-5.1], p = 0.004).
Discussion
The results indicate that 48.8% of the evaluated subjects had anxiety from mild to very severe associated with the COVID-19 pandemic, and 18.6% of these also experienced depression or stress from moderate to very severe, according to the DASS-21 test. This is consistent with the results of the STAI test, in which it was found that 42% of the sample had anxiety as a state. Although only 5.1% of them presented high anxiety, 19% had it as a trait of their personality, which would mean that 13.9% of the subjects with this characteristic could experience high anxiety as a latent state. The proportion of anxiety, depression, and stress was higher in the female gender when evaluated with the DASS-21 test, but this contrasted with the results of the STAI test, where the highest proportion of subjects with anxiety was male.
Although this study was conducted during Phase 1 and the first days of phase 2 of the COVID-19 epidemic in Mexico, it has shown similar results to other investigations: Shigemura et al.27 considered that anxiety and fear were increased due to the excess of sensationalist news and the rumors or misinformation regarding the pandemic. A group evaluated the positive and negative emotional indicators of 17,865 active users of a social platform in China28 and reported that there was a significant increase in anxiety and depression when compared the periods from January 13 to 19 and 20 to 26 (p < 0.001).
Another study described a proportion of 50.4% anxiety and 71.5% stress29, which corresponds to Liu et al.30 who found 50.7% of participants with symptoms of depression, and 44.7% of anxiety, however, the subjects included in both studies were health-care professionals, and other scales were used to evaluate these indicators. Furthermore, Wang et al.31 identified proportions of depression (30.3%) and anxiety (36.4%) lower than those found in our study (41.3% and 48.8%, respectively), but the proportion of stress they found was higher (32.1% vs. 26.8%). The DASS-21 test was used in both studies, but only in our study, the proportions between gender and the scales of this test were compared.
In studies related to other pandemics such as AH1N1 influenza, a similar proportion of evasive behaviors such as anxiety was also found (41.2%), which was measured with the STAI test32. Williams et al.33 identified that negative perceptions of AH1N1 influenza showed a predictive value of anxiety state of β = 0.498. In 2018, a research group found that 48.4% of assessed subjects had at least one symptom of anxiety or depression related to their perception of the Ebola epidemic, and 76% showed at least one symptom of post-traumatic stress34. High anxiety means were also found in subjects evaluated using the STAI test in Hong Kong and Singapore during the SARS epidemic35.
Furthermore, it has been found that people with a low tolerance for uncertainty perceive pandemics as threatening situations36. These experiences of anxiety could explain erratic behaviors among the population, such as the intensification of obsessive attitudes in handwashing or the excessive use of disinfectant products, stigmatization of health-care personnel or people with respiratory diseases regardless of the etiology, and the panic buying derived from the feeling of uncertainty about the epidemic.
Other relevant data are the proportions of evaluated subjects who consider COVID-19 a disease invented by the government or a world conspiracy. Although these proportions are low, they suggest that misinformation persists in our society. Since one of the main sources of information used is social media, it is imperative to apply strategies that lessen the impact of fake news that spreads rapidly and that can lead to anxious states.
One of the most significant findings in our study was the proportion of subjects with anxiety classified as severe or very severe in the DASS-21 test, and the consistency of these results with high A/S and A/T levels in the STAI test. Although these levels of anxiety were not expected in the sample because the study was performed during the early stages of the epidemic in Mexico, this proportion could increase as reports of infections and deaths in our country multiplies. Regarding the care of children during the health contingency, the fact that this activity is carried out by women in a higher proportion highlights that this could contribute to the development of anxiety or other negative emotional states in this population, but determining this would require a study specifically designed with a gender perspective.
The study has potential limitations. First, it was not possible to achieve a homogeneous distribution of individuals, and the fact that the most of the sample had a medium socioeconomic status or a bachelor's degree could reflect other perceptions regarding COVID-19. Second, the age mean was not representative for older adults, which would require additional studies that include them; however, our study population coincides with other reports regarding COVID-19 pandemic28-31, in which age or academic degrees have similar proportions to our results37. Moreover, in this study, it was identified that anxiety had opposite proportions regarding gender in the tests used, but this could be attributable to the specific characteristics of each scale.
In summary, this study demonstrates that anxiety, depression, and stress are identifiable emotional states in the face of the COVID-19 epidemic and that they are found in almost half of our population, in different degrees of severity. This makes it necessary to consider them within the negative impact that this disease generates in the country and to establish specific measures for its prevention, diagnosis, containment, or treatment.
Conclusion
We identified that the emotional indicators (such as anxiety, depression and stress) derived from the 2019 coronavirus pandemic were presented in almost a half of the study population, which requires early treatment to improve the integral attention and to lessen the negative impact of the 2019 coronavirus disease.

