











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Ankle fractures are one of the most common injuries treated by orthopedic surgeons. (1),(2),(3),(4),(5),(6)
There are several existing classification methods for these injuries in keeping with biomechanical aspects (e.g. Launge-Hansen) (7) and with the anatomy of the fracture.
The two main anatomical classification methods are the number of malleoli involved (be they unimalleolar 2/3, bimalleolar 1/4, or trimalleolar 7%), (8) and the anatomical region of the fracture in relation to syndesmosis (be it infrasyndesmal, transyndesmal or suprasyndesmal). (9)
Both of these methods present us with good intra- and interobserver reproducibility. (10) Weber C type injuries represent 14 to 47% of ankle fractures. (11)
The tibiofibular syndesmosis is made up of the anterior tibiofibular ligament, the posterior tibiofibular ligament, the transverse tibiofibular ligament, the interosseous ligament and the interosseous membrane. (12) It provides stability to the mortise, along with its tolerance and resistance to rotatory and axial translation forces. (3)
In 1972, Danis and Weber demonstrated that in the case of infrasyndesmal fractures, the syndesmosis is not damaged. However, in the case of transyndesmal fractures, 50% show damage to the syndesmosis, and in supra-syndesmal injuries, there was a 100% damage rate to the syndesmosis. (13) It is known that 100% of Weber type C fractures have rupture of the syndesmosis, even without apparent radiographic alteration. (14)
There are various ways to test the stability of the syndesmosis: clinical stress tests in external rotation, (15) pain caused by direct compression (16),(17) and peroneal translation, (15) as well as X-ray examination. The X-rays may show a "clear tibiofibular space" less than 6 mm in size in AP and mortise views, or the overlapping of the anterior tuberosity of the tibia over the fibula. This radiographic measurement depends on the rotation of the foot relative to the X-ray beam direction. (18)
The main measurements in the AP and mortise X-ray projections were described by Merle D'Aubigné (Figure 1):
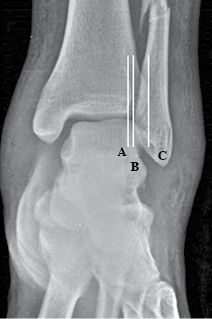
Figure 1: Merle D'Aubigné measurements; A. anterior tubercle of the tibia; B. border of the fibula; C. posterior tubercle of the tibia.
1. The "clear tibiofibular space", which is represented by the distance between the distal lateral border of the tibia and the medial border of the fibula. Normal: < 6 mm. (19)
2. The "tibiofibular overlap" is the distance between the medial wall of the fibula and the incisal surface of the tibia. Normal: > 6 mm or 42%. (19)
3. The "constant distance" between the two distal tibial tubercles. (18),(19)
The biomechanical instability caused by the syndesmosis is, without doubt, one of the most important predisposing factors for arthrosis of the ankle. (16),(20),(21),(22),(23),(24),(25)
There is a wide variety of tests, surgical interventions, and treatments (26) which ensure optimum care when maintaining the syndesmosis closed and stable when the fixation screw is removed.
The purpose of this study was to evaluate the changes in X-rays of the tibiofibular syndesmosis region (the tibiofibular clear space and the tibiofibular overlap) from the postoperative period to the transyndesmal screw removal in Weber C ankle fracture patients treated with open reduction, internal fixation and placement of a transyndesmal screw.
Material and methods
This is a retrospective study carried out in a cohort of patients with Weber C ankle fractures. They were surgically treated at "Hospital Regional del IMSS # 2 Villa Coapa", a level II trauma center in Mexico City. We included patients between 20 and 60 years of age. All had a transyndesmal fixed Weber C ankle fracture and complete radiographic registers in the preoperative phase of treatment, immediate postoperative before the transyndesmal screw withdrawal, and after its withdrawal (Figure 2) in the period between January 2014 and August 2014. We excluded patients with tibial pilon fractures, exposed fractures, complex injuries or direct trauma. The total sample was of 52 patients. The average age was 44.37 years (± 15.83); 30 were female (57.69%) and 22 male (42.31%) (Table 1).
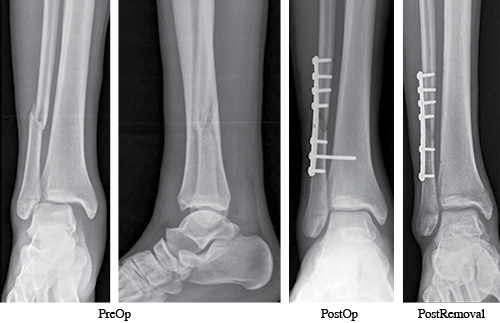
Table 1: Characteristics of the sample.
| Characteristic | Value |
|---|---|
| Age | 44.37 ± 15.83 |
| Female sex | 30 (57.69%) |
| Male sex | 22 (42.31%) |
Values expressed as mean ± SD; absolute frequencies (%).
We studied the radiographic registers of subjects who met the selection criteria. We registered the dates of the fracture, surgery and screw withdrawal, as well as age and gender. Measurements of tibiofibular clear space, tibiofibular overlap and intertubercular distance in each of the x-rays were also recorded.
The measurements were done in the IMPAX 6.4.0.5024 software system, using its included digital millimetric ruler.
Continuous variables were subjected to normality tests (Kolmogorov-Smirnov). All variables had a normal distribution and are thus described as mean, standard deviation, minimum, and maximum. The categorical variables were described as absolute and relative frequencies. Changes in the measurements during different stages of treatment that were considered: preoperative to postoperative; postoperative to pre-screw withdrawal; pre-screw withdrawal to post-screw withdrawal. The primary stage of treatment measured was the postoperative to post-screw withdrawal. The changes in the measurements were analyzed with a paired t-test. The management strategy of missing values was applied "by analysis". Data analysis was performed with IBM SPSS Statistics for Windows (V 16.0, Chicago). A two-tailed p-value of ≤ 0.05 was considered significant.
Results
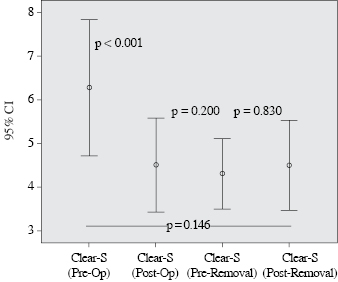
The mean time for the withdrawal of the trans-sindesmal screw was 55.56 days (± 21.83, 23-135) (Table 2). Taking into consideration the Merle-D'Aubigné measurement changes between the postoperative and after the withdrawal of the transyndesmal screw, we observed an increase of the tibiofibular overlap of 0.20 mm (± 2.29, p = 0.532); 0.21 mm (± 0.97, p = 0.146) in the tibiofibular clear space and 0.41 mm (± 2.08, p = 0.177) in the intertubercular distance (Table 3, Figure 3 and Figure 4).
Table 2: Mean time for removal of the syndesmotic screw.
| Value | |
|---|---|
| Time for removal of SS (days) | 55.56 (± 21.83, 23-135) |
Values expressed as mean (± SD, min-max). SS = syndesmotic screw.
Table 3: Radiographic measurements - Merle D'Aubigné.

Values expressed as mean (± SD). *Percent of change relative to initial value. TF = Tibiofibular; Clear-S = Clear Space; iT = inter-Tubercular. †T-test for related groups. Means and SDs are different in some cases due to the fact that missing data was pairwise suppressed during analysis.

Discussion
The relevance of fixing the syndesmosis as the most important predisposing factor of stability has been demonstrated by Weening and Bhandari. (27) Maintaining a reduced syndesmosis after the removal of the screw is equally important; thus the importance of the present study.
In this work, we found that after removing the trans-sindesmal screw, no radiographic variations were found, nor anything statistically significant in any of Merle D'Aubigné's measurements. The percentage of change in the radiographic measurements between the postoperative and the withdrawal of the trans-sindesmal screw was small: 2.38% change in the tibiofibular overlap, and 5.29% in the tibiofibular clear space. These changes were not statistically significant. The postoperative radiographic measurements may vary within a safe range. This finding does not necessarily have clinical relevance and does not mean that the original positioning of the screw was wrong or insufficient. It is also probable that in the operating theatre we tend to tighten a bit too much the syndesmosis with the screw.
Previous studies have assessed and compared multiple variables such as differences between surgical procedures, (28) the material with which the syndesmosis is fixed (metal versus titanium (29) versus suture, bioabsorbable or not (3),(30),(31)), the number of cortices, (32) the amount of screws, (33),(34) positioning, (35) the location of the screws, (35),(36),(37),(38),(39),(40),(41) their size, (42) and whether the screw is removed or not. (43),(44) In a previous analysis, Jordan, Talarico, and Schuberth analyzed the effect of the transyndesmal screw removal, as well as its effect on the syndesmosis. They concluded that there is not a significant difference with the withdrawal or in the follow-up. (45)
It is important to consider the variability of different X-ray technicians as projections may vary depending on several factors, including the patient's pain. Millimetric variations in the measurements may be due to these factors. Also, as we know, other important elements exist when it comes to stability, such as deltoid ligament repair. (46)
Given the fact that our inclusion criteria were ample, the results presented in this paper have a high degree of external validity (generalizability) to patients between 20 and 60 years of age with a transyndesmal fixed Weber C closed ankle fracture.
Syndesmosis injuries represent a challenge for orthopedic surgeons in the assessment of the injury, its management, stabilization, and repair.
There are still some issues to be addressed: the ideal number or cortices to be crossed with the syndesmal screw, whether to remove or not the syndesmotic screw, and the best timing for its removal.
With the results of this study, we were able to discover that after the withdrawal of the transyndesmal screw, there are no significant changes in X-ray measurements of the tibiofibular region.
It is clear that there is a difference between clinical and radiographic outcomes, and there is not always a correlation. The observed fact of a slight radiographic aperture of the syndesmosis does not necessarily mean ligamentous deficiency that translates to clinical stability.
In this study, we did not consider the inter-rater variability of radiographic measurements. Although the radiographic technique is standard and we can assume it is constant in all cases; we are aware that even slight variations in the position of the limb (i.e. rotation) may result in alteration of the radiographic measurements due to a variation of the X-ray beam (parallax error). There is a measurement, the intertubercular space, which in theory ought to remain constant due to its anatomical nature. However, we observed a mean difference of 0.41 mm (3.3%) between initial and final radiographic evaluations. We consider this variation as the result of a compound of inter-rater difference and measurement error. This fact might also have had an impact on the other measurements.
The small differences between the postoperative and post-removal periods of the tibiofibular overlap and tibiofibular clear space of 0.20 mm and 0.21 mm, respectively, might not be due to a failure in the syndesmal fixation. We believe that these slight variations could be a consequence of the normal process of screw removal and measurement error.

