











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Waste management practices pose an important challenge, especially for developing countries, due to the deficiency in waste generation data and difficulties in the management framework. In addition to the absence of waste management plans in healthcare facilities and the lack of available treatment options and appropriate disposal methods, making management efforts even more complicated1.
Studies on waste generated by health care facilities have been conducted mainly in secondary or tertiary level hospitals, such as specialized and highly complex hospitals because they are large waste generators2,3,4,5. However, the primary health care facilities have greater deficiencies in waste management than secondary or tertiary units. Although they do not provide hospitalization services, they carry out immunization activities, timely detection of cancer, dental services, laboratory analysis, among others. Thus, considerable amounts of waste6 are generated.
Most of the studies on health care waste management report conditions, quantities and composition in both Asian1,7,8,10and African countries2,10,11, but there are few studies in the Latin American context, especially in the primary health care establishments.3,6. In Sao Paulo, Brazil, an initial diagnosis in a primary health care center reported the absence of documents and certificates required by law, inadequate containers and bags, doubts about the management of expired medications and a lack of an autoclave for sterilization of infectious materials6.
In Mexico, the closest equivalent to regulate the waste management generated in healthcare establishments is the Mexican Official Standard NOM-087-SEMARNAT- SSA1-2002, Environmental Protection - Environmental Health - Biological-infectious hazardous wastes - Classification and handling specifications12 However, this standard only applies to the biological infectious type of waste and it does not consider the chemical pharmaceutical types such as medicines, vaccine residues or mercury, which are also generated by these health establishments. In addition, this standard classifies the waste generators according to the number of beds, and its scope does not include those with no beds, such as the primary healthcare centers.
The integral waste management in health care facilities occur within and consider five main stages figure 1: starting with identification, separation and packaging, collection and internal transport, internal treatment, temporary storage, and destination13.
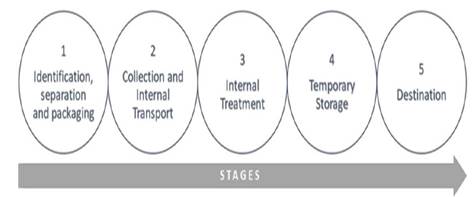
Figure 1 Integral waste management stages in health establishments Source: Compiled and designed by authors.
Regarding separation and packaging of waste, similar results were reported stating that this occurs in an unsatisfactory manner, mainly because the color coding is not respected, the containers are not made of the appropriate material or due to the lack of symbols that indicate the types of waste they contain, which are there to warn individuals about the damage they may cause, particularly when it comes to hazardous waste1,2,6,7,8.
Regarding transportation, 61% of the establishments studied had no dedicated equipment, specifically for transporting waste, while for storage, 60% have an area for temporary storage, but their conditions are not safe: they lack ventilation, inappropriate temperature or have inadequate localization (near the hospitalization areas or the kitchen)1. A case study on teaching hospitals from Iran reported that the storage time ranges from two weeks to one month before the waste is eliminated8. Likewise, one hospital in Venezuela, reported that the disposal of the total waste collected occurs outside the establishment, being left outdoors and, therefore, subject to the effects of the environment, rodents and indigent persons3.
According to a study carried out in hospitals of Addis Ababa, reported that there is no prior treatment of highly infectious laboratory waste before placing them in the common waste container the and only two of six healthcare facilities disinfect medical sharps objects after it is used2
The final disposal of waste depends on the type of waste generated. In the case of waste that cannot be treated internally, it must be collected by an authorized service provider. Only 63% of the establishments use an authorized company, the rest use their own vehicles or those of third parties, which did not meet the necessary conditions for the transport of hazardous waste1.
This study aims to assess the integrated waste management in primary health centers of the State Health Ministry of Veracruz, located in the municipality of Xalapa, Veracruz, Mexico.
Materials and Methods
This study was conducted in the health centers of the Secretary of Health from the municipality of Xalapa, capital city of the state of Veracruz, Mexico. According to the Unique Key for Healthcare Establishments (CLUES, its acronym in Spanish - March 2016) within the public establishments of the State Health Secretary of Veracruz, 944 healthcare centers and 63 hospitals are found, while in the Xalapa municipality there are 7 urban healthcare centers (primary care) and 4 hospitals (secondary level). This study was carried out in the seven urban healthcare centers located in the municipality of Xalapa. Each healthcare center was identified with a code in capital letters (A, B, C, D, E, F, and G).
For the data collection, a checklist was designed according to national and international regulations to determine the level of compliance at each waste management stage, which includes separation, identification and packaging, internal collection and transportation, internal treatment, temporary storage and destination. It contains 69 items and the evaluation score was determined by considering one if the specifications for each item were met, and zero if they were not met. Finally, the checklist was submitted to experts to validate its content by means of the group consensus method.
A database was created using the statistics software SPSS (Statistical Package for the Social Sciences) to process the information. One person was in charge of entering the information into the database. Data was cleared as it was collected. The compliance level of waste management was determined by adding each affirmative item of all the stages and was divided among the total of items applied. The results were expressed in proportions both partially for each stage of waste management and the total resulting from the evaluation of all the stages. Later, the scale used for the descriptive analysis was that proposed by Malekahmadi14, which categorizes the score obtained by each healthcare center as shown in table 1.
Table 1 Scale of waste management based on a score for compliance.
| Compliance percentage | Scale |
| 91-100 | Excellent |
| 71-90 | Good |
| 51-70 | Average |
| 26-50 | Low |
| 0-25 | Very low |
Source: Malekahmadi et al. (2014) Analysis of the healthcare waste management status in Tehran hospitals. Journal of Environmental Health Science & Engineering. 2014; 12(116).
Results
Each of the waste management stages is described and then waste management results yielded in the seven healthcare centers will be presented.
Identification, separation and packaging stage
Because the separation, identification and packaging stage differ according to the critical area where they are generated, the level of compliance in this stage was explored in each of the critical areas, as is shown in table 2.
Table 2 Compliance level of separation, identification and packaging stage in the critical areas of primary healthcare centers of Xalapa, 2016.
| Critical area | Healthcare center | Total % | ||||||
| A% | B% | C% | D% | E% | F% | G% | ||
| Inmunizacion | 60 | 80 | 100 | 60 | 80 | 40 | 60 | 69 |
| Nursing, preventive medicine | 100 | 40 | 60 | 60 | 60 | 60 | 60 | 63 |
| Dentistry | 75 | 75 | 86 | 75 | 75 | 75 | 75 | 77 |
| Pharmacy | 50 | 0 | 100 | 100 | 100 | 100 | 100 | 79 |
| Laboratory | - | 71 | - | - | - | - | 71 | |
Source: Compiled and designed by authors.
In the immunization area, it was found that, at healthcare centers A, F and G, syringes were discarded without prior rupture of the plunger, while in B and D we observed that the needles were discarded with everything including the hood. Similarly, in the area of nursing and preventive medicine, in six centers out of seven (B, C, D, E, F, and G) the needles are discarded with the hood and in some cases even with the syringe.
In the area of dentistry, the packaging of residual mercury represented the main reason for non-compliance, because although they are indeed available in containers under a water seal, these containers are sometimes made of glass, without any identification or a label of hazard warning symbols and date.
In the case of pharmaceutical waste, one of the main actions to be taken is to avoid the expiration of medicines. For this purpose, healthcare centers usually use a traffic light system on their shelves to control the flow of medicines. All of the centers, but one, achieved full compliance with this system.
Healthcare center C is the only one that provides clinical laboratory services.
Collection and Internal Transport
All the healthcare centers evaluated have signage of waste collection routes indicated with red arrows. Administrative staff are responsible for the collection of general or municipal waste, while hazardous biological infectious waste is usually transported by a nursing staff member. None of the seven centers evaluated had cars for waste collection, which is why the collection is done manually in all cases.
Treatment
In the healthcare centers that provide treatment, dry heat sterilizers are used for inactivating bottles and, in some cases, they are also used for sterilizing medical surgical instruments, because the equipment used for inactivating jars is inoperative. Healthcare center G was the only one where vaginal mirrors were disinfected with sodium hypochlorite before being disposed in the general waste container. For the chemical disinfection of an extracted dental organ, it was verified that in none of the cases were the concentrations of sodium hypochlorite used according to the recommendation.
Temporary storage
The availability of a specific area for the storage of infectious biological waste varies greatly and depended on the infrastructure conditions of each healthcare center. The period of time that the waste remains stored also varies for each healthcare center. At center A the waste has been stored for 7 years, while at center B its approximately 100 kg of waste had been managed by a trade union. Healthcare center C is the only one that is serviced by an authorized company, which is why their waste is stored for a period of 15 to 30 days maximum. At healthcare center D six months ago, waste was taken away privately. At healthcare center E the waste has been stored for three years. Healthcare center F has had their waste for six months, whereas center G for about 5 years.
The amalgam residues have been stored in the consultation rooms of the healthcare centers since they began to be packaged, and there was some uncertainty and ignorance about how it should be handled subsequently. There is no dedicated space for general waste to be stored or safeguarded until the municipal truck comes to collect it. Waste is left outdoors at all the healthcare centers, except center D, where the waste is stored in the public bathroom.
Destination
The destination of biological infectious waste in six of the seven healthcare centers evaluated is not managed by authorized companies on a regular basis. Keeping expired medicines is prevented in most of healthcare centers, so three months before their expiration date, medicines are organized to be donated or medical staff is notified to increase their use. General waste is arranged to be collected by the municipal trucks daily, every two or three days, depending on the location of the healthcare center.
Finally, in terms of the total compliance level of integral waste management of the seven evaluated healthcare centers the total score ranged between 47% to 63 %, median 55%, as shown in Figure 2. In the identification, separation and packaging stage, the level of compliance ranged from 56% to 77%; median 64%; in the collection and internal transport the values ranged from 46% to 73%; in the treatment, the level of compliance ranges from 40% to 60%; for temporary storage, the level of compliance was between 11% and 80% and, lastly, in the destination of waste, the level of compliance ranged from 40% to 60%.
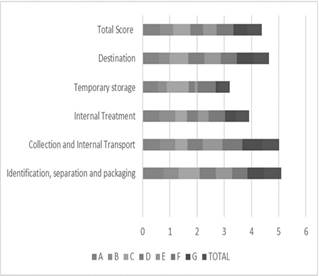
Figure 2 Compliance level of the integral waste management stages in primary healthcare centers of Xalapa, 2016 Source: Compiled and designed by authors.
Out of the above percentages, we see that the scale of compliance for healthcare centers A, C and F is of average compliance and healthcare centers B, D, E and G present a low level of compliance table 3.
Discussion
Previous studies mention that the identification, separation and packaging stage is one of the most critical stage of the process and that it is carried out unsatisfactorily1,6,7,8. This study found that this stage have the best level of compliance when compared to other management stages. The colors used for each type of waste vary according to the counüy’s policies and the generating establishment5,9,1,5. In the case of Mexico, the requirements that must be met by the bags and containers used for waste separation is correctly regulated by the Official Mexican Standard NOM-087-SEMARNAT- SSA1-200212, which establishes the use of the red color for blood residues, cultures and infectious type strains, non-anatomical and puncture-resistant waste; and yellow for pathological waste. There is no specific color for liquid waste. In the evaluated healthcare centers, it was found that most of them adhere to this color-coding system. In addition, it was observed that not all of the healthcare centers have red bags, and if they do, they are reused or placed only in order to show them in the event of an inspection, but in practice they are not used appropriately.
Despite having a color-coded system and the right containers will contribute to a better waste separation, complying with this aspect is not enough. It was identified that infectious waste and general waste is mixed, or needle hoods are disposed in containers for medical sharp objects. This inadequate separation of waste increases the volume of infectious waste and, therefore, the costs of treating it.
For vaccines that come in glass syringes with needles attached, according to the Vaccination Manual of the Ministry of Health16, it is recommended that all of it, including the needle, should be placed in red rigid containers. However, this process considerably increases the weight and volume of infectious biological waste. In all of the healthcare centers, with the exception of one, it was observed that glass syringes were eliminated in this way, and where this protocol was not followed, the nursing staff would separate the needle from the glass syringe with the aid of forceps, placing them latter with the vaccine bottles destined to be inactivated or, where appropriate, with the general waste.
All the evaluated healthcare centers have signage for waste collection routes. However, the signage is not respected at the time of waste collection. For the collection of waste, it is necessary to provide protective equipment such as resistant gloves, boots and a uniform or apron. None of the evaluated healthcare centers complied with equipment for full protection of the staff. Thus, the staff is exposed to spills, pricks or wounds. A study conducted by Sharma and Chauhan17 found that 16.67% of the staff that handled waste had suffered injuries or pricks in the last six months. However, this was not reported to the authorities, hence the importance of taking the necessary preventive measures. In addition to using protective equipment, the staff must be vaccinated. In 70% of the healthcare centers studied, the staff did not have all the basic vaccines against hepatitis B, tetanus and influenza. The World Health Organization18 recommends that the internal transport should be carried out in collection carts. However, none of the healthcare centers had any available. This is probably since the amount of waste generated daily is not as large as in hospitals.
The treatment method and their destination depend on the type of waste generated19. Some studies report the method of disinfection and crushing plastic waste to avoid their reuse and resale, as there are no guarantees of these not going back into circulation15,19. This study found out that the majority of the primary healthcare centers dispose them directly in the municipal trash.
Regarding needles treatment, some studies report the use of electric needle destroyers, which then send the waste to an authorized distributor, or using autoclaves to disinfect them before being buried5,20. None of the evaluated centers use needle destroyers or treat the needles before throwing them away in a red container.
The Vaccination Manual, by the Ministry of Health16, establishes that only viral vaccine residues need to be inactivated, for which the empty bottles or those containing leftovers are placed in an autoclave or pressure cooker at a temperature of 150°C for at least 20 minutes. Afterwards the contents are poured down the drain. In the evaluated healthcare centers, inactivation is mainly carried out by dry heat sterilization equipment, and there is no clear criterion regarding the temperature and duration of the process, so there is no guarantee that the inactivation is carried out correctly.
About storage, NOM-087-SEMARNAT-SSA1-200212 establishes that the generators included in Level 1 (where healthcare centers should be included) can store the infectious waste for a maximum period of 30 days. However, 85% of the urban healthcare centers located in the municipality of Xalapa do not adhere to this provision, because they are not considered in the collection route of the authorized service provider. Also, there is no formally established system for these healthcare centers to send the waste to authorized collection centers. The same happens with mercury waste and lead sheets generated in dental consulting rooms, meaning that most of them have large amounts of infectious waste stored in inappropriate conditions. The general trash stored outdoors may attract animals and represent health risks.
The highest average for the identification, separation and packaging of waste coincides with that reported by Kumar5.
Such average is followed by the collection and transport average, but the low level of compliance in the treatment and destination of waste hinder efforts to separate waste correctly, causing the process to be interrupted.
The highest average for the identification, separation and packaging of waste coincides with that reported by Kumar5. Such average is followed by the collection and transport average, but the low level of compliance in the treatment and destination of waste hinder efforts to separate waste correctly, causing the process to be interrupted.
The compliance level of waste management in the primary healthcare centers was medium to low, which makes the waste management criteria very heterogeneous. Unless the necessary measures are taken for adequate waste management, this situation will persist due to the lack of continuity in all stages of the waste management process. In addition to this, it is important to mention that cleaning, maintenance and waste management services are outsourced to third parties, leaving the governing and regulatory role to the Ministry of Health and other institutions, who exercise little supervision and place little emphasis on regulation compliance.
Waste management in health facilities is an ongoing process, which requires an integrated approach since generation to disposal, since deficiencies in one of the management stages render the efforts and resources invested less effective and efficient. In the primary healthcare centers located in the municipality of Xalapa, Veracruz. there is no systematic waste collection, which is evidenced in the inadequate storage and disposal of waste. This hinders efforts to separate waste correctly. Thus, the process is disrupted.
Conclusions
Globally and nationally, adequate waste management is a constant concern. The few studies carried out regarding waste generated in healthcare facilities, especially micro generators, show that they have not received the same level of attention when it comes to this type of waste.
The current situation in healthcare centers shows they are in a range of low to medium level of compliance, which makes the waste management criteria very heterogeneous. Unless the necessary measures are taken for adequate waste management, this situation will continue due to the lack of continuity in all stages of the waste management process.
In the urban healthcare centers of the municipality of Xalapa, Veracruz there is no systematic collection of waste, which is evidenced in the inadequate storage and disposal of waste. This eliminates efforts to separate waste correctly, thus disrupting the process.

