











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Almost 500 million people live with diabetes in the world. The president of the International Diabetes Federation reported that “diabetes is not just a health crisis”, It is a global social catastrophe. It causes devastating personal suffering and leads to poverty to families due to its chronic nature. Because of the great number of people with diabetes, all governments of the world are having troubles to face the problems related to diabetes care and this will remain a growth cost. As can be seen, the multiple factors related to a style of unhealthy life in the population are many and they are responsible for the uncontrolled rates of obesity and diabetes.
The problem of diabetes represents a great growing cost burden. The IDF has said that by 2017 the total health expenditure on diabetes would reach 727 billion dollars (people aged 20-79 years with diabetes), which represents an increase of 8% compared to the 2015 calculations. When using the wide age range group, 18-99, the costs amount to 850,000 billion dollars. A very high percentage of health spending is dedicated to the care of patients with chronic diseases; if measures that include therapeutic adherence are not taken this numbers will continue to increase, as is evident.
Mexico ranks 5th place of the ten territories in the world with the highest number of people with diabetes. In 2017, 12 millions of cases of people aged 20-79 with diabetes were registered. According to the FID projections, this problem would rank 4th place with an estimate 21.8 million cases in 2045.
Diabetes causes microvascular and macrovascular complications that bring deep psychological and physical problems to both patients and caregivers. The incidence and prevalence of this disease continues to increase throughout the world in spite of growing knowledge about risk factors and evidence of prevention programs.
México is one of the most affected countries in Latin America. In 2016, an announcement of diabetes epidemiological emergency was emitted in the national territory by La Secretaría de Salud. According to official data, it represents the second leading cause of death with 105, 574 cases in 2016.
In 2015, in Tabasco, Mexico, type 2 diabetes, one of the eleven important causes of death, ranked second place with 2, 283 cases registered.
It is in this sense that the need to take urgent measures before this health problem is exposed, where the responsibility of both the different sectors and the general population is joint. The empowerment of the patient in the management of his condition is considered as a viable alternative, conceptualizing it as the combination of abilities, motivation and opportunities of power. Empowerment begins when health professionals recognize that patients are in control of their daily diabetes care. Today, it is an urgent measure giving power to those who have in their hands the decision to take care of themselves and adhere to a treatment, and should be put into effect. Governments, health systems, non-governmental organizations and the family are a fundamental support in this cause.
Therefore, this study aims to analyze the relationship between the level of empowerment and Therapeutic Adherence with the glycemic control of patients with Type 2 Diabetes from a first level medical unit in Tabasco, Mexico.
Supporting materials and methodology
An observational, transversal and analytical study was designed, with the triangulation of the information of the applied instruments for deeper analysis. The population considered for this study were patients with Type 2 Diabetes treated and under treatment in a medical primary care unit of Villahermosa, municipality Centro, tabasco, Mexico throughout 2016 (N = 286). From the population described, the size of the sample was estimated by using the formula to obtain a proportion for finite populations, with a reliable data of 95% (Z2 = 1.96), a relative error (precision) of 10.0%, an estimated prevalence of 50.0%, in a total population of N = 286 people. A non-response rate (NRT) of 20.0% was considered. The calculated sample was 110 patients (n = 110), nevertheless, there was a non-response rate of 11.0% of the patients to be surveyed, leaving 100 patients to study. Simple random probabilistic sampling without replacement was performed, based on a census of patients with Type 2 Diabetes, obtaining n = 100 patients of the indicated universe, after selection of the statistical IBM © SPSS © Statistics software, 22nd version, and its application of generation of numbers random, used for that purpose, where all the participants had the same probability of being selected. A TNR of 11.0% was presented.
Inclusion criteria, having a diagnosis of Type 2 Diabetes, attending consultation to the medical care modules, being in treatment during the study period in the morning and evening shifts and participating with informed consent were considered. Glycemic control (glycosylated hemoglobin HgA1c) was the dependent variable; empowerment and therapeutic adherence were the variables of interest. Sociodemographic and clinical were Secondary or covariable variables.
A structured instrument was integrated in order to organize the procedures and collect the data for patients with Type 2 Diabetes, which included three sections; the first section serves for the patients’ identification and their sociodemographic, clinical and laboratory data (a clinical, methabolic and medical evaluation). The second incorporates the DES 28 Scale to measure the perception of the patients’ empowerment in their disease and the third one measures the therapeutic adherence based on the perception of the patients.
The questionnaire was applied and data was obtained from its medical, clinical and laboratory records with prior informed consent. In order to avoid systematic errors, a training of the personnel in charge of the activity was carried out for the correct application of the instrument. Weight and height measurements were taken from the medical records and from the last visit to his control. Personnel trained in somatometry conducted these measurements and the instruments used for their measurement were the scales of each medical office, carefully calibrated during the procedure.
A single instrument with four sections was integrated to collect the sociodemographic and clinical variables, as well as the empowerment and therapeutic adherence:
The personal data compilation sheet related to sociodemographic, clinical and laboratory information included the variables such as age, sex, occupation, marital status, schooling, residence, housing, economic dependence and metabolic control, as well as evolution time, compliance with the treatment installed, among others.
The normal glycosylated hemoglobin (HgAlc) was used as the gold standard, the results were obtain from the records one month prior to the study, for the purpose of determining if at the time of the study the patients were in control of their blood glucose levels.
The DES 28 Scale was used to measure the perception of empowerment in patients with diabetes, validated in the Hispanic population. A pilot test was conducted for the Validation of the scale and its items, as well as the verification of the reliability of the instrument using the coefficient A. Cronbach that presented a result of .874 for the scale, due to the cultural changes and idiosyncrasies of the Mexican population of the south-southeast region. The degree of empowerment in self-care was determined by using a Likert-type scale of 5 points (1= strongly disagree to 5= strongly agree). This scale evaluates self-control, self-efficacy, problem solving, psychosocial coping, support, motivation and decision-making.
Martin_Bayarre_Grau’s instrument of complementary Affirmations was used for the measurement of the perception of Adherence in patients, designed to evaluate adherence levels and describe their components. It consists of twelve items, divided into three factors: personal involvement, professional-patient relationship and compliance with the treatment, evaluated from the scores obtained in the items of the questionnaire. The categories that run through the operational definition of therapeutic adherence that is proposed were defined as follows: Compliance with Treatment (CT); it is the execution by the person of the prescribed medical indications, items 1, 2, 3, 4. Implication personal (IP); it is the search by the patient of strategies to guarantee the fulfillment of the prescriptions with the execution of the necessary efforts, items 5, 6, 8, 9 and 10. Transactional relationship (RT); this implies the collaboration relationship between the patient and his doctor to establish the treatment and to elaborate the strategy to follow that guarantees compliance and acceptance by both, items 7, 11 and 12.
Descriptive and inferential statistics were used for the data collection and statistical analysis, using the measures of central tendency and dispersion and the quantitative, continuous and discrete variables. The use of the table of simple frequencies with absolute, relative values (percentage) for each category of the variables analyzed was considered to analyze the qualitative and order qualitative variables. Subsequently, the transformation of the dependent variable and continuous independent to dichotomous categorical was carried out, using as cut-off points the normal and abnormal values of each scale and laboratory test used. Bivariate analysis was performed between the dependent variable: controlled and uncontrolled glycosylated hemoglobin (HbAlc), and the main variables, empowerment and therapeutic adherence. The application of the Pearson X2 test statistic was implemented as well as its degrees of freedom (gl) and the value of p<0.05.
Results
Characterization of the patient with Type 2 Diabetes (T2D), according to sociodemographic an biochemical control variables.
In the studied group, it was observed that patients with T2D have a mean age of T = 53.58 years, ds ± 11.53 years, minimum age of 25 years and maximum of 82 years, range of 57, median of 55.58 and mode of 55.50. The variable age was recoded in decades; obtaining six categories to compare that are shown in table 1, where the following results are observed: the decade from 55 to 64 years represented 39.0%, the decade from 35 to 44 years, 22.0%. The presence of patients aged between 25 and 34 years represented 5.0%, classified as T2D should be observed.
Tabla 1 Demographical and social characteristics of patients with type 2 Diabetes, medical primary health unit no. 1 located in Villahermosa, Tabasco, México, 2016.
| Sociodemographics | f | % | |
|---|---|---|---|
| Sex | Male | 28 | 28.0 |
| Female | 72 | 72.0 | |
| Ages in decades | 25-34 | 5 | 5.0 |
| 35-44 | 22 | 22.0 | |
| 45-54 | 16 | 16.0 | |
| 55-64 | 39 | 39.0 | |
| 65-74 | 17 | 17.0 | |
| 75-84 | 1 | 1.0 | |
| Scholarship | Illiterate person | 5 | 5.0 |
| Elementary | 43 | 43.0 | |
| Middle school | 42 | 42.0 | |
| High school | 10 | 10.0 | |
| civil status | Single | 10 | 10.0 |
| Married | 60 | 60.0 | |
| Divorced | 2 | 2.0 | |
| Consensual union | 15 | 15.0 | |
| widow(er) | 13 | 13.0 | |
| Occupation | homemaker | 68 | 68.0 |
| Active employee | 22 | 22.0 | |
| Unemployed | 5 | 5.0 | |
| Retired | 5 | 5.0 |
Source: Questionnaire.
According to the prevailing sex, it can be observed that the female sex is represented by a 72.0% of the total sample analyzed, in terms of the level of studies, elementary and middle school patients obtained the highest percentage by a 43.0 and 42.0% respectively, those who were married are represented by a 60.0% majority and 68.0% to homemakers. (Table 1)
According to the place of origin, most patients are from urban area and they are represented by an 84.0%; patients that live in their own home 76.0%, depend on their spouse economically 49.0%, live with a relative 76.0% and live on their own 16.0%. (Table 2)
Tabla 2: Characteristics According to economical and territorial location variables of patients with Type 2 Diabetes, medical primary health unit no. 1 located in Villahermosa, Tabasco, México, 2016
| Economical and territorial location variables | f | % | ||
|---|---|---|---|---|
| Residence | Urban | 84 | 84.0 | |
| Rural | 4 | 4.0 | ||
| Sub-urban | 12 | 12.0 | ||
| Housing | Own home | 76 | 76.0 | |
| Rendered - loaned | 17 | 17.0 | ||
| Rented | 7 | 7.0 | ||
| Economic dependence | Spouse | 49 | 49.0 | |
| Kids | 22 | 22.0 | ||
| Siblings | 5 | 5.0 | ||
| None | 16 | 16.0 | ||
| Others | 8 | 8.0 | ||
Source: Questionnaire
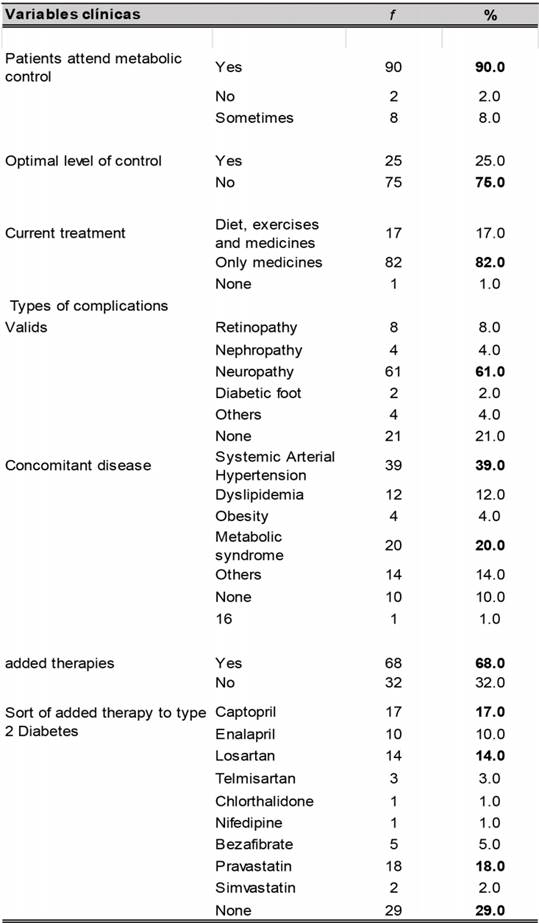
The clinical variables related to the control, treatment and complications of Type 2 Diabetes are as shown in (Table 3 and 4).
Tabla 3: Characteristics according to clinical variables of patients with type 2 Diabetes, medical primary health unit no. 1 located in Villahermosa, Tabasco, México, 2016.
Source: Questionnaire. Image with origin failures
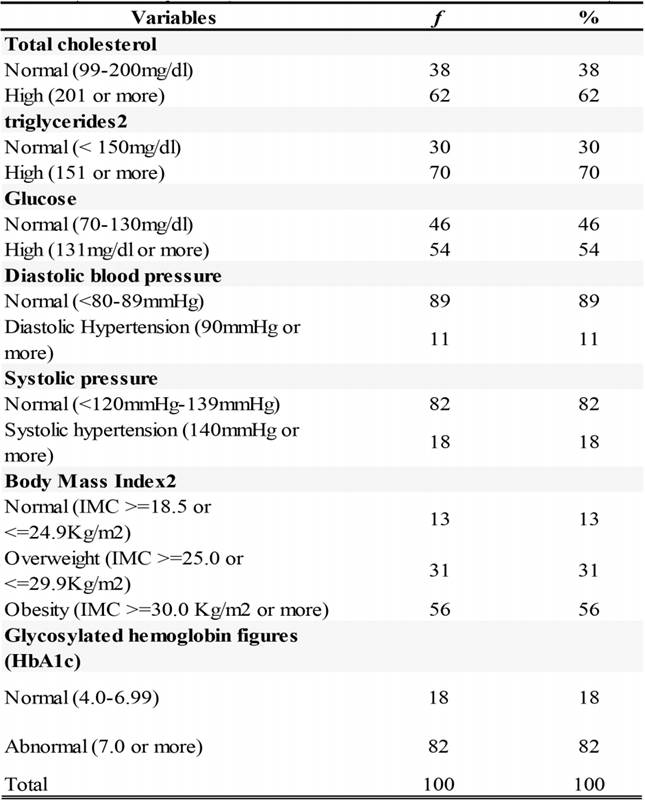
Tabla 4 Metabolic control and somatometry of patients with T2D, Medical primary health Unit no. 1 located in Villahermosa
Source: Questionnaire. Image with origin failures
Patient going to appointments for metabolic control are represented by a 90.0%, those using medications by an 82.0%, diet and exercise 17.0%. The main complications presented were diabetic neuropathy having a 61.0%, other white organs such as retinopathy, nephropathy, diabetic foot among others, together represent 18.0% and those who have no complications 21.0%.
With regard to comorbidities, arterial hypertension was present by a 39.0% of patients; using treatments added to DT2 68%, none of them 29.0%, pravastatin 18.0%, captopril 17.0%, among other antihypertensive drugs. (Table 3).
The average number of years of those patients suffering T2D was T = 8.96 years, ds ± 7.174 years, having a minimum value of 1 year and a maximum of 35,with a range of 34 years, a median of 7.00 and a mode of 5.0.
The variables of metabolic control and somatometry are expressed in table 4. The median of the glucose figure was T = 152.25mgs / dl, ds ± 53.317mgs / dl, having a minimum value of 49mgs / dl and a maximum of 334mgs / dl, with a range of 285mgs / dl, an average of 136.0mgs / dl, and a mode of 120.0mgs / dl.
The median of the triglycerides figure was T = 188.33mgs / dl, ds ± 78.530mgs / dl, having a minimum value of 71mgs / dl and a maximum of 652mgs / dl, with a range of 581mgs / dl, a median of 169.0mgs / dl and a mode of 150.0mgs / dl. The median of the systolic blood pressure figure was T = 121.84mmHg, ds ± 13,848 mmHg, minimum value of 90mmHg and a maximum of 160mmHg, with a range of 70mmHg, a median of 120.0mmHg, and a mode of 120.0mmHg. The median of the diastolic blood pressure figure was T = 76.09mmHg, ds ± 8.567mmHg, having a minimum value of 60mmHg and a maximum of 90mmHg, with a range of 30mmHg, a median of 80.0mmHg and a mode of 80.0mmHg.
The median of the weight figure in kilograms of patients with T2D was T = 73,648 kg, ds ± 15.1143 kg, having a minimum value of 46 kg and a maximum of 155.0 kg, with a range of 109.0 kg, a median of 72,250 kg and a mode of 80.0 kg.
An average size of T = 1.5529 m. was presented, with a ds±, 07809 having a minimum value of 1.37m. and a maximum of 174.0 m., with a range of .37cm., a median of 1.5350 m. and a mode of 1.50.0 m.
The median of the body mass index (BMI) was T = 30.8194Kg2, ds ± 5.32, having a minimum value of 19.53 and a maximum of 54.94, with a range of 35.41Kg2, a median of 30.79 Kg2 and a mode of 31.20 kg2.
The average abdominal circumference of the patients was T = 94.06 cm., ds ± 12.219 cm., having a minimum value of 65 and a maximum value of 140, with a range of 75, a median of 96.0 and a mode of 100.
The median of the glycosylated hemoglobin (HbA1c) was T = 8.07%, ds ± 1.44%, having a minimum value of 4.0%, and a maximum value of 12.8%, with a range of 8.8%, a median of 8.0% and a mode of 7.5%. According to the percentile, 25% of patients have HbA1c of 7.2%, 50% have HbA1 of 8.0%, and of 75% have HbA1c of 8.675%. The continuous variable glycosylated hemoglobin (HbA1c) was recorded into the normal, uncontrolled and pathological categories according to the WHO normative figures. It was observed that patients with Type 2 Diabetes under study were found with uncontrolled figures of 61.0%, in pathological figures they were found with 21.0% and the 18.0% of patients were found only with figures of <7.0. Once analyzed the outcomes, the variable glycosylated hemoglobin (HbAlc) was dichotomized in Normal / Control = 1, when values were observed 4.0-6.99 (18.0%) and Abnormal / uncontrolled = 0 when figures were observed > 7.0-12.99 ( 82.0%). (Table 4).
Level of empowerment of patients with Type 2 Diabetes.
This section describes the results of the analysis of the Empowerment instrument questions most frequently answered by patients: 1) identify with which actions of their health care in T2D is dissatisfied, 57% of them agree. 2). He is able to convert his goals into a practical and concrete plan of action to control his diabetes, 56% of them agree, 3). You can overcome obstacles and achieve your goals for the control of your diabetes, 61% of them agree. 4). Find ways to feel good even if you have the disease, 54% of them agree. 5). Know ways to face the stress that causes you to have Type 2 Diabetes, 58.0% of them agree. 6). Know where to find support to control your disease, 50% of them agree and 43.0% strongly agree 7) Know what helps you stay motivated to control your Type 2 Diabetes, 61% of them agree 8) Know enough to make the decisions that are convenient for your health care, 53% of them agree.
Empowered patients presented an 86%, and those without empowerment revealed a 14%, of the patients with empowerment, those who showed lack of control presented the 80.2% with an x2 of 1,300 and a value of p = .000. (Table 5).
Tabla 5 Perception of empowerment and adherence in patients with Type 2 Diabetes, Medical primary health unit no. 1, 2016
| Table 5. Perception of empowerment and adherence in patients with Type 2 Diabetes, Medical primary health unit no. 1, 2016 | |||
|---|---|---|---|
| Perception of empowerment | f | % | |
| Patients with empowerment | 86 | 86.0 | |
| Patients without empowerment | 14 | 14.0 | |
| Total | 100 | 100 | |
| Perception of therapeutic adherence | f | % | |
| Patients with adherence | 84 | 84.0 | |
| Patients without adherence | 16 | 16.0 | |
| Total | 100 | 100 | |
Source: Questionnaire. Image with origin failures
Therapeutic compliance (Bayarre Grau)
In this aspect the 68.0% of patients declared that they always take their medication in the established schedule, 72.0% of them always take all the indicated doses, 41.0% of them always comply with the indications related to the diet, 36.0% sometimes perform the physical exercises indicated in, 72.0% always attend scheduled follow-up visits, 63.0% always adjust their medication schedules to their activities or daily life, 77.0% of them always decide together with their doctor the treatment to follow, 74.0% always comply with their treatment without supervision of their family and friends, 80.0% always carry out the treatment without making great efforts, 51.0% always use reminders that facilitate the completion of their treatment, 73.0% always discuss with the doctor how to comply the treatment, and 75.0% always have the possibility to manifest the acceptance of the treatment prescribed by their doctor for their diabetes. The therapeutic adherence was present by an 84% of the patients and those without adherence were represented by a 16%. The 83.3% of the total of patients with adherence resulted uncontrolled with x2.632 and a value of p = .000. (Table 5).

Discussion
This study reveals that patients who feel empowered and adherent to treatment have inadequate glycemic control. Most participants in the study are women (72%), with an average age of 53 (± 11.5) years, a minimum age of 25 years and a maximum age of 82. The time of evolution with diabetes was less than 10 years; these data coincide with that observed by Alarcon-Mora and colleagues.
The elementary school level was the predominant scholarship in patients, revealing a 43%, and those living with a stable partner revealed a 62%. These results are similar to what reports Serrani-Azcurra in his study.
Almost all of the participants reported following a pharmacological treatment (82%), while glycosylated hemoglobin (HbAlc) was found in normal values in 18% (4.0-6.99), data differ from that observed by Urban-Reyes in its study, with more than 70% of patients with normal HbAlc. This could be because they are patients with fewer years of evolution with the disease.
The comorbidity that occurs most frequently in patients is related to arterial hypertension, similar to that reported by Aguilar and Urzua. The therapeutic adherence reached an 84% in our study, a fact that is similar to that observed by Bertoldo et al. and Castillo et al., In which compliance behaviors were greater than 60% and 70%, respectively. It differs with that said by Lopez-Simarro and collaborators, which it could be explained because most of the patients in their study were hypertensive.
The patient’s perception of empowerment related to the control of their disease is 86%. The literature consulted reveals that empowerment is related to a better knowledge of diabetes, better adherence and better self-care behaviors. We will have to work with more effective strategies for empowerment to be achieved, such as making a paradigm shift, moving from traditional care to patient-centered care, without neglecting aspects such as the gender approach in health, in this field there is still a significant lag of men who do not demand health care in the same proportion as women. Dominguez Mont points out in his study that “While the tasks of care are considered primarily feminine ... the de-modernization of health care practices will be little visible”. Although the instrument explores the perception of compliance with the therapy in the patient, it fails to measure in more depth determining factors such as type of diet, physical activity and other aspects related to their control, which could be causing the observed levels of glycosylated hemoglobin and other abnormal metabolic control variables. Investigating other factors and implement empowerment strategies are opportunities to achieve successful outcomes.
Conclusions
Patients who feel empowered and adherent to the treatment have inadequate glycemic control.
Most patients were women, homemakers, with elementary schooling, married, in a greater proportion they presented obesity, glycosylated hemoglobin and elevated lipids. Glycemic control is not compatible with the perception of empowerment and therapeutic adherence, this is reflected in the gold standard figures (glycosylated hemoglobin) and this allows researchers to conclude that in their study, patients have not really internalized the importance of care and responsibility of their health despite having attended their medical check-ups for several years.
The patient’s perception of being empowered and being adherent in the treatment is not enough to justify the figures of glycosylated hemoglobin decontrol presented in this research Taking a medication-only treatment, the patient’s perception of a diet and exercise, is not enough to obtain results that impact on the control of their glycosylated hemoglobin, because it is not clear how much the patient knows about his diet and also it is not clear how much and how he should exercise.
It is recommended to include variables of perception about metabolic control, obstacles, challenges, support elements and expectations in the patient for further studies.
Implementing effective empowerment strategies would be an opportunity to achieve successful outcomes.

