











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Type 2 diabetes mellitus (DM2) is a chronic and degenerative metabolic syndrome with a multifactorial aetiology and genetic basis that induce an abnormal metabolic use of sugars, proteins and lipids by the cells, there is a loss of carbohydrates tolerance, hyperglycaemia, glycosuria, polydipsia, polyphagia, and polyuria1. Thus because an insulin resistance in peripheral tissues and alterations in insulin secretion by the pancreatic p cells. These rises the glucose levels in blood and produces a damage in tissues and organs of the body with several complications, increasing the morbidity and mortality of this disease in the human population The hyperglycaemia in DM2 is a marker of the severity of this metabolic disease, more than the disease per se2'3.
In México since the year 2000, the federal health system reports that DM2 is the first cause of death among women, and the second among men4'5. The Mexican government invest 15% of their incomes for the treatment of DM2 patients; this is approximately 318 US million dollars per year6. The development of organic complications for this diseases, increase the economic costs in health services, and considering that most of the DM patients pay for most of theirs medical treatments such as the dialysis, haemodialysis, therapy with laser, drugs and surgical procedures such as the amputation of any extremity. Therefore, it is important to consider that the quality of life in these subjects became compromised with a decrease in many aspects of their life5-7.
A risk factor to develop DM2 is the overweight and obesity. The World Health Organization (WHO), reports each year 2.8 millions of adults decease for this cause, 44% of this population has DM2, 23% ischaemic heart disease, and 41% developed some kind of cancer, among many other complications8'10. The Pan-American Health Organization (PHO) and the WHO calculated that approximately 30% of the Mexican population suffers obesity11'13. The National Survey of Health and Nutrition in Mexico14'15, has showed that male population over 20 years old has higher risk factors, such as overweight and obesity, to develop DM2. The 50% of the population between 60 to 69 years old has overweight, 49% between 50 to 59 years old, and 45.1% between 40 to 49 years old. If overweight is not controlled it turns into obesity. In this population obesity is present in 34% of the persons in the range of 40 to 49 years old, 31.1% is in the range of 30 to 39 years old, and 28.7% is in the range of 50 to 59 years old. Therefore, they have a higher risk to develop DM27.
Because DM2 has increased dramatically around the world a team work of The International Diabetes Federation empathises the importance to identify the different life styles of the population to improve their health status, and to be a sensibiliser in the DM patients to become aware of the importance of their own health care in their own home setting. Therefore, the objective is to prevent clinical complication, and to lower the costs of this disease3,16. Previous studies with Hispanic17, Puerto Rican18 population in the United States and in Mexico19, using different prediction models for diabetes management and diabetic self'care20, have showed that health deterioration in DM2 patients are influenced by the lifestyle, health beliefs and level of acculturation. Pender21 designed a model for the health promotion in nursing practice and behavioural sciences, which is currently used. This health promotion model (HPM) has been used in different sample population to predict the lifestyle and specific behaviour of an individual. It is sustained with the concept that a change or modification in the lifestyle depends on the combination of the characteristics, experiences, knowledge and specific effects in the behaviour of each one, in order to generate a plan to improve the personal health22. HPM evaluates three characteristics in the subject: a) The individual characteristics and experiences, b) Cognitions and specific effects of the behaviour, and c) The results gained by the changes of specific habits to promote benefices and changes in the lifestyle of a person to improve their health condition. In this context, the aims of the present work is to determine the lifestyle and habits in a representative rural population with DM2. A health care model to promote the health status of the population was applied based on a questionnaire, in order to know how the lifestyle could affect the control of DM2.
Materials and methods
Sample population
This is a descriptive and transversal study carried out in a sample population previously diagnosed with DM2 at least one year before the research. The study was structured and divided into six phases: 1) Capacitation and training of the work team, 2) Self'care orientation to DM2 patients, 3) Laboratory analysis, BMI and GH, 4) Questionnaire application and recognition of the lifestyle, 5) Six month later laboratory analysis, BMI and GH and, 6) Analysis of the results.
The study was carried out in six clinical settings of first level belonging to different hospitals of the Federal Health Services (SESA) in the State of Tlaxcala, Mexico, from May 11 to November 16, 2015. The clinics in Amaxac de Guerrero, San Nicolás Panotla, Santa María Nativitas, San Juan Totolac, Santa Inés Zacatelco and Contla de Juan Cuamatzi were selected by convenience because their high incidence of DM2 adult patients, representing the 8.5% of all SESA hospitals in the State of Tlaxcala (Figure 1). A multidisciplinary team of health service professionals including nurses, physicians, and social service students participated in the study.
Source: Auíhor's original data: Tlaxcala, Tlax|., 2015. Map was retrieved from https://www.siem.gob.mx/siem/portal/estadisticas/iinage52/29.gif
Figure 1 Clinics in the rural communities of Amaxac de Guerrero. San Nicolás Panotla, Santa María Nativitas, San Juan Totolac, Santa Inés Zacatelco and Contia de Juan Cuaniatzi vvhere the questionnaires were appiied
One hundred twenty six subjects of both sexes, with an age range of 26-61 years old, belonging to the health care system were invited and recruited on the visit day to the physician consultation on the indicated date. Only those who accepted to participate, were included in the study. Those patients with some type of neurological alteration, physically handicapped, with major DM2 complications or pathologic disorders others than DM2, and those not interested in participating were excluded of the study. The patient’s clinical history included the body-mass index (BMI), height, weight, and glycosylated haemoglobin (GH) measurements. Laboratory analysis were obtained before the questionnaire application and six months later. A series of clinical orientation regarding the improvement of their lifestyle, nutritional advice, personal care, and regular exercise were given to all the patients after the first sample collection of blood.
Questionnaire application
The data for this study was collected in an individual semi- structured questionnaire using the Likert scale according to Pender21-22. This study was based on four sections of the questionnaire: a) sociodemographic (age, sex, education, sociodemographic status, social security, civil status, and number or accompanying persons living with the patient); b) a lifestyle and health practice; c) personal responsibility, and d) a lifestyle profile section23. It was divided into 43 items that were answered individually for each patient. The instrument was used in Spanish population and validated previously19. It was applied only once to each subject at the beginning of the study. Likert scale was elaborated according to the attitude regarding the style of life of the DM2 patients as follows: 0 - never, 1 - some times, 2 - frequently, 3 - routinely, 4 - no answer.
Statistical analysis
Percentages and frequencies were calculated from the total number of answers. The confidence of the questionnaire was determined with the alpha of Chronbach (.86). A statistical program (SPSS, v20) for social sciences was used for data analysis and to graphic the results.
Ethical Considerations
The study was performed in accordance to the Declaration of Helsinki24, and authorized by the ethical committee review board in the Faculty of Health Sciences and Nursing, belonging to the Universidad Autónoma de Tlaxcala, México. All participants got detailed information about the study to give their authorized consent to participate. The information collected was kept completely confidential.
Results
Sociodemographic characteristics of the studied population
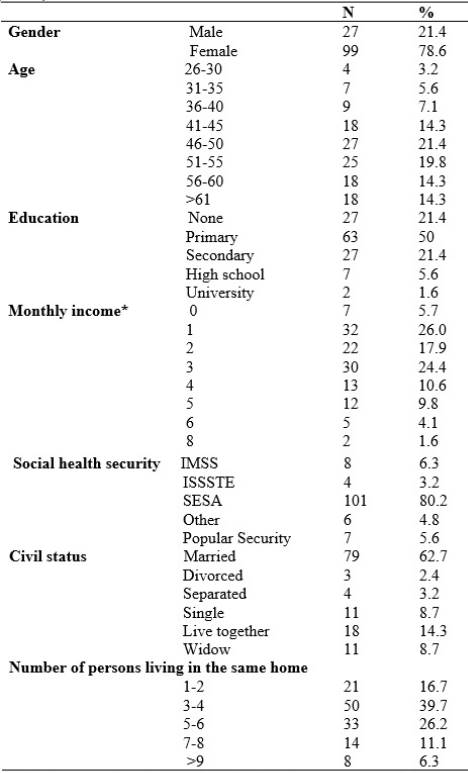
The study showed that 78.6% of the population are female and 21.4% male. Most of the subjects are in the range of 46 to 55 (41.2%) years old. The 77.4% are married or live together. The level of studies of most of the participants (50%) is up to primary, incomplete in the majority of the cases. The monthly income is in the range of one to three minimal salary in 74% of the population. Most of the population have access to health services by the government through the SESA (80.2%), IMSS (6.3%), ISSSTE (3.2%) and a popular community security service (5.6%); only the 4.8% of the population has access to private security health services. Most of the DM2 patients (39.7%) live with 3 or 4 members of the family, but none lives alone (Table 1).
Tabla 1 Frequency distribution of the sociodemographic characteristics of the studied population source: autor´s original data: Tlaxcala, tlax, 2015
Laboratory analysis
The BMI at the first time had a mean of 26.67 (range from 19.53 to 38.29) and after six months of orientation the mean was 26.36 (range from 19.53 to 38.31) as compared with a normal range of 24 -25 respectively. GH at the first time had a mean of 7.74 (range from 4.40 to 16.36), and after six months of orientation it was 7.33 (range from 4.80 to 10.60) as compared with a normal range from 4.00 to 6.00 respectively. No statistical differences before and after clinical orientation was determined in these subjects.
Lifestyle analysis
To identify the several aspects that can affect the lifestyle of DM2 patients, the questionnaire was divided in order to analyse the answers that are related to changes in habits of personal health care, nutrition, lifestyle, and exercise.
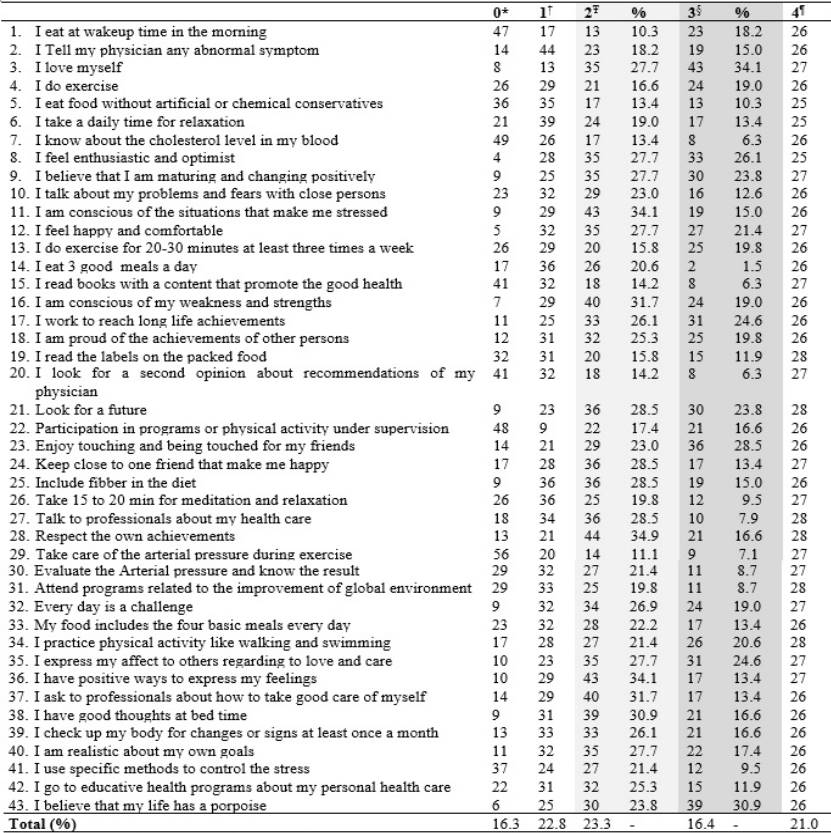
According to the questions and the percentages of the answers stratified by the Likert scale, the results were as follow: never (16.3%), sometimes (22.8%), frequently (23.3%), routinely (16.4%), and finally no answer (21.0%) (Table 2).
Tabla 2 Frequency distribution of habits and related situations in the lifestyle in DM2 patients. source: autor´s original data: Tlaxcala, tlax, 2015
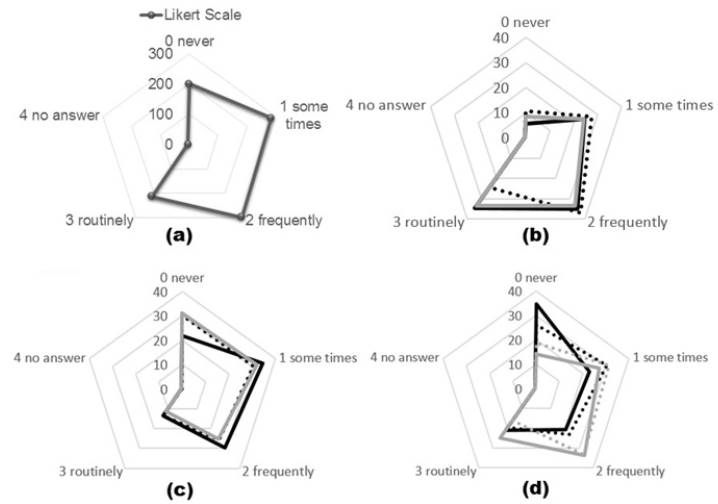
The questionnaire showed that 69.3% of the population is not aware of their status of life; 56.5% do not go with the doctor; 30.2% do not have interest in their health status; 39% do not know about their diseases; 34% do not practice any type of exercise; 56.6% is not or very few interested to get a good nutrition, and only 16.2% are conscious of doing exercise frequently. According to the significance of the lifestyle of DM2 patients the questions were grouped in 10 subscale items related to the health promotor model, and the total percentage of the answers were analysed and graphed (Table 3, Figure 2). The data indicate how the life style should affect the satisfying mode of life of the DM2 patients. More of DM2 patients answered that: just some time (1) or frequently (2) -in the Likert scale- are satisfied with their life style. A less number of DM2 patients answered that they routinely (3) take care of their own life style, and also they never (0) take care of their own health and life style (Figure 2a). Regarding questions 1 to 3, they showed that the feeling of the patients about their life, to get a mature behaviour and good feelings, and to get a vision of the future, are not so important or are not conscious that affect their life style (Figure 2b). The percentage of answers in questions 4 to 6, showed that the patients want to know more about the disease and how to get control of the DM2 (Figure 2c). The importance of a good life style in the DM2 patients related to the time that they dedicate to themselves, to do exercise, to enjoy their life style, to have a good nutrition and the importance of their own life, still have a lack of dedication among this population (Figure 2d).
Tabla 3 Percentage distribution and determination of lifestyle in DM2 patients according to the related grouped questions.
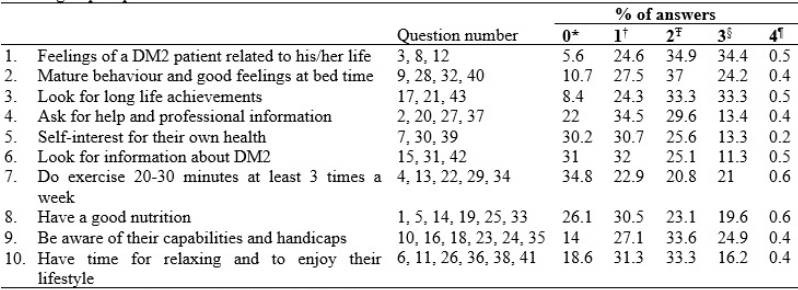
Source: autor´s original data: Tlaxcala, tlax, 2015
Figure 2 (a) Percent of total answers in the lifestyle in DM2 patients according to table 4 showing how theh data related to better life and health fills the graph up to the periphery, according to the likert scale, (b) answers related to questions 1 to 3:- questions, questions2, - questions 3, (c) answers related to questions 4 to 6: - questions 4, question 5, - question 6 (d) answers related to questions 7 to 10: - question 7, - question 8, - question 9, question 10,
Discusión
The sociodemographic characteristics of the studied population is an important factor in the life style of any DM2 patients. Most of the population is female with incomplete studies, and with an income that make difficult to get a good life style. It is also important to considerer that in these rural communities, men are more resistant to follow self-care instructions or accepting a physician treatment, and do not go to clinical settings. They are committed to labour work in the crops and settling animals mainly during the morning, being a cultural style of life difficult to remove from their believes. Women spend more time with their family at home, taking care of the young; they have the responsibility to prepare the food and to attend all the necessities of the family, including those related to the health. This is the main reason why the woman goes more frequently to the clinics and hospitals. These characteristics are similar among rural communities in México and has been reported previously by others researchers19-25. A fact is that most of the population have access to health services, however, the DM2 patients do not follow carefully the physician recommendations, probably because of a safe feeling of living with one or more of the family members that can take care of their main necessities.
Most of the population have DM2 after the 41 years old related to bad habits of nutrition, the time they dedicate to work, and eating fast food or non-nutritional food. Thus, the DM2 patient has to prepare their own food following home traditions without an appropriate healthy orientation. The lack of studies, low income to buy and prepare healthy meals have a relation to poverty, and furthermore, they do not have access to information to improve their lifestyle. The laboratory analysis showed no differences before and after clinical orientation that should reflect any change in the diet or lifestyle of the people, when the data is compare with the reference normal range. Our data was similar to the reported in others studies19-26, where the GH has a higher level than the normal range. Considering that most of them are adults with non-regular and non-healthy habits, the data reflects that the DM2 patients do not follow the indications of their physician even when all of them have access to social security services, and do not change their regular dietetic and exercise habits in order to improve their health status. Thus, because of a tradition of bad familiar habits transmitted from generation to generation. A lack of personal interest and health education have a relation to a low income and scholar level in most of the rural communities in Mexico6 27. Healthy programs should include clinical analysis more frequently in order to get control of the systemic health status of each individual, in order to improve the habits that can help to improve the lifestyle of the population.
We note that twenty-one percentage of questions were not answered, possibly because the patients feel ashamed of their own lifestyle, and they have the guilty feeling, as they note, that do not have a self-commitment in taking care of their own health. This is possible due cultural traditions focused in the people looking for cures rather than in the prevention of the disease or not having the self-commitment of looking after themselves. Thus, it is necessary that the personal of the health services should have a major influence in the cognitive development process to improve the behaviour related to the improvement of healthy habits among this population. However, counselling to improve the lifestyle given by a clinician to increase physical activity in these patients is not enough to improve their lifestyle28. Therefore, both the family of the patient and the nurse, play an important role in the improvement of the life of the DM2 patients, emphasizing that written counselling and instructions are better than only oral counselling. However, there is still some interest from the DM2 patients to cover all their necessities regarding their lifestyle but another important factor that can be considered is the lack of knowledge and education of the topic19.
Conclusions
These results show the necessity to increase both well- trained human resources and better educational community- based diabetes programs developed and implemented by the government, with the active participation of the rural communities and the society, in order to improve the health status and lifestyle of patients with DM2. This programs have to be continuous and nursing play an important role for clinical and care orientation of the population with higher risks to prevent the development of DM2.
The relationship between the income and life style is an important factor that affects the way the patient get a better medical treatment and the support of at least one member of the family. The goals of improvement of the health status and changes in the life style in patients with chronic degenerative diseases is a long time work that should be applied in all healthy programs if we look for a difference in the life style of the population. This could be used to prevent clinical complications of DM2 and other chronic degenerative diseases and to maintain a good human health in the own home setting. Healthy programs should be considered more frequently in order to change the habits that can help improve the health of the population. More research need to be done to know the causes why people in rural communities are not committed or interested in their own health. The community based programs to chronic diseases, such diabetes mellitus, should be consider the self- efficacy and low costs of the programs, continuous social support to the community, physiological and psychological outcomes in the patient, health-related influences (religion and beliefs, among others). Continuous health orientation by nurses and physicians for easily implementable primary and secondary prevention approaches to delay disease progression, complications and deterioration in patients with diabetes.

