










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista mexicana de trastornos alimentarios
versión On-line ISSN 2007-1523
Rev. Mex. de trastor. aliment vol.3 no.1 Tlalnepantla ene./jun. 2012
Artículos
Comparing Body Image and Risky Eating Behavior between Mexican and German Women
Comparando Imagen Corporal y Conducta Alimentaria de Riesgo entre Mujeres Mexicanas y Alemanas
Gilda Gomez-Peresmitré1, Bukard Jaëger2, Gisela Pineda Garcia3, Silvia Platas Acevedo MA1
1 Department of Psychology. National Autonomous University of Mexico (UNAM).
2 Department of Psychosomatics and Psychotherapy. Hannover Medical School.
3 Department of Social and Administrative Sciences. Autonomous University of Baja California (UABC).
Correspondencia:
Gilda Gomez-Peresmitré.
Department of Psychology.
National Autonomous University of Mexico (UNAM).
E-mail. gildag@unam.mx
Recibido: 28/02/2012
Revisado: 24/06/2012
Aceptado: 06/07/2012
Abstract
Background. Body dissatisfaction is regarded as a powerful risk factor for dietary restraint and bulimic behavior among women.
Objective. To compare Mexican and German women's body image and eating risk factors by developing structural models to find similarities or differences between the two samples.
Participants. The non-random sample of N = 404 (Mexican: 175; German: 229) medical and nursing students (total Mage = 20.6, SD = 0.86) answered standardized scales (EAT and EDI) and a culture-free 10-silhouette scale on body dissatisfaction.
Hypothesis. The main hypothesis proposed that Mexican women will show a stronger relationship between body dissatisfaction and restrained diet than the German women will.
Results.The findings confirmed this hypothesis by showing that in the relationship dissatisfaction-dieting, the Mexican group obtained the highest values of the correlation and determination coefficients, compared to the German group.
Discussion.Mexican women underestimated their body size, and it could be that body size underestimation lessens social pressure. It is concluded that whether this may be seen as a contradictory result or as a cognitive-defensive strategy in order to minimize the pressure experienced must be decided with further investigation.
Key words: Mexican and German women, body image, restrained eating, risk factors for eating disorders, structural models.
Resumen
Antecedentes. La insatisfacción corporal es un poderoso factor de riesgo para dieta restringida y conducta bulímica en mujeres.
Objetivo. Comparar imagen corporal y conducta alimentaria de riesgo en mujeres mexicanas y alemanas mediante el desarrollo de modelos estructurales detectando al mismo tiempo similitudes y diferencias.
Participantes. La muestra no aleatoria de N = 404 estudiantes de medicina y enfermería (175 mexicanas y 229 alemanas) con una Media total = 20.6 años (DE = 0.86) respondió a escalas estandarizadas (EAT y EDI) y a una escala de insatisfacción corporal de 10- siluetas libre de influencia cultural. Hipótesis. Las mexicanas mostrarán una relación más fuerte entre insatisfacción corporal y dieta restringida que las alemanas.
Resultados. Los hallazgos confirman la hipótesis, mostrando que el grupo mexicano obtuvo los coeficientes (de correlación y de determinación) más altos en la relación insatisfacción-dieta.
Discusión. Las mexicanas subestiman el tamaño de su cuerpo y se asume que dicha subestimación podría tener como propósito disminuir la presión social. Se concluye que si esto puede interpretarse como un resultado contradictorio o como una estrategia cognitivo defensiva para minimizar la presión experimentada debe decidirse con nuevas investigaciones.
Palabras clave: Mujeres mexicanas y alemanas, imagen corporal, dieta restringida, factores de riesgo en trastornos alimentarios, modelos estructurales.
Introducción
In Western societies, an extremely high value has been placed on physical appearance; slenderness is considered a symbol of attractiveness, beauty, and success in life. These kinds of values are characteristic of Western culture, which rapidly penetrates other communities as they develop socio-economically (Toro et al., 2006). The internalization of the current thin ideal promotes body image disturbances in the form of body dissatisfaction (BD) and body distortion (Thompson & Stice 2001; Wiseman, Moisimann & Ahrens, 1992). Body image disturbances may be seen as any form of affective, cognitive, perceptual, or behavioral disturbance directly related to concerns about body size or shape (Durkin & Paxton, 2002; Gowers & Shore, 2001).
These mostly negatively associated concerns -like negative self evaluation, low-self-esteem, and negative affect - may lead to a dieting behavior or dietary restraint (Stice, 2001). This eating behavior is widely accepted and promoted in the majority of post-modern societies as a measure of improving social acceptance and self-confidence. Thus, negative body image as a gendered factor widely extended within women of all ages is regarded as one of the most powerful risk factors for the development and maintenance of dietary restraint, bulimic behaviors, or Bulimia Nervosa (BN), and it has been found to be a prospective predictor of sub-clinical yet chronic eating disorders (Cooley & Toray, 2001; Thompson, Heinberg, Altabe, & Tantleff-Dunn, 1999).
Negative affect is a risk factor for dietary restraint and for bulimic behaviors; depression, stress and low self-esteem, among others, are some of its components (Stice, 2001; Stice & Shaw, 1994). Negative affect has been estimated by using the Ineffectiveness Scale of the Eating Disorders Inventory (EDI) (Garner, Olmsted & Polivy, 1983), which measures negative feelings like low opinion of oneself, low self-esteem, and feelings of inadequacy, among others. This same Ineffectiveness Scale was successfully used in a cross-cultural study in 12 countries (Jaeger et al., 2002).
Few cross-cultural investigations have been developed related to risk factors for eating disorders (ED), with fewer still in Latin American countries. Mexico is an exception in the past ten years cross cultural studies have been published conducted on Mexican and Spanish samples of adolescent students. Three of them (total mean age groups of 13, 16, and 17 years) utilized the same instruments in their search for differences and similarities in eating and behavior attitudes and reported a replication of the main results: the Mexican girls obtained higher percentages on restricted diets, as well as a higher body dissatisfaction than the Spanish girls did (Acosta, Llopis, Gomez-Peresmitre & Pineda 2005; Gomez-Peresmitre & Acosta, 2000; Gomez-Peresmitre & Acosta, 2002).
Another study compared the prevalence of ED, socio-cultural risk factors, and body image characteristics between Spanish and Mexican adolescents (total mean age of 14 years) (Toro et al., 2006). The investigators reported that the Spanish girls were more body dissatisfied than the Mexican girls were. However, one in four of the Mexican girls restricted their diet more than the German girls. Although the Mexican girls were less body dissatisfied, they had lost more weight in the previous year and reported more pressure (from peers or friends) to lose weight than the Spanish girls (260 in the Mexican sample vs. 17 in the Spanish sample).
Two other cross-cultural studies with Mexican (Mancilla et al., 2010) and Spanish (Raich et al., 2001) university women utilizing the same instruments (EAT 40) focused on eating attitudes and behaviors and body image. The Spanish girls, with a total mean age of 19 years, were more body dissatisfied and exhibited more eating disorders symptoms than the Mexican girls did. On the contrary, (Mancilla et al., 2010) found that Mexican women (with a total mean age of 21 years) had a higher rate of symptoms of ED than the Spanish women did, and that most Mexican girls had dieted and exercised in order to control weight. In all the studies, the Spanish girls were significantly taller than the Mexican girls were. In this way, the Mexican's BMIs were larger but the differences were not statistically significant (except for Mancilla et al., 2010).
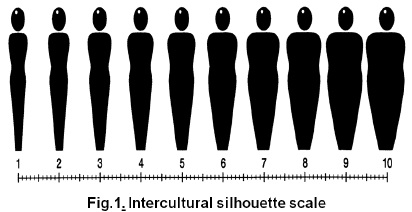
Studies on BD since 1983 (Thompson et al., 1999) have frequently used body silhouettes. In general, silhouette measures consist of schematic figures distributed within a weight range from underweight to overweight. The subjects' task is to select body silhouettes based on the perceptions of their current body size (actual) and their desired body size (ideal). Jaeger et al. (2002) designed and developed a set of silhouettes that were assumed to meet the requirement of being neutral to ethnic and cultural backgrounds, i.e., the silhouettes were faceless, hairless, and undressed because each one of these aspects could give a particular ethnic and cultural cue. The set of silhouettes was successfully applied in a multi-cross-cultural study, in which 12 different countries participated. Jaeger and coworkers (2002) found remarkable differences among those different cultures, influenced by the variability of the BMI. However, they also found that BD was similar in Western countries.
For years, researchers believed that eating disorders and with them, the risk factors that precede them, were exclusive to economically developed countries. However, some studies have shown that this is not so (e.g., the aforementioned studies conducted with Spanish and Mexican samples). This study aims to contribute to this knowledge, since some results have shown that today's adolescents in developing countries may have more risky eating behaviors compared with their counterparts in economically developed countries. In this way and taking into account the above background, the main objective was established for this study: To compare Mexican and German women's body images and eating risk factors by developing structural models to find similarities or differences between Mexican and German samples. It must be underlined that the theoretical assumptions that support the hypotheses of this study state that: a) A thinner the ideal figure be more body dissatisfaction will be experienced and b) Body dissatisfaction is a predisposing factor for the onset of restrained dieting (Brownell & Napolitano, 2006; Garfinkel & Garner, 1982; Stice, 1994). The hypotheses proposed were: (1) The Mexican girls will be more body dissatisfied than the German girls; (2) By comparing the two models (Mexican vs. German), the first group will show a higher ft weight on the path body dissatisfied—restrained diet, as well as higher explained variances (R2) on body dissatisfaction and restrained diet, than those of the German model. It is also assumed that a negative link will be found between (3) ideal and BD and (4) ideal and dieting.
Methods
Participants
Female medical and nursing students participated in the study. The total non-probabilistic sample (N= 404 females) was comprised of Mexicans (175) and Germans (229). The samples were matched in some of the principal demographical variables (sex, study area, school grade, and residence in urban demographic areas). The total mean age for Mexican and German students was 20.64 years, with a SD = 0.86. The mean age by group was Mexican women (Mage=20.4, SD = 0.49) and German women (Mage = 20.1, SD = 1.0).
Instruments
Body dissatisfaction. In order to measure body dissatisfaction (difference between actual and ideal figure) and internalization of the ideal thin figure (defined as the selection of a thin silhouette from a group of silhouettes of various body sizes), a set of 10 silhouettes assumed to be neutral to ethnicity, culture, and details (Figure 1) was used. A German work group (Jaeger, Massoubre & Lamprecht, 2000) originally developed these for a previous multi-cross-cultural study in a three-stage peer revision procedure. Four questions were asked in relation to the silhouette scales: "Please mark with a cross the silhouette that best represents the current shape of your body"; "What do you wish you looked like?"; "What is the most attractive silhouette in your opinion?"; "What do you find the most attractive silhouette in the opposite sex?" Participants were asked to mark with a cross the position representing their attitudes on a 0-10 decimal scale (Figure 1); positions between the two silhouettes were allowed and coded as real numbers. The authors reported the test-retest reliability as: Rtt= 0.82 ("actual"); Rtt= 0.77 ("ideal"); Rtt= 0.71 ("attractive"); and those of convergent validity as: Rcit= 0.73 ("actual" and BMI). The procedures followed by the authors, as well as the psychometric features, are described in detail elsewhere (Jaeger et al., 2002; Jaeger et al., 2000).
Dietary restraint. Dietary restraint was measured by the Dieting Scale of the Eating Attitudes Test (EAT) (Garner, Olmsted, Bohr & Garfinkel, 1982), comprised of 16 statements scored on a 6-point scale (never = 0/always = 5), with higher scores indicating a higher level of restrained eating. For the EAT psychometrical properties see Garner et al. (1982). The consistency coefficient for both samples, the Mexican and German ones, was of the same value, an alpha of 0.76.
Ineffectiveness scale. The negative affect factor was estimated through the Ineffectiveness Scale of the Eating Disorders Inventory (EDI) (Garner et al., 1983), which has shown a convergent validity (ineffectiveness/self esteem ) of R = 0.70 (p< .001). The Ineffectiveness Scale is comprised of 10 statements scored on a 6-point scale (never = 0/always = 5), with higher scores indicating a higher degree of ineffectiveness. The authors reported a reliability estimate alpha of 0.90 for the subscale. The consistency sample values were alpha = 0.70 for Mexican women and alpha = 0.85 for German women.
Body Mass Index (BMI). BMI was calculated as weight in kilograms divided by height in square meters (BMI = kg/m2). Medical personnel took the weight and height measures.
Procedure
Prior to data collection, a pilot study of the Silhouettes Scale (Figure 1), applied to a sample composed of 20 Mexican students, was used to test the appropriateness of the figures to represent body sizes, to corroborate a good acceptation of an unfamiliar set of silhouettes and a clear understanding of the instructions (the German group already counted with data in this respect). The results showed the Silhouette Scale was a good or an appropriate instrument for the Mexican sample.
The investigators of the two countries, at Mexico City and at Hanover, Germany, followed the same (standardized) procedure. The questionnaires were applied to groups of medical and nursing students at Mexican and German universities. One of the reasons behind the decision to choose samples of students related to medicine was precisely the interest that (one can assume) these young people should have for the medical field and for health issues, making them more responsive to problems like ED. Informed consent was obtained from all study participants. All the contacted students agreed to participate. The respective local ethics committees approved the non-invasive procedure. Professional translators undertook and controlled the translation and retranslation of the instruments.
Results
Preliminary analyses
Age. The mean age of Mexican women (Mage = 20.4, SD = 0.49) and German women (Mage = 20.8, SD = 1.0) differed statistically: t(346)= 4.29, p = 0.000. It is important to note that we expected not to find a significant difference in this variable, but a minimal difference of a few tenths (0.4) resulted in a significant one, most likely due to the large size of the total sample, since in separate structural analysis, age accounted for < 3% of variance in any variable.
Body Mass Index.(BMI =kg/m2). The BMI ranges for Mexican women were 16.9-36.2, with a M = 23.5 (SD = 3.3) and for German women, from 15.735.9, with a M = 21.3 (SD = 2.8), which elicited a significant difference at (p = 0.000). An examination of the height and weight data showed that German students were significantly taller than Mexican students were (MGerm = 169.5, SD = 6.6 vs. MMex = 159.1, SD = 6.6; t(395) = 15.5, p = 0.000) and that they weighed more than the Mexican women did (MGerm = 61.2, SD = 8.8 vs. MMex = 59.5, SD = 9.4), but they did not differ significantly; they only showed a marginal difference (t(392)= 1.8, p = 0.08). A review of height data shows that German women are taller (10 cm) than Mexicans, and although Mexican students weight less than their German counterparts do, one would expect a lighter weight given their height.
Attitudes Toward One's Own Body. Table 1 contains the results of attitudes toward one's own body with regard to the silhouette scale (Figure 1): all four estimates significantly vary between samples. With a Mean Silhouette Scale Position (MSSP) of 2.12, the Mexican women's 'most attractive' estimate was significantly slimmer (t(266.5) = 6.23, p = 0.000) than that selected by the German group (MSSP = 3.01), and their 'ideal' estimate (MSSP = 2.40 vs. MSSP = 3.31, t(260) = 5.41, p = 0.000) again represents a significantly slimmer figure. Taking into account a MSSP of 4.10 for the 'actual' estimate, this also results in a significantly larger (t(288.2) = -2.00, p = 0.046) "actual-ideal" difference (1.70) (Table 2), which is regarded as a measure of body dissatisfaction. In contrast, German women reported an 'actual' MSSP of 4.53 and, together with a comparable moderate 'ideal' MSSP of 3.31, this resulted in the same significant difference-score (p = 0.04) of 1.22 (Table 2) and one may conclude that Mexican women experience more body dissatisfaction than German women do. For women from both countries, the 'most attractive' estimate is slimmer than their 'ideal' MSSP. However, for Mexican women, this estimate is the slimmest (2MSSP) (See Figure land Table 1). Asking German women for the most attractive silhouette in the opposite sex German women's preferred for German men a MSSP significantly bigger than that for Mexican women (MSSP = 4.52 vs. MSSP = 3.64, t(266.5) = 6.23, p = 0.000).
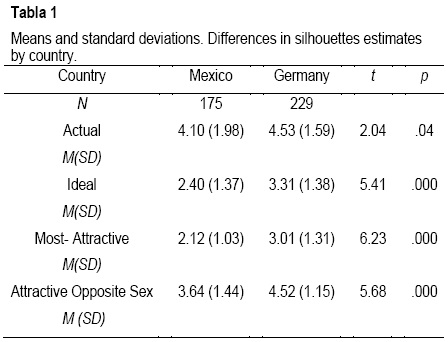
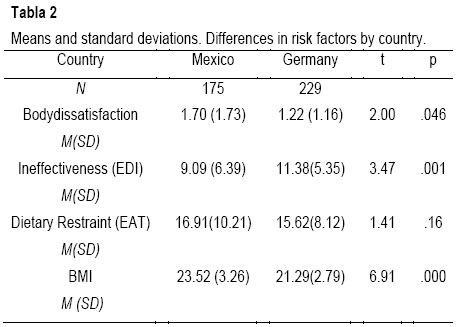
Risk Factors for Dietary Restraint. Table 2 provides the descriptive statistics and "t" results of the risk factors related to the development of dietary restraint ("restraint"), such as body dissatisfaction ("body-diss"), ineffectiveness and BMI, and it includes dietary restraint in order to know which group diets more. For practical reasons, Table 1 shows the risk factors of internalization of a thin ideal figure ("ideal") and that of actual figure ("actual"). It can be seen that Mexican "body diss" is significantly higher than that of the German "body diss" (170 vs. 1.22, p< 0.05); although the Mexican women's sample "restraint" mean was higher than that of the German sample (16.91 vs. 15.62, p = 0.0.16), the difference was not statistically significant. Conversely, the German sample's mean for ineffectiveness was higher than that of the Mexican sample (11.38 vs. 9.09, t(320) = 3.47, p< 0.01), but they did produce a significant difference. The BMI values revealed that Mexican women's BMI (23.5) was significantly higher (t(335.6) = 6.9, p = 000) than German women's (21.3). According to the obtained cutting points with a validated BMI scale with Mexican students, the Mexican women fall into the overweight category (BMI 23-27) (Saucedo & Gomez-Peresmitre, 1997), while the German women have normal weights. According to the World Health Organization (WHO, 1999) values, Mexican and the German women fall into the normal weight range, although the BMI of the Mexican women was significantly higher than that of the German women (Table 2).
Main Analyses
Statistical Indexes of Overall Model Fit.
In order to analyze structural interrelations, parameters and path models were set up (Maximum Likelihood Method) and tested via the Structural Equation Modeling analysis (SEM) by the AMOS 4.0 Statistical Programme (Arbuckle & Wothke, 1999; Bollen & Long, 1993).
The indices used to assess model fit, that is, the ability of a model to reproduce the data, were: 1) The chi-square tests to test the null hypothesis that the model has a good fit in the population, thus it shows what the researcher expects; 2) The root mean square error of approximation (RMSEA) measures the error of approximation and a value of zero indicates the best fit. Thus, RMSEA < 0.05 indicates close approximate fit, values between 0.05 and 0.08 suggest reasonable error of approximation, and RMSEA > 0.10 suggest poor fit; and 3). The normed fit index (NFI) defines the null model as a model in which all of the correlations or co-variances are zero. A value between 0.90 and 0.95 is acceptable and above 0.95 is good (Bollen & Long, 1993).
Structural models results.
In the Mexican women model (MWM) (Figure 2), the way Mexican women perceived themselves ("actual" figure) was highly related (0.95) to body dissatisfaction ("body-diss"). In the German women model (GWM) (Figure 3), the BMI of German women relates (0.58) to "body diss". Furthermore, the "actual" figure vanishes from the GWM, while in the MWM, the BMI does not disappear; rather, it correlates to "actual" (R = .69). "Actual" body and "ideal" body are correlated: R = 0.46 (the double-headed arrow between "actual and "ideal" estimates) (Figure 2).

In the analysis of the GWM and the MWM, we observed a direct link between "body-diss" and dieting, as well as a higher Beta load in the Mexican model (MWM = 0.60 > GWM= 0.36); also, the risk factor of body-dissatisfaction explains the 71% (R2=0.71) of the variance, while in the GWM, it only accounts for 26%. In the MWM and the GWM, there is a direct negative relationship (-0.41 and -0.27, respectively) between "ideal" and "body diss" and in the MWM, a direct negative link (-0.44) appears between the "ideal" estimate and dieting behavior. Thus, it can be said that to the extent that the "ideal" is slimmer, in that same measure, body dissatisfaction increased (for Mexican and German women), and dieting behavior increased (for Mexican women). No evidence of this last relationship exists in the GWM.
On the other hand, the ineffectiveness factor (negative affect) shows a direct low influence (0.19) on "dieting" in the MWM (Figure 2) and a small and negative influence (-0.008) on the same variable ("dieting") in the GWM. Of major importance is that this variable (in terms of its structure or relationships) for the GWM could be also appreciated, going back to Table 2, where ineffectiveness was significantly higher for German women than for Mexican women.
Discussion and Conclusions
It is worth noting that unlike in the traditional research, where there is a great deal of evidence supporting the development of dietary restraint as a predictive risk factor for the onset and maintenance of bulimia nervosa (Lowe, 1993; Polivy & Herman, 1985; Stice et al., 2000; Stice, Shaw & Nemeroff, 1998; Stice, 2001; 2002), in the field of cross-cultural research, there is no corresponding theoretical and practical support for this eating disorder. This work appears to be a first approximation in this regard.
Comparing the distributions of body attitudes by country, it can be stated that more risk indicators for dietary restraint were found in the Mexican women; for example, this group displayed a higher level of body dissatisfaction, which in turn, confirmed the results of antecedent studies (Acosta et al., 2005; Gomez-Peresmitre et al., 2000; 2002; Mancilla et al., 2010). This group also chose a thinner "ideal" figure, and the "most attractive" was the thinnest of overall figures chosen by both German and Mexican women. Based on theoretical and empirical backgrounds, it is assumed that a higher degree of body dissatisfaction, combined with the desire for aideally thin figure, is an indicator of greater perceived social pressure to be thin. At this point, it must be added that Mexican women are heavier than German women are, but their most attractive feminine figure is a slim one. Thus, if Mexican women are dissatisfied with themselves and striving to be thinner, as well as admiring and wishing for a slim figure, it may be naturally expected, as based on the literature, that there will be further consequences of social pressure (Stice, 1994; Stice et al., 1998), which must be investigated in new Mexican samples to gain more support for the findings of this study.
A surprising result is that the self-perception of Mexican women (the "actual" body estimate) starts in the fourth position of the silhouettes scale (Figure 1), a more or less slim figure, representing almost the same position that German women chose (to the middle of the fourth position), when the Mexicans are heavier than the Germans. This result confirms findings reported by Toro et al. (2006) in his study of Spanish and Mexican girls: more Mexicans (28%) than Spanish girls (18%) considered themselves thinner than average, when the Mexicans were heavier than the Spanish girls were. Looking at the German and the Mexican samples, it seems that Mexican women underestimated their body size, and it could be that body size underestimation lessens social pressure. Whether this may be seen as a contradictory result or as a cognitive-defensive strategy in order to minimize the pressure experienced must be decided with further investigation.
Another interesting finding yielded by the SEM-analyses was a strong and direct link between actual body and body dissatisfaction for Mexican women, while in the SEM analyses of the German women, there was a direct and significant pathway from BMI to body dissatisfaction. It seems that although members of the two women's groups are body dissatisfied, the Mexican women are the most dissatisfied (these results are consistent with those in Table 2, and in the same way, they confirm hypothesis 1). Besides, it is important to note that Mexican women's body dissatisfaction is linked with a subjective variable, self-body-perception (actual body), while body dissatisfaction among German women is linked with an objective measure (BMI). In fact, it can be seen that the subjective variable of self-body-perception ("actual") vanishes from the German model (Figure 3). It could be said that the subjective or the objective body evaluation could be a cultural difference. It would be interesting, then, to know if a particular feature of body perception (subjective/objective) makes any difference in the way one feels about one's own body image. In addition, if this response were positive, what would its effects on body image disturbances (dissatisfaction/distortion) be? At this point, it must be stressed that some results in structural parameters may point to interesting differences in culturally determined attitudes toward the body, which need to be addressed later.
On the other hand, the finding related to the presence of the path ("body-diss"— dieting) in the analyses of the German women, as well as in the Mexican women, the strongest Beta weight being provided by the latter (0.60 vs. 0.36) (See Figures 2 and 3) and the results related to the explained variance by the risk factor of restrained diet being higher for the Mexican Model than for the German one, 43% vs. 13%, respectively, confirmed hypothesis 2, and it appears to mean that the Mexican group is at a higher risk of developing bulimic symptoms than the German group.
Theoretical and empirical findings widely supported and documented this interrelation (Stice 1994; 2001; 2002). Furthermore, the higher load of influence of body-dissatisfaction upon dieting in the Mexican sample (0.60) confirms an independent study undertaken with Mexican samples (Unikel, Aguilar, & Gomez-Peresmitre, 2005). When these variables were inter-related within a SEM analysis, a direct influence was found, with a similar structural path and with the same beta-weight and positive interrelation (0.60). The replication of these results confirms that body dissatisfaction appears to be an important predictive or antecedent variable for the development of risky eating behavior, such as dietary restraint. In addition, the relevance of the role of the ideal figure on restrictive dieting among Mexican women must be highlighted. In Figure 2, it is evident that "ideal" relates to "restraint" directly and indirectly through body dissatisfaction (behaving in accord to hypotheses 3 and 4) with acceptable beta loads (> 0.40 < 0.60) respectively, while among German women, we can see only the indirect relationship (confirming hypothesis 3 and rejecting hypothesis 4) with lower beta loads (> 0.27 < 0.36).
Finally, it is important to stress that the main constraint of this study is its inability to generalize results to their respective populations (Mexican and German nurses and medical students) because of its sampling frame and the cross-sectional design, which does not allow temporal and causal relationships to be unambiguously interpreted. The study also relied completely on self-reported data, which should be supplemented in future studies with more precise analysis methods and data collection. In addition, more studies are required to test the hypothesis that cultural factors contribute to the different results (specifically with respect to ineffectiveness and that of the particular feature of body perception (subjective/objective), as well as the social pressure derived from the socio-cultural environment).
It is also suggested that future research on differences in risk factors for dietary restraint in these cultural domains should account for the different roles of the BMI in weight- and eating-related attitudes in women of both cultures. A detailed possible research question could be whether German women, being normal in weight and slimmer than the Mexican women are, entail more risky eating behaviors than Mexican women, being heavier, but underestimating their weight.
Acknowledgment. We want to thank the grant given to our study (the Mexican Research group) by the Support Program of Research Projects and Technological Innovation PAPIIT IN304011.
References
Acosta, G. M., Llopis, M. J., Gómez-Peresmitré, G. & Pineda, G. G. (2005). Evaluación de la conducta alimentaria de riesgo. Estudio transcultural entre adolescentes de España y México. International Journal of Psychology and Psychological Therapy, 3, 223-232. [ Links ]
Arbuckle, J. L. &Wothke, W. (1999). Amos 4.0 user's guide. Chicago, IL: SPSS. [ Links ]
Bollen, K. A. & Long, J. S. (1993).Testing structural equation models. Newbury Park, CA: Sage. [ Links ]
Brownell, K. D. & Napolitano, M. A. (1995). Distorting reality for children: Body size proportions of Barbie and Ken dolls. International Journal of Eating Disorders, 18, 3, 295-298. [ Links ]
Cooley, E. & Toray, T. (2001). Body image and personality predictors of eating disorder symptoms during the college years. International Journal of Eating Disorder, 30, 1, 28-36. [ Links ]
Durkin, S. J. & Paxton, S. J (2002) Predictors of vulnerability to reduced body image satisfaction and psychological well being in response to exposure to idealized female media images in adolescent girls. Journal of Psychosomatic Research, 53, 995-1005. [ Links ]
Garner, D. M., Olmsted, M. P., Bohr, Y. & Garfinkel, P.E. (1982). The eating attitudes test: Psychometric features and clinical correlates. Psychological Medicine, 12, 871-878. [ Links ]
Garner, D.M., Olmsted, M.P. & Polivy, J. (1983). Development and validation of a multidimensional Eating Disorder Inventory for anorexia nervosa and bulimia. International Journal of Eating Disorder, 2, 15-34. [ Links ]
Gómez-Peresmitré, G. & Acosta, V. (2000).Imagen corporal como factor de riesgo en los trastornos de la alimentación: Una comparación transcultural entre México y España. Revista Clínica y Salud, 11, 2, 35-58. [ Links ]
Gómez-Peresmitré, G. & Acosta, V. (2002). Valoración de la delgadez. Un estudio transcultural (México/España). Psicothema, 14, 2, 221-226. [ Links ]
Gowers, S. G. & Shore, A. (2001). Weight and shape concerns in the development of adolescent anorexia nervosa. British Journal of Psychiatry, 179, 236-242. [ Links ]
Jaëger B., Massoubre C. & Lamprecht, F. (2000). Psychometrische Eigenschaften einer Silhouettenreihe zur kulturneutralen untersuchung von körperlichem selbstbild und schlankheits-wunsch. In Lamprecht F., Schmidott G, Kuensebeck HW (Eds): Neue und alte Betätigungsfelder der Psychosomatik and Psychotherapic, 218-228 Frankfurt, VAS. [ Links ]
Jaëger, B., Ruggiero, G.M., Edlund, B., Gómez-Perretta, C., Lang F. & Mohammadkhani, P. (2002). Body Dissatisfaction and Its Interrelations with Other Risk Factors for Bulimia nervosa in 12 Countries. Psychotherapy Psychosomatic, 71, 54-61. [ Links ]
Lowe, M. R. (1993). The effects of dieting on eating behavior: A three-factor model. Psychological Bulletin, 114, 100-121. [ Links ]
Mancilla, D. J., Fernández, L. M., Vázquez, A. R., Alvarez, R. G., Franco, P. K., López, A. X. et al. (2010). Influencias socioculturales y conductas alimentarias o saludables en hombres y mujeres de España y México. Revista Mexicana de trastornos alimentarios, 1, 36-47. [ Links ]
Polivy, J. & Herman, C. P. (1985). Dieting and binge eating: A causal analysis. American Psychologist, 40, 193-204. [ Links ]
Raich, R. M., Mora, M., Sánchez-Carracedo, D., Torras, J., Viladrich, M.C., Zapater, L. et al. (2001). A cross-cultural study on Eating attitudes and behaviours in two Spanish-speaking countries: Spain and Mexico. European Eating Disorders Review, 9, 53-63. [ Links ]
Saucedo-Molina T. & Gómez-Peresmitré, G. (1997). Validez diagnostica del índice de masa corporal en una muestra de adolescentes mexicanos. Acta Pediátrica de México, 18, 19-27. [ Links ]
Stice, E. (1994). A review of the evidence for a socio-cultural model of bulimia nervosa and an exploration of the mechanisms of action. Clinical Psychology Review, 14, 633-661. [ Links ]
Stice, E. (2001). A prospective test of the dual-pathway model of bulimic pathology: Mediating effects of dieting and negative affect. Journal of Abnormal Psychology, 110, 124-135. [ Links ]
Stice, E. (2002). Risk and maintenance factors for eating pathology: A meta-analytic review. Psychological Bulletin, 128, 825-848. [ Links ]
Stice, E., Akutagawa, D., Gaggar, A. & Agras, W. S. (2000). Negative affect moderates the relation between dieting and binge eating. International Journal of Eating Disorders, 27, 218-229. [ Links ]
Stice, E. & Shaw, H. (1994). Adverse effects of the media portrayed thin-ideal on women and linkages to bulimic symptomatology. Journal of Social and Clinical Psychology, 13, 3, 288-308. [ Links ]
Stice, E., Shaw, H. E. & Nemeroff, C. (1998). Dual pathway model of bulimia nervosa: longitudinal support for dietary restraint and affect-regulation mechanisms. Journal of Social and Clinical Psychology, 17, 129-149. [ Links ]
Toro, J., Gómez-Peresmitré, G., Sentis, J., Valles, A., Casulá, V., Castro, J. et al. (2006). Eating disorders and body image in Spanish and Mexican female adolescents. Social Psychiatry and Psychiatric Epidemiology, 41, 7, 556-565. [ Links ]
Thompson, J. K., Heinberg, L. J., Altabe, M. & Tantleff-Dunn, S. (1999). Exacting beauty: Theory, assessment, and treatment of body image disturbance. Washington, D. C: American Psychological Association. [ Links ]
Thompson, J. K. & Stice, E. (2001). Thin-ideal internalization: mounting evidence for a new risk factor for body-image disturbance and eating pathology. Current Directions in Psychological Science, 10, 5, 181-183. [ Links ]
Unikel, C., Aguilar, J. & Gómez-Peresmitré, G. (2005). Predictors of eating behaviors in a sample of Mexican women. Eating and Weight Disorder, 10, 9-33. [ Links ]
Wiseman, C.V., Gray, J. J., Mosimann, J. E. & Ahrens, A. H. (1992).Cultural expectations of thinness in women: An update. International Journal of Eating Disorders, 11, 85-89. [ Links ]
World Health Organization. (1999). Obesity: preventing and managing the global epidemic. Geneva: Report of a WHO convention. [ Links ]

