










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista mexicana de ciencias agrícolas
versão impressa ISSN 2007-0934
Rev. Mex. Cienc. Agríc vol.6 no.8 Texcoco Nov./Dez. 2015
Articles
Knowledge in traditional medicine and its contribution to rural development: case study Totonac region, Veracruz
1Postgrado en Socioeconomía, Estadística e Informática-Desarrollo Rural. Colegio de Postgraduados. Campus Montecillo. Carretera México-Texcoco, km 36.5. C. P. 56230, Montecillo, Estado de México. (pascual.jimenez@colpos.mx).
2Colegio de Postgraduados. Carretera México-Texcoco, km. 36.5. C. P. 56230, Montecillo, Estado de México. (gildardo@colpos.mx).
3Universidad Autónoma Chapingo. Carretera México-Texcoco, km 38.5. C. P. 56230, Chapingo. Estado de México. (plantasmedicinaleschapingo@yahoo.com.mx; torrijos.marcia@colpos.mx).
The threat to biodiversity in rural areas persists mainly by high rates of deforestation, the expansion of the agricultural frontier, and the contamination of soil and water. The so close links between this cultural diversity in the territories of indigenous peoples make suppose an erosion of indigenous knowledge, linked to the use and exploitation of their plant genetic resources. This study analyses the process of transmission and exchange of knowledge on traditional medicine in two ways: 1) between family members; and 2) between traditional medicine and its complementarity with allopathic medicine. The study was conducted in 2013 in the Totonac region of the State of Veracruz. 53 questionnaires to heads and four key informant interviews were applied to disclose the acquisition and transmission of knowledge and the syncretic act of attention. The results show that traditional medicine still represents an important practice for the health care of members of the family and are the mother and father who favour the transmission of this knowledge to the children through the induction consumption of home remedies; however, gradual loss of knowledge of their ancestors is perceived. Although traditional medicine is kept at the local level and uncommercial in practice to coexist with allopathic medicine, where the actors recognize their respective areas of competence and benefits.
Keywords: health, joint attention; medicinal plants, Totonac region, traditional knowledge
La amenaza a la biodiversidad de las áreas rurales persiste principalmente por las altas tasas de deforestación, la ampliación de la frontera agrícola, y la contaminación del suelo y agua. Los vínculos tan estrechos entre ésta con la diversidad cultural en los territorios de poblaciones indígenas, hacen suponer una erosión de los saberes autóctonos, vinculados al uso y aprovechamiento de sus recursos fitogenéticos. Este estudio analiza el proceso de transmisión e intercambio de saberes en medicina tradicional en dos vertientes: 1) entre integrantes de la familia; y 2) entre la medicina tradicional y su complementariedad con la medicina alópata. El estudio se realizó en 2013 en la región Totonaca del estado de Veracruz. Se aplicaron 53 cuestionarios a jefes y cuatro entrevistas a informantes clave para conocer la adquisición y transmisión de conocimientos, así como el acto sincrético de la atención mixta. Los resultados muestran que la medicina tradicional aún representa una práctica relevante para la atención de la salud de los miembros de las familia y son la madre y el padre quienes propician la transmisión de estos conocimientos hacia los hijos e hij as a través de la inducción en el consumo de remedios caseros; sin embargo se percibe pérdida paulatina de saberes de sus antepasados. Aunque la medicina tradicional se mantiene en el nivel local y poco comercial, en la práctica coexiste con la medicina alópata, en donde los actores reconocen sus respectivos ámbitos de competencia y beneficios.
Palabras clave: atención mixta; plantas medicinales, región Totonaca, saberes tradicionales, salud
Introduction
Currently, in Mexico the gardens and orchards in the backyard of the family are a great vegetable wealth due to the high degree of diversity, complexity and anthropocentric uses. Mendoza (2011) compared the level of use and management in urban, suburban and rural areas (Estomba et al., 2006) which is in rural areas where greater acreage of plants for therapeutic purposes, it is there where there is more diversity, better handling and more knowledge compared to suburban and urban areas, and where the woman is who plays a major role in preserving (OMS, 1995; Zapparoli, 2012).
Herbal medicine has been traditionally regarded as a basic therapeutic alternative for a large segment of the rural population without access to modern allopathic medicine. Laurell (1975) Jorand (2008) mentioned that, the rural and urban lumpenproletariat do not constitute a significant market for private medicine for its low level of income, and in traditional medicine are a means to preserve their health, which is known as calls "green social security" (Cunningham, 2002). From the point of view of rural development, it is established that, the loss of genetic diversity of plants can be stopped by the farmers, if they contribute with their millennial wisdom to establish gene banks in the dynamic space of the backyard or their plots (Cuevas, 1991). Additionally, it is considered that the systematization of knowledge through studies and encourage the rescue from the family garden or plot with special participation of the domestic group will always be the central element in order to apprehend the traditional family medicine (Jorand, 2008).
The use of medicinal plants has become increasingly important as a therapeutic option for the important role acquired in the overall health of rural communities by reducing significant costs for much of the population lacks full or partial coverage of the public health system, so rural development programs should promote the recovery of these alternatives for their contribution for improving the social, economic and environmental well-being. In this sense, Mata (2002) refers to rural development as: "... the economic and social process that takes place in traditional rural societies and tends to improve the welfare of the rural population through actions such as introduction of modern technologies and the provision of social services (...) in order to increase income (ratio between production and household consumption) and improve the quality of life of the majority of the rural population".
Bañuelos (2007) notes that indigenous knowledge regarding the use and conservation of plants linked to culture, identity, territory and development; i.e. plant resources are considered a product of culture. Unfortunately that knowledge, wisdom and everyday expressions are lost by the pressure of modern industrializing society, and Cuevas (1991) argues that the elimination or drastic alteration of human groups inherent in rural cultural attributes, promotes loss of important traditional knowledge and attitudes related to the interpretation and use of the plant. Meanwhile Bartoli (2005) shows even more extreme in predicting the disappearance of traditional expertise, due to the lack of young people to learn and prepare to take over from the old traditional medical settings; and Foucault (1982) indicates that hegemonic medical practices transform, move and even eliminate this popular knowledge.
In the practice of health care in the rural sector it has been developed a model of joint attention or convergence where coexist both traditional medicine and allopathic (Bejarano, 2004; Espinosa, 2009). However, the choice of using one or other health care (allopathic doctor or healer), also depends on the perception of the signs and symptoms that are the disease and the preconception of the sufferings that have either natural or supernatural,l from the body or the spirit. The mixed model of health care is defined by Espinosa (2009) as "a concept that is not limited to the past, but how knowledge (popular and scientific) are socialized and incorporated into the daily life of individuals and communities, and in the possibility of building new knowledge, theories and practices "and not limited by the cultural diversity, the obstacle is the relationships of hegemony and subordination that ultimately results in domination and subordination, which comes diminished the participation of traditional medical and yields to the power of " themedical knowledge learned" (Bejarano, 2004).
In this context, the need for intercultural dialogue is recognized between biomedical and traditional knowledge in hospital and community care; however, it is also where most cultural barriers that prevent or limit communication and make a complementary and not antagonistic conditions as it should be noted (Espinosa, 2009). In this context, two worlds intersect: a primitive, sage and natural; and another novel, sophisticated and artificial (Prieto, 2004). Duarte (2004) recognized the advances in the joint attention in Mexico; however, underlining their intentions to consider a delay of traditional medicine in the field of national medical culture and not enough progress in giving voice and autonomy to the communities to decide their relationship.
In the traditional view, is known to be a common practice that the traditional healer or doctor intuit based on the origin of the disease and distinguished four major causes according to Eroza (1996): the first natural, sickening are those factors which directly affect the physiological status of individuals; the second related to social transgressions to the collective rules, which in this case result in the appearance of certain diseases; the third, whose calendrical causes damage the health and are associated with certain periods and scales, as well as the position of the stars, as they express a dichotomous nature of the universe, including taxonomy grouped by hot-cold system disease; and finally, the indigenous cosmogony, those illness caused by various divine and supernatural beings ready to affect agents, also called cultural affiliation (Jorand, 2008).
The indigenous world around medicinal plants reflects family, economic, consumption levels and builds social organization, where such practices and knowledge can promote economic and social development of the community (Bañuelos, 2007). Thus, the objective raised in this research was to analyse the process of transmission of knowledge of traditional herbal medicine, its complementarity with allopathic medicine and its importance in the preservation of health at household and community level. The central hypothesis of the research states that despite the influence of allopathic medicine in the population, the predominant use and transmission of knowledge across generations, preserving the tradition of using medicinal plants as remedies in primary health care of disease and it is complemented by the conventional system generating a mixed model care in the region.
Materials and methods
The Ejido Lazaro Cardenas (Streams) is located between parallels 20° 24' 42' 'and 20° 25' 28" north latitude, the meridians 96° 57' 53'' longitude and 96° 57' 19' 'form the west meridian of Greenwich and the Ejido Hueytepec 20° 19' 17'' and 20° 19' 48'' north latitude, the meridians 97° 2' 17'' and 97° 1' 6'' west longitude from the meridian of Greenwich. North bordering the Gulf of Mexico, the municipalities of Papantla and Gutiérrez Zamora, Veracruz (Figure 1). The average elevation is 10 meters and 300 meters at its highest point. The vegetation is characterized by grassland, tular, mangrove and tropical semi-deciduous forest, converge in the agricultural, livestock and urban use. Predominantly hot and humid climate with abundant rains in summer, with annual rainfall between 1 400 and 1 600 mm, and the temperature ranges between 24 and 26 °C, corresponding to Aw climate (tropical with summer rains) (INEGI, 2009).

Figure 1 Location of the study area. Source: Prepared with images of Municipal Risk Atlas Tecolutla Basic Level (2011).
The methodological approach of the study was mixed with descriptive correlational and explanatory scope. The non-experimental design with accessible unit test of sampling and volunteer (Hernández, 2010).
The sample size was obtained by the formula
Where: N= total population; n= sample size; d= precision or error. The survey was conducted to 53 family heads of obtaining information on socio-economic aspects of the participants, knowledge and background of the use of medicinal plants, transmission of knowledge and world view of the health-disease process. The study was supplemented with four targeted depth interviews with key informants (two midwives, one at a street vendor last herbalist and the head of the Medical Unit Country Hueytepec), adhering to a semi-structured script, the product of these interviews ordered in order to articulate a narrative in the context of complementarity of knowledge on both sides (family and between traditional medicine and allopathic). Scientific names are specified according to data available on Tropicos.org and the Digital Library of Mexican Traditional Medicine available http://www.medicinatradicionalmexicana.unam.mx.
Results and discussion
Sociodemographic profile of the study population
The average age of respondents was 45 years, with a minimum of 14 and maximum of 76 years. 64.2% were women and 35.8% men. The highest level of education completed was highschool, with an average of 5.3 years of education (incomplete primary). The occupation of the participants were housewives (57.7%), agricultural activities (30.2%), various trades (5.7%), employees (3.8%), students (3.8%); and traders (1.9%).
73.6% is from Riachuelos, 18.9% comes from elsewhere in Veracruz and 7.5% of other State in Mexico. 11.5% spoke an indigenous language, predominantly Totonaco in 71.4% of cases, while 28.6% said they speak Zapotec, an immigrant corresponding sector of other states, mainly of Oaxaca.
Home Remedies and its importance as a strategy for teaching and learning in the family.
98.11% of respondents admit having been taken home remedies based on medicinal plants, mainly for health and for being cheaper than allopathic medicine, also by tradition or taste and eventually out of curiosity. In the process of teaching and learning within the family, 67.3% refers to parents who are best taught the art of home remedies within the family and 32.7% indicated that grandparents. In the nuclear family it is where knowledge is transmitted from parents to children more effectively and practices it, since 84% say they induce their children to consume home remedies often in contrast with 16% prefer not to. This process is reinforced when the grandparents are present.
From the sector that transmit their knowledge to their children, 95.3% provided the remedy and explained to them the components of the mixture and process for preparing them; the rest is limited only to provide them without explanation. While it is obvious that a simple explanation does not enable the user remedies constitute an expert herbalist, but are basic principles to become a guardian of family health. In this process, the woman is the one who has a central role in the preservation and transmission of traditional knowledge, because 100% admitted that are most interested in learning these methods within the family; and especially women in adulthood, for this role in the overall home care, including health of the family, which coincides designated by OMS (1995) and Zapparoli (2012) "... females carry most of the weight in terms of respect for the responsibilities associated with the vital functions of the family, including health".
The main reason for providing home remedies is to improve health by 81.1 % of respondents, and is a complementary practice primary care system that are currently performed by going to the clinic that the State Health System provides. Families turn to the doctor or healer according to the perception of the signs and symptoms of the disease and have their own access to allopathic medicine. This relationship is part of the process of the mixed model of care in which the patient's need to restore their health with the State to guarantee an intercultural context.
The worldview about health and disease. Regarding the disease origin, there is a strong perception that they are linked to changes in consumption patterns between families, linked to the intake of industrialized products. 67.3% related diseases with an unbalanced diet, bad habits by substituting natural foods by processed. Also, in the same proportion they relate to the supernatural elements to which people are exposed, admitting that some people may be caused to other evils mainly due to envy; hence 94.3% agree that one must resort to sorcerers to counter, assuming they know healers to cause illness and diseases, but also know how to remove them.
The economic value and use of medicinal plants. Although, 71.2% indicated not to spent money on buying medicinal plants, 28.8% admit to having spent $117.88 pesos a year on average for this item, with a maximum of $1 200.00 pesos which is very low compared to the expenses incurred in allopathic medicine, $3 896.34 pesos on average and a maximum of $50 000.00 pesos in the case of families with relatives with chronic degenerative diseases. Also admitted selling medicinal plants; however, declare to acquire these therapeutic resources by collecting (20%), buy them at the local market (11%) and 69% grown in the family garden, where some species coexist tolerated and encouraged other protected-plants tolerated arise spontaneously in areas of anthropogenic vegetation that are left there without receiving any handling or care, wild but this strategy is to follow the disturbed areas. The protected arise spontaneously within the field of crops (weeds) or the garden and care recipients directly and consciously made the management to protect the plants. The fostered arise spontaneously within the crop or the garden and indirectly receive some care from the farmer, and management consciously done to encourage growth and development of spontaneous plants, including its dispersion, De Wet et al. (1975), (Figure 2).

In addition to conserve germplasm, preserve traditional management techniques for the maintenance and reproduction of the garden, the species composition and the topological arrangement are defined to make them more functional and productive. Empirically recognize that intra and interspecific competition from vegetable conduct to a more and better synthesize these active ingredients that give them greater therapeutic efficacy. Acosta (2001) states that researching and knowledge of healers, herbalists, is crucial to ensure the supply of medicine to the future trying to find and cultivate high-value medicinal plants that enable rural families to improve their economic situation.
The material evidence is reflected in cutting tools and cleaning the kitchen garden, which demonstrate that many ways in which they interact with plants, these instruments are kept in the corner of the house or in the garden itself, always as testimony to the way in which they are grown, harvested and preserved plants for tea or infusion, treating minor ailments and more aggressive (Figure 2).
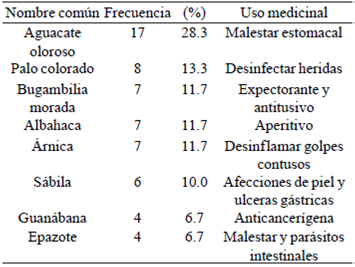
For the primary health care is quite vast the medicinal flora used in the Totonac region. More than 54 species were identified, of which people use as complementary and most often the fragrant avocado (Persea americana Mill.), palo colorado (Hameliapatens Jacq.), the purple bougainvillea (Bougainvillea spectabilis Willd.), basil (Ocimumbasilicum L.), arnica (Heterothecainuloides Cass.), aloe (Aloe barbadensis Mill.), soursop (Annonamuricata L.) and epazote (Teloxysambrosioides (L.) WA Weber) (Table 1).
The 32 diseases mentioned are grouped into thirteen major categories, highlighting those related to digestive, respiratory, metabolic, skin disorders and trauma disorders; headache and toothache, among others (Table 2).

Knowledge as a syncretic act. It is the family space propitious where the parents transmit knowledge, and ancestral wisdom to their children, as manifested by Genaro, who realized that his father was a midwife attending mainly his family: "... my father saw my nieces, my sisters and my mom, because my aunt, the midwife sometimes failed, even with him I learned how to remove the veins of the plant (ribs), how it should be washed well and put them to boil in a large saucepan, exclusively for that and how to filter the mixture; in cases of vaginal inflamed as to how to put to cook with cooking oil acuyo leaves (Piper auritum Kunth) and Santa Maria (Tanacetum parthenium (L.) Sch. Bip.) and how to wrap them in a clean cloth, he studied and also had many books as me "(Huesca, 2013 Pers. Comm.). A similar case is that of Amelia who learned from her mother as much housework as the art of healing, for 40 years makes what she calls giving birth: "... I learned because my mother and my aunt who were midwives took me with them when they went to see sick people..." (Pérez, 2013 Pers. Comm.).
The obvious construction of ordinary dialogue between biomedical and traditional knowledge specializes in them their medical practice and those who interact with these therapists. This kind of learning gather circumstantial actions that are added to them, at least in theory and in this particular case, a complementary relationship coexistence and mutual respect. The testimony of these actors also reflects its relationship with allopathic medicine, as manifested by Genaro when referring that he was invited by a doctor of the Mexican Social Security Institute (IMSS) to work as a cook in his private clinic, but when he demonstrated skills in births, his involvement was even more: "... I worked with her as a cook, and as she attended patients at home she used to tell me, when they get sick, you call me on the phone when they're bad, I would help her and I learnt about giving birth, I also learnt how to put a shot and serum as well... she saw that I liked giving birth and said: you going to help me; with that knowledge I came here to Hueytepec where I started giving birth with all the people here ..." (Jardínes, 2013 Pers. Comm.).
The allopathic doctors, have recognition of the quality and effectiveness of traditional medicine practitioners. The head of the medical field unit (UMC) said: "... the midwives are highly skilled people, have so much intuition and insight to know when a baby will be born, that even scares, they never have infected babies, there rate of infections in children born in hospital than those born with them is higher... " (Huesca, 2013 Pers. Comm.)
Sharing knowledge is also given from allopathic medicine to practitioners of traditional medicine, which is confirmed by the statement made by the doctor on duty in Hueytepec "... four active midwives have just returned from a course taught by the IMSS, where they were trained in the proper use of pine teams, sterilized delivery equipment, especially to prevent cases of congenital tetanus caused by cuts with rusted scissors and contaminated with Clostridium, they received precise information that if they bathe babies using herbs, these must be clean and well boiled, and avoid waste in the navel..." (Pérez, 2013 Pers. Comm.).
The contributions of official medicine is recognized when an interviewee says "... the community was not very clean, we started with the program opportunities with the participation of the community starting to sweep and whitewash, with the arrival of the UMC the issue of health is already communautaire acquis and generally it improved: the chigger, malaria, among others were eradicated" (Jardines, 2013. Pers. comm). Similarly, the medical staff of the clinic accepts the skills of midwives and open channels of dialogue to accept its teachings and ask explicitly to be instructed "... teach me, you know why you practice it and so we both learn" (Pérez, 2013 Pers. Comm.). However, the levels of understanding and language system in each health care has sometimes a few troubles, since the midwives apply what popular wisdom has taught them, as in the following words"... we go with the moons' dates and they do not" (Huesca, 2013 Pers. Comm.).
There is social recognition no matter the gender of the midwife, as expressed by Amelia "... Genaro, my respect for him as well, I recommend him as if he was a doctor, this man is even better than us, if the babe has already been born baby and fifteen or twenty minutes have passed, and the placenta does not come out, he applies an injection and take out the placenta, not even hurting them; I've had a childbirth with him already..." (Pérez, 2013 Pers. Comm.). The above mentioned person do notes: "... when there is no medical authorization to inject the patient, I give make them chew mint leaves (Mentha L.) with salt, which provokes disgust", thus achieving in the mother a violent act as inertia and promptly ends with the expulsion of the placenta.
UMC staff on duty, remain vigilant to ensure that midwives only act in cases of extreme urgency, as long as there is no endanger the life of the mother, this occurs in the framework of the NOM 007SSA2-1993, which is an indicator of management quality on health nationally and internationally to raise the survival rate level. The application of the rule has brought a limitation on the functions of midwives, but there is not also a full understanding of justification. The following quote contextualizes this feelings: "... right now we do not see births, because in a course in Veracruz we were told only to visit each month to watch them go well,... we cannot do anything ourselves. We are several midwives here but we all have said so in the social network or health committee ... that's why we no longer work since 2011, because according to them many women would die; neither me nor my colleagues ever lost a patient, they do have losses in the hospitals and continue working" (Huesca, 2013 Pers. Comm.).
Although this legal provision limits the midwives, they continue practicing for various reasons, such as cultural, economic and capacity of hospitals. In this regard, the UMC chief refers that Genaro disobeyed the indication to not attend births and answered to the call of four births, one of them of high-risk, and says: "... I've had that failure about him, even though he informs to be attending a childbirth and that everything is in order, the medical staff remains alert for any obstetric emergency..." (Jardines, 2013 Pers. Comm.). Amelia also states "... in an emergency will not let the person die, but if it is high-risk and is scheduled, we do not put our hands on it..." (Huesca, 2013 Pers. Comm.).
Another factor of persistence of traditional practice is the close relationship between midwives and patients as they treatment them in their own language and have their confidence, as there is a belief among women that if they go to the clinic, their going to have a surgery to avoid having more children. In the Totonac region, their traditional doctors are midwives, healers and indigenous or half-blood sorcerers, who know of medicinal plants for delivering babies and also for relieving physical and inner illnesses. They are people who acquire a privileged status within their communities and they are respected within the families who come to receive their services. There is a bond established between traditional medicine practitioners and their patients and go beyond the cognitive aspect, an example of this is that the midwives and obstetricians are also called "grandmothers or grandfathers" of new borns, and they correspond them and name them "navel grandchildren"
The loss of traditional knowledge and attitudes that were part of the healing process and that augured good life for the newborn are lost by several causes, that in words of Genaro reflect his feelings "... they used to have a habit of making a party, killing a turkey or a pig and made mole, tamales and gave food to the midwife, now days we don't even get any food at all... also perfuming the babies with incense, lighting twenty-four candles, walking the child in there, I did all that for the child to grow pretty" (Jardines, 2013 Pers. Comm.). Nevertheless, there is no disappointment or frustration for them, only survives the love and respect for them as their "navel grandchildren".
In the field of modern medicine, the practice leads to the medical staffto gain a better understanding ofthe sophistication of local knowledge systems and incorporate them into their own, as the doctor says "... I tell them not to stop taking the drug and drink guaya tea (Melicoccus bijugatus Jacq.) as drinking water, they like it because it is not bitter". Discloses quite satisfied that injured patients sap palo colorado (Hamelia patens Jacq.) and accelerates healing; know of other cases in which ingest muicle (Justicia spicigera Schltdl) increasing the hemoglobin levels...", goes on saying " there are many cases of anaemia associated with poverty, there are campaigns for its detection, but they do not come despite that the children are pale, present rickets, unwillingness and they do not do well in school" (Jardines, 2013 Pers. Comm.). However, regretting that the present education sector in the town is still helpless to join the dialogue on this knowledge, above all by the lack of knowledge and commitment to community health.
The living pharmacy in the courtyard of the UMC of Hueytepeces represents a sign as a symbolic act of the complementarity and mutuality-regime achieved; the doctor exhibits pleased a small plot where midwives grow some plants they use in their ethnomedical practice.
As we can see, this social phenomenon is complex, where the participation of different actors (families, authorities, doctors, healers, patients) form a functional system regarding health care and it is quite important to understand it for the effective implementation of initiatives towards its strengthening and, as mentioned by Mata (2002), not only about production, but also regarding technology, the services, incomes, in all the dimensions for a better life quality. The risk in the development of process, the aggression is not focused only on the environment, it also involves cultural and social aspects that also have a significant impact (Bes, 1997).
The United Nations Industrial Development Organization (UNIDO) reported in 1998 that, without counting with users of medicinal products derived from industrial processes of medicinal plants, it has been calculated that there are about 1500 million people turning to vegetable traditional therapies. Therefore it is urgent to preserve the traditional knowledge and implement its dissemination and preservation in order to contribute to the welfare of social subjects and care of natural resources.
Conclusions
The use of traditional medicine in the Totonac region remains central to the preservation of health at home and in the nuclear family where the parents are primarily concerned with teaching children how to prepare herbal home remedies, considering the production cycles of plants, management intensities and harvesting techniques according to the regenerative capacity of the plant genetic resources available.
The transmission of knowledge prevails and it is consolidated through generations, preserving the tradition of using medicinal plants as remedies in primary care for diseases and is complemented with the conventional system generating a mixed model of attention in the study region. This mixed attention happens spontaneously through an open dialogue between medical field clinic staff, patients, midwives and healers, which facilitates the complex reality that hangs in the practice of traditional medicine that will not be fragmented, achieving to understand the interests, aspirations, needs and goals of individuals that constitute relevant to the transmission of knowledge and conservation and use of natural resources. In this sense, it's quite understood the need to create a Centre for Environmental Education and Traditional Medicine for rescuing ancestral knowledge that promotes and preserves alternative and complementary medicine for improving the health of the rural family.
The farmers and rural communities have suffered a progressive abandonment of development policies to improve the living conditions of the population in these areas, which has led to significant negative impacts on the erosion of their ancestral knowledge in the use and conservation of the environment. In this scenario, medicinal plants have to be a tool to help build new strategies for sustainable rural development.
Literatura consultada
Acosta, L. 2001. Plantas medicinales: una alternativa de desarrollo rural. Facultad de Ciencias Médicas, Cuba. 211 p. [ Links ]
Bañuelos, F. N. 2007. Consideraciones metodológicas para el diseño de propuestas de desarrollo local/regional sustentable en comunidades indígenas. Ra Ximhai. Universidad Autónoma Indígena de México. 3(1):27-47. [ Links ]
Bartoli, P. 2005. ¿Esperando al doctor? Reflexiones sobre una investigación de antropología médica en México. Revista de Antropología Social. 14:71-100. [ Links ]
Bejarano, I. 2004. Lo culto y lo popular. Medicina letrada/Medicina tradicional. Hacia una práctica unificada de los conocimientos médicos. Facultad de humanidades y ciencias sociales. Argentina. Universidad nacional de Jujuy. 24:13-22. [ Links ]
Bes, E. 1997. Aspectos medioambientales en los programas de desarrollo rural. En Revista Española de Desarrollo Rural. Núm. 2. 43 p. [ Links ]
Cuevas, S. J. A. 1991. Definición, aprovechamiento y conservación de recursos fitogenéticos en una comunidad indígena totonaca. Tesis de Maestría. Colegio de Postgraduados en Ciencias Agrícolas, Montecillos, México. 177 p. [ Links ]
Cunningham, A. 2002. Applied ethobotany. People, wild plant use and conservation. Earthscan. WWF/UNESCO. UK. 300 p. [ Links ]
De Wet, J. 1975. Weeds and domesticates: evolution in the manmade habitat. Econ. Bot. 29:99-107. [ Links ]
Duarte, G. 2004. Políticas nacionales de salud y decisiones locales en México: el caso del Hospital Mixto de Cuetzalan, Puebla. Salud Pública, México. 46(5):388-398. [ Links ]
Eroza, S. E. 1996. Tres procedimientos diagnósticos de la medicina tradicional indígena. Alteridades. UAM-Iztapalapa. 6(12):19-26. [ Links ]
Espinosa, C. L. M. 2009. Diálogo de saberes médicos y tradicionales en el contexto de la interculturalidad en salud. Ciencia Ergo Sum. Universidad Autónoma del Estado de México. 16(3):293-301. [ Links ]
Estomba, D. 2006. Medicinal wild plant knowledge and gathering patterns in a Mapuche community of North-western Patagonia. Enthnopharmacol. 103:109-119. [ Links ]
Foucault, M. 1982. El nacimiento de la medicina social. Medicina tradicional. México. 3:3-16. [ Links ]
Gobierno del estado de Veracruz. 2011. Atlas municipal de riesgos nivel básico de Tecolutla. Secretaría de Protección Civil. 38 p. [ Links ]
Hernández, S. R. 2010. Metodología de la investigación. McGraw-Hill. Quinta edición. México. 1-31 pp. [ Links ]
Huesca, A. 2013. Yerbatero ambulante, residente en La Luz del Portugués, Municipio de Gutiérrez Zamora, Veracruz. [ Links ]
Instituto Nacional de Estadística, Geografía e Informática (INEGI). 2009. Prontuario de información geográfica municipal de los Estados Unidos Mexicanos. Tecolutla, Veracruz. Clave geoestadística. 30158. [ Links ]
Jardines, H. A. 2013. Médico encargado de la Unidad Médica de Campo, región III-Norte de Martínez de la Torre, residente en Hueytepec, Municipio de Tecolutla, Veracruz. [ Links ]
Jorand, B. 2008. El conocimiento de la medicina tradicional herbolaria de las comunidades nahuas del Municipio de Hueyapan, en la Sierra Norte de Puebla. Cuicuilco. ENAH. México. 15(44):181-196. [ Links ]
Mata, B. 2002. Desarrollo Rural centrado en la pobreza. Ed. Universidad Autónoma de Chapingo (UACH). México, D. F. 87 p. [ Links ]
Mendoza, G. R. 2011. Uso y manejo de plantas ornamentales y medicinales en espacios urbanos, suburbanos y rurales. Rev. Mex. Cienc. Agríc. 3:525-538. [ Links ]
Pérez, A. 2013. Partera de Hueytepec, residente en Hueytepec, Municipio de Tecolutla, Veracruz. [ Links ]
Prieto, A. M. 2004. Conocimiento indígena tradicional: el verdadero guardián del oro verde. Boletín de antropología. Universidad de Antioquía, Colombia. 18(35):132-164. [ Links ]
Ramos, G. 2013. Partero de Hueytepec, residente en Hueytepec, Municipio de Tecolutla, Veracruz. [ Links ]
Tropicos.org. 2014. Jardín botánico de Missouri. ULR: http://www.tropicos.org/. [ Links ]
Universidad Nacional Autónoma de México (UNAM). 2009. Biblioteca digital de la medicina tradicional mexicana. http://www.medicinatradicionalmexicana.unam.mx/. [ Links ]
Zapparoli, Z. M. 2012. Mujeres y prácticas curativas tradicionales. Reflexiones. Universidad de Costa Rica. 91(2):107-119. [ Links ]
Received: July 2015; Accepted: November 2015
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
