










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.22 no.2 Ciudad de México abr./jun. 2018
Case reports
Fibrolipoma in the mouth
* Master’s Degree in Oral Pathology. State University Feira de Santana. Feira de Santana, Brazil.
§ Dental Undergraduate Student. State University Feira de Santana. Feira de Santana, Brazil.
II Master’s Degree in Public Health. State University Feira de Santana. Feira de Santana, Brazil.
¶ PhD in Oral Pathology. State University Feira de Santana. Feira de Santana, Brazil.
Fibrolipoma is the most frequent histological variation of all lipoma lesions. From a clinical point of view, it is very similar to lipoma, for this reason it is frequently misdiagnosed. It is an asymptomatic lesion of benign behavior, rarely found in the oral cavity. These associated factors contribute to drive the patient to only seek treatment when lesions have reached great dimensions, are ulcerated and/or cause deglutition and mastication difficulties. The aim of the present study was to relate three cases of fibrolipoma in the mouth. All three reviewed cases were of 38-49 year old females, who exhibited a nodular, painless lesion in the region of the oral mucosa, with sizes varying 1-2 cm. In all cases, initial suspected diagnosis was fibroma or lipoma, nevertheless, histopathological analysis revealed they were fibrolipoma. Fibrolipoma are rare lesions in the mouth, exhibiting clinical characteristics which are similar to many lesions, thus it is oftentimes diagnosed as one of these entities. Thus, importance of conducting histopathological studies is stressed so that this condition can be accurately diagnosed.
Key words: Pathology; lipoma; mouth
El fibrolipoma es la más prevalente de las variaciones histológicas del lipoma. Clínicamente, se asemeja mucho al lipoma y por eso muchas veces es subdiagnosticado. Es una lesión de comportamiento benigno, que raras veces se desarrolla en la cavidad oral y que suele ser asintomática. Estos factores asociados contribuyen para que la mayoría de los pacientes sólo busquen tratamiento cuando las lesiones presentan grandes dimensiones, están ulceradas y/o causan dificultades en la masticación y deglución. El objetivo de este estudio es relatar tres casos de fibrolipoma en cavidad oral. Los tres casos relatados son de mujeres, con edades entre 38 y 49 años, que presentaban una lesión nodular, indolora, en región de mucosa yugal y con dimensiones variables entre 1 y 2 cm. En todos los casos las sospechas diagnósticas iniciales fueron de fibroma o lipoma, pero el análisis histopatológico concluyó que se trataban de fibrolipomas. Los fibrolipomas son lesiones raras en la cavidad oral y presentan características clínicas semejantes a diversas lesiones, de modo que suelen ser diagnosticados como una de estas entidades. De este modo, se resalta la importancia de la ejecución del estudio histopatológico, para que se pueda realizar un correcto diagnóstico de esta patología.
Palabras clave: Patología; lipoma; boca
Introduction
Lipoma is a benign neoplasia encompassing 50% of all soft tissue tumors. It is more frequently found at the nape of the neck, back, abdomen, buttocks, arms and legs. It is found in head and neck region in 20% of all cases, and in even lesser numbers in the mouth, with frequency of 1-5% of total cases.1-4 According to the World Health Organization (WHO) fibrolipoma constitutes the most prevalent variation of the 13 histological lipoma classifications.5 It is characterized by presence of a significant fibrous component associated to adipose cells lobes.6
Fibroma is a benign tumor commonly found in the trunk of the body as well as the limbs, nevertheless, its onset in the mouth is considered rare.7,8 Clinically, they exhibit similar characteristics to lipoma, since they appear as slow-growing, nodules, ovoidor circularshaped submucosal nodules, which are usually painless and not bleeding.
Due to the benign behavior of these lesions, patients commonly seek treatment only when the lesion is of a great size and/or painful, especially during mastication.6,9 Bearing in mind their clinical similarities with lipoma, histopathological examination is an essential stage in the diagnosis of this type of tumor.8
From a clinical perspective, many differential diagnoses can be proposed, since its clinical pattern frequently appears in other lesions such as lipoma, neurofibroma, fibrous hyperplasia and pleomorphic adenoma.9
Fibrolipoma treatment is exclusively of a surgical nature; the traditional technique is the most common, although diode laser can be used to perform this surgical excision.2,8
This type of lesion exhibits a favorable prognosis and minimum percentage of relapses. Meanwhile, in cases when it does occur, it is directly related to security margins observed during lesion removal surgical procedure.9,10
Case description
Case 1: A 49 year old female, domestic employee, attended the oral lesions reference center due to an asymptomatic nodule in the mouth. Upon review of medical history, the patient informed of blood hypertension, episodes of shortness of breath, persistent cough and drug allergies. The patient had a five-year smoking habit (5 cigarettes a day) and had been consuming alcohol for the last 30 years. She had been wearing full dentures in both arches for the last three years, with no previous history of trauma but with difficulties in chewing. Intra-oral exploration revealed a node-type lesion, with pedicled implantation, of a pinkish hue and superficially located in the oral mucosa adjacent to the region of lower right molars. The lesion was slow-growing for the last four years, exhibiting regular contour, fibrous consistency and approximately 1 cm in its larger extension. Fibroma was the initial diagnostic assumption.
Case 2: A 47 year old female patient, a housewife, attended the reference center due to the presence of a lump in her cheek. The patient informed that the lesion had its onset due to her habit of chewing on her cheek, and that she needed to remove the lump for esthetic reasons. Personal medical history was non-contributory. The patient reported she experienced difficulties when swallowing and chewing. She did not smoke or drink alcohol, and to that moment did not wear dentures. Intraoral exploration revealed a ovoid, regularly contoured, painless nodule, of approximately 2 cm, superficially located in the left oral mucosa region. The lesion was of a soft consistency, pinkish hue, smooth surface, exophytic growth, pedicled implantation and slow growth, spanning 30 years. Initial diagnosis assumption was fibroma with differential diagnosis of lipoma (Figure 1).

Case 3: A 38 year old female, washerwoman, was referred to the oral lesions center to remove a lump she suffered in the mouth. Personal medical history reported dipyrone allergy. The patient did not smoke or drink alcohol and was not wearing dentures. Intraoral examination revealed a painless, node-type, oval shaped and regularly contoured lesion, lesion measured approximately 1 cm, was superficially located in the left lip commissure region, of a soft consistency, pinkish hue intermingled with dark regions, rough surface, exophytic growth, sessile implantation and slow development (two and a half years). First diagnostic assumption was traumatic fibroma with differential diagnoses of inflammatory hyperplasia and lipoma.
Due to the benign character of the cases diagnostic assumptions, selected treatment was surgical excision. Analyses were previously requested (full blood count, bleeding time, prothrombin time, activated partial thromboplastin time and glucose on an empty stomach); they revealed no alterations; therefore, surgical procedures were conducted and samples were preserved in 10% formaldehyde in order to be sent for histopathological analysis to confirm suspected diagnosis (Figure 2).

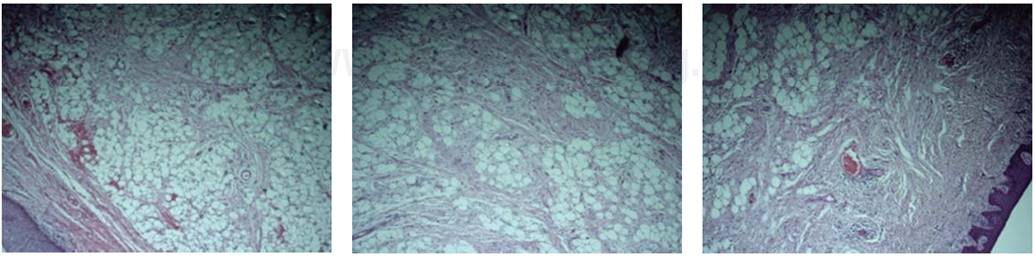
Histological sections of all cases were examined and stained with hematoxylin and eosin. In them, the following was found: benign neoplasia fragments of mesenchymal nature characterized by proliferation of mature adipose cells and fusiform fibroblasts. This proliferation was organized in lobes intermingled with prominent fibrous component. Stroma was of the fibrous dense type, with intense fibroblastic proliferation and collagen deposits, in addition to exhibiting intense vascularization. The following was also observed: moderate chronic inflammatory infiltrate in juxta-epithelial and perivascular position as well as areas of hemorrhagic extravasation. Thus, all three lesions were diagnosed as fibrolipoma (Figure 3).
Discussion
Fibrolipoma are benign tumors representing a histological variation of lipoma; they are not prevalent in the oral cavity and maxillofacial region;1-5 their etiology is as yet unknown, nevertheless, some studies relate them to obesity and trauma. These associations were not conclusive, since, even after adopting a low-fat diet, there was no decrease in lesion size.
With respect to trauma, the association is not yet clear, since it does not occur in all cases.6-9 The same observation were made in the present study, since out of the three studied cases, only one (case 2) experienced previous trauma history.
According to Scivetti et al, 2006, true determination of lipoma incidence is difficult, since these are asymptomatic, slow-growth lesions, so that patients only seek treatment when lesions have reached dimensions to compromise mastication, deglutition and phonation.2,10 Fortunately, even though they were asymptomatic, lesions of cases reported in the present study did not reach a great size, nevertheless, in two cases patients reported difficulties to chew and swallow.
This condition does not exhibit gender predilection, although some studies show a slight superiority in males, especially in the case of very large lesions.7,11 This condition mainly affects subjects aged 40 years and over, but can be found in subjects of any age.1,2,6 In general, fibrolipoma measure between 0.5 and 8 cm diameter,11 the most common size is 1 x 1 x 1 cm.10,12 Cases related to age range and lesion size presented in this study concur with data found in scientific literature, nevertheless, they differ with respect to gender, since all cases here presented were of female patients.
Although they rarely occur in the mouth, these lesions frequently develop in the oral/buccal mucosa, as we could observe in all three cases. In addition to the oral mucosa, they can commonly appear in regions such as the floor of the mouth, tongue and lips.2,7,10,13 Lesions normally appear with nodular aspect, oval shape, soft consistency or slightly indurated; they are floating, of sessile or pedunculated/pediculated implantation and smooth surface. Coloring varies from yellow, when the lining mucosa is thinner, to pinkish hue similar to that of the adjacent mucosa. In cases when the mucosa is thicker.2,10,12,14,15 Thus, most characteristics observed in reviewed cases concur with consulted literature, with exception of rough surface and presence of dark areas in case 3, which was justified by a greater melanin pigmentation in the affected area, since the patient was melanodermic.
Due to their similarities to other conditions, fibrolipoma exhibit many differential diagnoses such as ranula, dermoid cyst, thyroglossal duct cyst, pleomorphic adenoma, pyogenic granuloma, lymphangioma, schwannoma, minor salivary gland neoplasia, fibroma and lipoma.10,15-20 In many cases, even in the cases here presented, it is not possible to establish an accurate fibrolipoma diagnosis based only on clinical data. It is thus essential to conduct complementary examinations such as biopsies (incisional or excisional biopsies depending on the size of the lesion) followed by histopathological analyses.4,6,21,22
From the histological point of view, lesions are neoplastic and of a mixed nature, exhibiting an adipose and fibrous component, they are mature in proliferation, supported by a vascularized conjunctive stroma intermingled with tumor lobes. Histopathological aspect exhibited by these lesions was very specific and essential for the diagnostic conclusion of this condition.
Treatment of fibrolipoma mainly consists on classical surgical excision, although diode laser technique can also be used.2,11,16 When the lesion is small, as in the cases presented in this study, excisional biopsy can be used as treatment as well as complementary examination. Fibrolipoma exhibit low recurrence rate especially in cases when the lesion is well-encapsulated and security margins are respected during their removal.1,10,23
Conclusions
Fibrolipoma is a rare neoplasia found in the mouth, of as yet unknown etiology, no gender predilection and variable size. Some lesions can exhibit high growth potential, and might generate difficulties in basic vital functions such as phonation and deglutition. They are generally painless, although in some cases, when ulcers develop, patients suffer great discomfort. Another important characteristic is that fibrolipoma clinical characteristics are very similar to several other conditions. These similarities, especially with lipoma and fibroma, can result in an under-diagnosis of fibrolipoma. Thus, the need for a histopathological study is stressed, so as to achieve accurate and precise diagnosis of this condition.
Referencias
1. Chidzonga MM, Mahomva L, Marimo C. Gigantic tongue lipoma: a case report. Med Oral Patol Oral Cir Bucal. 2006; 11 (5): E437-E439. [ Links ]
2. Manjunatha BS, Pateel GS, Shah V. Oral fibrolipoma-a rare histological entity: report of 3 cases and review of literature. J Dent (Tehran). 2010; 7 (4): 226-231. [ Links ]
3. Odoi AT, Owusu-Bempah A, Dassah ET, Darkey DE, Quayson SE. Vulvar lipoma: is it so rare? Ghana Med J. 2011; 45 (3): 125-127. [ Links ]
4. Iaconetta G, Friscia M, Cecere A, Romano A, Orabona GD, Califano L. Rare fibrolipoma of the tongue: a case report. J Med Case Rep. 2015; 9: 177. [ Links ]
5. Fletcher CDM, Mertens F, Unni KK. Adipocytic tumors. In: Pathology and genetics: tumors of soft tissue and bone. Lyon, France: World Health Organization Classification of Tumors, IARC Press; 2002. pp. 9-46. [ Links ]
6. Linares SM, Vega ME, Mosqueda A. Lipoma de lengua. Dermatologia Rev Mex. 1996; 40: 414-416. [ Links ]
7. Fregnani ER, Pires FR, Falzoni R, Lopes MA, Vargas PA. Lipomas of the oral cavity: clinical findings, histological classification and proliferative activity of 46 cases. Int J Oral Maxillofac Surg. 2003; 32 (1): 49-53. [ Links ]
8. Do Egito-Vasconcelos BC, Granja-Porto G, De Aguiar Soares-Carneiro SC, Lopes De Freitas-Xavier R. Lipomas of the oral cavity. Rev Bras Otorrinolaringol. 2007; 73 (6): 848. [ Links ]
9. Venkateswarlu M, Geetha P, Srikanth M. A rare case of intraoral lipoma in a six year-old child: a case report. Int J Oral Sci. 2011; 3 (1): 43-46. [ Links ]
10. Scivetti M, Di Cosola M, Lo Muzio L, Pilolli GP, Maiorano E, Capodiferro S et al. Fibrolipoma gigante de la mejilla: a propósito de un caso. Av Odontoestomatol. 2006; 22 (1): 33-36. [ Links ]
11. Furlong MA, Fanburg-Smith JC, Childers EL. Lipoma of the oral and maxillofacial region: Site and subclassification of 125 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98 (4): 441-450. [ Links ]
12. Neville BW, Damm DD, Allen CM, Bouquot JE. Patología oral e maxilofacial. 3a ed. Rio de Janeiro: Saunders Elsevier; 2012. [ Links ]
13. Khubchandani M, Thosar NR, Bahadure RN, Baliga MS, Gaikwad RN. Fibrolipoma of buccal mucosa. Contemp Clin Dent. 2012; 3 (Suppl 1): S112-S114. [ Links ]
14. Bandéca MC, De Pádua JM, Nadalin MR, Ozório JE, Silva-Sousa YT, da Cruz Perez DE. Oral soft tissue lipomas: a case series. J Can Dent Assoc. 2007; 73 (5):431-4. [ Links ]
15. Colella G, Biondi P, Caltabiano R, Vecchio GM, Amico P, Magro G. Giant intramuscular lipoma of the tongue: a case report and literature review. Cases J. 2009; 2: 7906. [ Links ]
16. Del Castillo-Pardo de Vera JL, Cebrián-Carretero JL, Gómez-García E. Chronic lingual ulceration caused by lipoma of the oral cavity. Case report. Med Oral. 2004; 9 (2): 163-167. [ Links ]
17. Favia G, Maiorano E, Orsini G, Piattelli A. Myxoid liposarcoma of the oral cavity with involvement of the periodontal tissues. J Clin Periodontol. 2001; 28 (2): 109-112. [ Links ]
18. Nunes FD, Loducca SV, de Oliveira EM, de Araújo VC. Well-differentiated liposarcoma of the tongue. Oral Oncol. 2002; 38 (1): 117-119. [ Links ]
19. León-Camacho M, Parra-Márquez O, David C, Stea-Tortorice D. Fibrolipoma lingual: reporte de un caso y revisión de literatura. Rev Venez Invets Odont IADR. 2014; 2 (2): 147-155. [ Links ]
20. D’Antonio A, Locatelli G, Liguori G, Addesso M. Pleomorphic lipoma of the tongue as potential mimic of liposarcoma. J Cutan Aesthet Surg. 2013; 6 (1): 51-53. [ Links ]
21. Piattelli A, Rubini C, Fioroni M, Iezzi G. Spindle-cell lipoma of the cheek: a case report. Oral Oncol. 2000; 36 (5): 495-496. [ Links ]
22. Studart-Soares EC, Costa FW, Sousa FB, Alves AP, Osterne RL. Oral lipomas in a Brazilian population: a 10-year study and analysis of 450 cases reported in the literature. Med Oral Patol Oral Cir Bucal. 2010; 15 (5): e691-e696. [ Links ]
23. Moore PL, Goede A, Phillips DE, Carr R. Atypical lipoma of the tongue. J Laryngol Otol. 2001; 115 (10): 859-861. [ Links ]
Received: October 2016; Accepted: September 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
