










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.20 no.1 Ciudad de México ene./mar. 2016
https://doi.org/10.1016/j.rodmex.2016.02.004
Case reports
Teliangectaticum granuloma associated to a natal tooth
a DDS, Specialist in Pediatric Dentistry and Corrective Orthodontics. Teacher at the Rafael Nuñez University Corporation, Cartagena, Colombia.
b DDS, Oral Implantology Specialist. Teacher at the Rafael Nuñez University Corporation, Cartagena, Colombia.
c DDS, Specialist in Stomatology and Oral Surgery, Graduate in Molecular Microbiology. Teacher at the Rafael Nuñez University Corporation, Cartagena, Colombia.
Oral teliangectaticum granuloma, also known as pyogenic granuloma is a proliferation of exuberant granulation tissue caused by chronic inflammation or local irritation. It is a rare lesion in newborn; it appears as an isolated tumor lesion, mostly located in the anterior zone of the alveolar crest. This lesion bleeds spontaneously and shows predilection for the female gender. Its etiology is related to trauma factors, local irritation and hormonal changes. Due to its size it can affect the newborn's feeding. Surgical removal is the choice treatment for this type of lesions. The present study presents the case of a newborn with diagnosis of telangiectaticum granuloma in the mandibular ridge associated to a natal tooth. Clinical and histopathological characteristics are described as well as performed treatment.
Keywords Natal teeth; pyogenic granuloma; breast feeding
Granuloma telangiectásico bucal, también conocido como granuloma piógeno, es una proliferación de tejido de granulación exuberante, a una inflamación crónica o una irritación local, poco frecuente del recién nacido, que se presenta como una lesión tumoral única, localizada con mayor frecuencia en la zona anterior de la cresta alveolar, de sangrado espontáneo, tiene predilección por el género femenino, la etiología se relaciona con factores traumáticos, irritación local y cambios hormonales, por el tamaño puede afectar la alimentación del neonato, la remoción quirúrgica es el tratamiento de elección. Se presenta caso clínico de recién nacido con diagnóstico de granuloma telangiectásico en reborde mandibular asociado a diente natal, se describen las características clínicas, histopatológicas y tratamiento.
Palabras clave Dientes neonatales; granuloma piogénico; lactancia materna; (DeCS)
INTRODUCTION
Oral teliangectaticum granuloma (OTG), also called pyogenic granuloma, or lobular capillary hemangioma, is a reactive, inflammatory, hyperplasic benign lesion which affects skin and oral mucosa. This type of lesion, of unknown pathogenesis, is related in newborn to several developmental factors such as trauma, presence of natal teeth, and local gingival irritation due to plaque, among others.1
This tumor lesion has its onset in the alveolar mucosa. It appears most frequently in the upper jaw, mainly in the anterior region. It is a rapid growing lesion and measures from millimeters to centimeters. It can interfere with the processes of breastfeeding, lip closure and breathing. It can exhibit a reddish hue or be similar to adjoining mucosa; the base of the lesion is frequently pedicled, soft and very prone to bleeding.2
Histo-pathological examination of the lesion reveals endothelium formed by abundant lobes of capillary vessels surrounded by neutrophil-rich inflammatory infiltrate.3 Surgical resection is the most recommended treatment alternative, in order to fully remove the base of the lesion, reach the periostium and extract any natal teeth. Relapse of this lesions is not frequent.4,5
Natal teeth are teeth erupted before their due time. They are present at birth.6 Muench et al reported an OTG case associated to a natal tooth. They proposed that the presence of a natal tooth, or the state of the tissues after its extraction could stimulate the development of OTG due to the trauma received by the gingival tissue when the newborn is breastfeeding.7
Oral examination is an essential part of routine physical examinations, since there are neonatal lesions that could affect the newborn. OTG is an infrequent condition at this stage of life. The aim of the present study project was to acquire knowledge in etiological factors, as well as clinical and histological characteristics so as to be able to correctly diagnose and treat OTG.
CASE PRESENTATION
A four month old male patient was referred from the Pediatric Dentistry Service to the Stomatology and Oral Surgery Service of the Rafael Nuñez University Corporation, due to the presence of a tumoral lesion at the lower jaw's alveolar ridge. The lesion measured approximately 2.0 cm, was soft, with pedicled base, smooth surface, elicited spontaneous bleeding when breastfeeding, and presented a 29 day evolution time (Figure 1). Upon recording personal history, the mother reported that the newborn had experienced extraction of a natal tooth, the child had then been taken to a pediatric dentist, where it was decided to conduct a 30 day clinical control, with the hope that the lesion would resolve. Clinical assessment revealed increase in lesion size. At that time the mother informed that breastfeeding was accompanied by bleeding and the child's crying, all which considerably decreased the frequency of maternal breastfeeding episodes.

Exploration of organs and systems did not exhibit alterations or familial history contributory to the case. The case's clinical impression was oral telangiectaticum granuloma and differential diagnosis of giant cell peripheral granuloma.
At a surgical meeting attended by different specialists (such as stomatology, oral surgery and periodontics) it was decided to surgically remove the lesion. This decision was reached considering that it was a rapid therapeutic alternative, in view of the lesion's interference with maternal breastfeeding, which affected the newborn's nutrition status. Surgical procedure under general anesthesia and sedation was offered, but, upon the mother's refusal, the procedure was conducted under local anesthesia.
The swaddling technique was used in order to control movements during surgical procedure. This technique consists on rolling the blanket around the newborn, like a well-wrapped package. The idea behind this is that the child feels a replication of the security he experienced within the uterus, as well as to avoid that any of the child’ s reflexes might disrupt the surgical act (Figure 2).8

In the present procedure, infiltrative anesthesia was used. An incision at the base of the lesion was executed with scalpel number 15 and number 3 Bard Parker handle; after incision, the whole area was scraped. Extracted specimen measured 1.9 cm in diameter. It was immersed in a 10% formalin jar after which hemostasis was executed. After this, artificial feeding with a cold bottle was recommended in order to enhance vasoconstriction. Pharmacological and analgesic therapy was prescribed.
Anatomical and pathological report of microscopic description revealed a lesion formed by fibrous stroma with neo-formation of prominent endothelium capillary vessels, joined by inflammatory cells of the lymphocyte, polymorphonuclear neutrophils and eosinophils types. The lesion was lined with a hyperkeratotic squamous epithelium (Figure 3), which was compatible with telangiactetic granuloma and negative to malignancy.
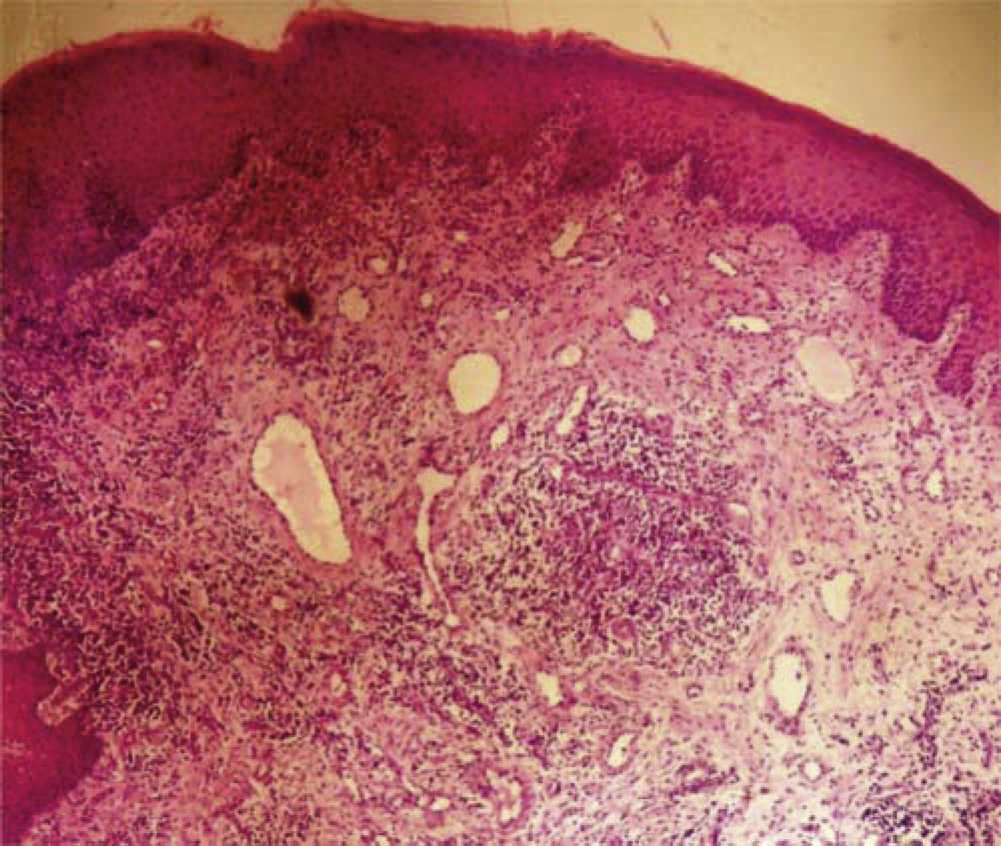
Figure 3 Histological section showing proliferation of small-caliber vessels surrounded by abundant polymorphonuclear neutrophiltype inflammatory cells.
Eight days after procedure, at the post-surgical control, suitable healing of soft tissues was observed (Figure 4). Two months after surgical procedure the patient did not suffer relapse.

DISCUSSION
OTG is considered a benign, vascular, reactive lesion which, when subjected to stimulus, produces excessive growth of connective tissue. It is commonly found in areas of the mouth such as the gingiva, labial mucosa and alveolar ridges. Associated etiologic factors are trauma and local irritation.9,10
Muench et al reported the clinical case of a six day old newborn who presented a tumor lesion at the anterior alveolar ridge of the mandible. The gingival tissue had a mobile natal tooth; the authors concluded that OTG development was due to the presence of that natal tooth.7 This concurs with the present case of a pediatric patient who presented a tumor lesion in the mandibular alveolar ridge with spontaneous bleeding during breastfeeding. This tumor was clinically and histologically compatible with OTG. In the present case, as an important history factor, the mother reported that her child primarily exhibited a mobile natal tooth in the area of the lesion. This could then be considered an etiologic factor associated to the disease due to the friction and the constant trauma it generated in the tissues.
Milano et al reported that OTG could be associated to the presence of natal teeth due to the micro-trauma that the gingival tissue is subjected to when the infant is breastfeeding.4 Garcia et al reported two cases of pediatric patients who presented OTG associated to dental eruption; they reported that micro-trauma suffered by gingival tissue related to an erupting tooth can be associated to OTG development,11 this concurs with the present study of a pediatric patient where the presence of a natal tooth with related OTG factor was due to the trauma teeth could cause on the gingival tissue.
Krishnapillai et al, reviewed 215 OTG cases in a study, the histological characteristics described in that study concurred to those found in the present one.12
With respect to treatment, Willies et al and Muench et al declared that surgical treatment was the most recommended procedure when comparing it to spontaneous regression;1,7 this is in concordance with the present case where surgical resection of the tumor was undertaken. OTG experiences rapid growth, due to its size, it can interfere with the breastfeeding process and thus cause nutritional deficiencies in the newborn. It is recommended that extraction of natal teeth be performed by a dentist or area specialist, so as to avoid inappropriate handling of the soft tissues.
REFERENCES
1. L.J. Willies-Jacobo, H. Isaacs Jr., M.T. Stein. Pyogenic granuloma presenting as a congenital epulis. Arch Pediatr Adolesc Med. 2000, 154: 603-605 [ Links ]
2. C.A. Díaz, P.J. Orozco, A.L. Tirado. Granuloma telangiectásico en cavidad oral. Rev Cubana Estomatol. 2013, 50: 219-225 [ Links ]
3. H. Jafarzadeh, M. Sanatkhani, N. Mohtasham. Oral pyogenic granuloma: a review. J Oral Sci. 2006; 48:167p [ Links ]
4. M. Milano, C.M. Flaitz, J. Bennett. Pyogenic granuloma associated with aberrant tooth development. Tex Dent J. 2001; 118:166p [ Links ]
5. C.M. Rebolledo, R.J. Harris, P.O. Cantillo, M.Z. Carbonell, C.A. Díaz. Granuloma telangiectásico en cavidad oral. Av Odontoestomatol. 2010; 26:249p [ Links ]
6. N.N. Basavanthappa, U. Kagathur, R.N. Basavanthappa, S.T. Surya-prakash. Natal and neonatal teeth: a retrospective study of 15 cases. Eur J Dent. 2011, 5: 168-172 [ Links ]
7. M.G. Muench, S. Layton, J.M. Wright. Pyogenic granuloma associated with a natal tooth: case report. Pediatr Dent. 1992; 14:265p [ Links ]
8. B.E. van Sleuwen, A.C. Engelberts, M.M. Boere-Boonekamp, W. Kuis, T.W. Schulpen, M.P. L’Hoir. Swaddling: a systematic review. Pediatrics. 2007; 120:e1097p [ Links ]
9. A.G. de Souza, B.C. da Silva, M.S. Israel, R. Lindenblatt, A.M. de Andrade, M.E. Ramos. Atypical location of pyogenic granuloma in two pediatric patients. Gen Dent. 2008; 56:447p [ Links ]
10. L. Aguilo. Pyogenic granuloma subsequent to injury of a primary tooth. A case report. Int J Paediatr Dent. 2002; 12:438p [ Links ]
11. C.I. García, A.A. Hinojosa, B.B. Aldape, E.E. Valenzuela. Hemangioma lobular capilar (granuloma piógeno) asociado a la erupción: Reporte de dos casos clínicos. Rev Odont Mex. 2004; 8:127p [ Links ]
12. R. Krishnapillai, K. Punnoose, P.V. Angadi, A. Koneru. Oral pyogenic granuloma--a review of 215 cases in a South Indian Teaching Hospital, Karnataka, over a period of 20 years. Oral Maxillofac Surg. 2012, 16: 305-309 [ Links ]
*This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
Received: June 2015; Accepted: September 2015
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
