










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.20 no.1 Ciudad de México ene./mar. 2016
https://doi.org/10.1016/j.rodmex.2016.02.001
Original research
Temporomandibular joint disorder prevalence in resident physicians at the Specialties Hospital «La Raza» National Medical Center
a Maxillofacial Surgeon attached to Regional Hospital No. 1, Chihuahua, Chihuahua, Mexico.
b Maxillofacial Surgeon, attached to the Maxillofacial Surgery Ser- vice «Dr. Antonio Fraga Mouret», «La Raza» National Medical Center, IMSS.
c Specialist in Applied Statistics. Faculty of Science, UNAM.
Aim:
To determine prevalence of temporomandibular joint disorder in resident physicians at the Specialty Hospital.
Material and methods:
Cross sectioned prospective, observational study. Out of a total of 324, 50 residents were assessed, including non surgical and surgical specialties of different residency years. Residents under orthodontic treatment or having been subjected to previous orthodontic treatment were excluded. Helkimo index was applied for temporomandibular joint diagnostic purposes A physical exploration of the temporomandibular joint and masticatory muscles was later conducted.
Results:
For result evaluation, descriptive statistics and chi-square (χ2) test were used. Statistical package SPSS 12 was used. Prevalence of temporomandibular disorder in residents was 66% of studied population. Significant result was obtained with respect to gender; it being higher in females with p ≤ .013. Greater incidence was observed in the first residency years, as well as in non surgical specialties when compared to surgical ones.
Conclusions:
Prevalence of residents’ temporomandibular disorder was similar to that reported worldwide in general population. The present study equally found greater prevalence in females. It would be significant to conduct another study to measure stress in resident physicians and relationship of stress with temporomandibular disorders.
Keywords Temporomandibular articulation disorder; residents
Objetivos:
Determinar la prevalencia de disfunción de la articulación temporomandibular en médicos residentes del Hospital de Especialidades.
Material y métodos:
Estudio observacional, prospectivo, transversal. Se evaluaron a 50 residentes de un total de 324 incluyendo especialidades no quirúrgicas y quirúrgicas, de los diferentes años de residencia. Fueron excluidos los residentes que se encontraran en tratamiento de ortodoncia o hubieran estado sometidos previamente. Se aplicó el índice de Helkimo con fines diagnósticos para disfunción temporomandibular, posteriormente se realizó una exploración física de la articulación temporomandibular y de los músculos de la masticación.
Resultados:
Para la evaluación de resultados se utilizó estadística descriptiva y chi-cuadrada (χ2). Utilizando el paquete estadístico SPSS 12. La prevalencia de disfunción temporomandibular en residentes fue del 66% de la población estudiada. Tuvimos un resultado significativo en cuanto al género siendo mayor en mujeres con una p ≤ .013. En los primeros años de residencia se observó mayor incidencia, así como en las especialidades no quirúrgicas, que en las quirúrgicas.
Conclusiones:
La prevalencia de la disfunción temporomandibular en residentes es igual a la reportada a nivel mundial en población general. Al igual, encontramos mayor prevalencia en mujeres. Sería importante realizar otro estudio para medir estrés en médicos residentes y la relación con disfunción temporomandibular.
Palabras clave Disfunción de articulación temporomandibular; residentes.
INTRODUCTION
In the general population, a range of 40 to 50% suffer some type of temporomandibular disorder. Initial signs and symptoms usually appear during the second cycle of life. With age, prevalence and symptom implication perception increase.1 A bibliographic review of 17 articles on temporomandibular articulation disorder prevalence, revealed variance of 16 to 68%. Criteria used to diagnose the disorder were Helkimo index in 11.7%, research diagnostic criteria for teemporomandibular disorders 23.5%, craniomandibular index 58.8%, anamnestic questionnaires 35.2%.2
Different research projects confirm the high prevalence of these disorders, reporting that, in adult population, 70-75% suffer at least one sign of temporomandibular disorder,3 one of every four subjects is conscious of suffering it. It has been proposed that, after toothache, temporomandibular articulation disorders are the most common cause for facial pain; they can affect up to 15% of general population. Predominant age ranks between 20 and 40 years of age. Nevertheless, some authors propose that no significant differences are to be found among different age groups. The fact that this disorder is frequent does not imply it warrants treatment in all cases, since in fact, only 5 to 6% really need it. Other affected subjects will suffer mild cases which can even sometimes be transient.
A study was conducted in Mexico in the population of the Military Camp Number 1-A. In it, it was observed that temporomandibular disorder was present in 42% of all cases; in the study results, occlusal alterations were the most important risk factor for patients to suffer temporomandibular disorders.4
Several conditions were found in resident physicians, among those we could count anxiety, depression, hostility and instability.5 Professional wear syndrome or burnout syndrome indicators have been found. This syndrome is very common amongst health professionals, especially in physicians who are exposed to high levels of stress in their work.5,6 Burnout syndrome among different specialties is not statistically significant. I can vary from 75% in gynecologists, 63% in internal medicine physicians, 63% in neurologists, 60% in ophthalmologists, 50% in dermatologists, 40% in general surgeons, 40% in psychiatrists, 27% in family doctors.7,8
Many stress-related diseases can be found in these residents: gastritis 53%, colitis 27%, anxiety 25%, neck muscle contractions 24%, migraine 21%, back pain 17%, alcoholism 17%, unsubstantiated fears 8%, neurodermatitis 3%,asthma 1.5%, frigidigty 1%, impotence 1%, diabetes mellitus II 0.5%, hyperthyroidism 0.09%, hypothyroidism 0.09%.9
Studies have been conducted on whether the residents’ decrease in sleeping hours might bring about important physiopathological consequences such as an increase in pro-inflammatory cytokines, from which a decrease in neurological functions can arise and thus affect cardiovascular health with inflammation of the vascular walls, all of which play an important role in atherosclerosis.9
According to the 2003 Consulate for Accreditation of Medical Education Graduates, there are references on hospital-related activities and the number of residents’ active duty hours. They concluded that these active working hours should not exceed 80 hours per week; it is considered that many residents surpass this number of hours per week; this can be considered a predisposing factor for temporomandibular articulation disorders, since stress is one of its main etiological factors.9,10
MATERIAL AND METHODS
The aim of the present study was to assess prevalence of temporomandibular dysfunction in resident physicians at the Specialties Hospital. It was an observational, prospective, cross-sectioned and open study. To calculate the sample's size, a worldwide prevalence of 50% temporomandibular disorder was arbitrarily taken, with 8% error margin, 95% degree of confidence, in a population of 324 residents of all specialties attached to the Hospital. Result obtained was n = 24. Nevertheless, 50 male and female residents of different specialties were examined, aged 23-40 years, mean 31.5 years. Participants were classified according to year of residency, specialty and whether they presented or not temporomandibular articulation dysfunction. Resident physicians who were not attached to the Institution or who were under orthodontic treatment were excluded.
To conduct the present study, Helkimo index with diagnostic aim for temporomandibular disorders was applied. The index was anonymously answered by resident physicians in training stage, authorization was previously granted with an informed consent letter, based on the format used at IMSS (Mexican Institute of Social Security) for research in human beings. The present research project was conducted at said Institution. This assessment was conducted in two phases: a questionnaire which included questions geared to temporomandibular articulation dysfunction based on symptoms that might be related to that disorder. The second phase was conducted through clinical findings; in it, physical exploration of the following was performed:
1. Temporomandibular articulation exploration: whether there were «clicks» or «crepitations».
2. Masticatory muscles palpation.
3. Mandibular movements limitation (laterality and protrusion).
4. Discrepancy in dental occlusion.
Obtained data were collected in a format designed for this purpose.
Analyses results were examined through central tendency measures, dispersion measures, percentages and chi-square (χ2) test. Special software Microsoft Office Excel® and SPSS12 were used for this procedure.
RESULTS ANALYSIS
The present study was conducted on 50 residents who were randomly selected from a total of 324 physicians attached to the Specialties Hospital. With respect to the gender variable, we studied 26 males (54%) and 24 females (48%). Percentage of temporomandibular dysfunction prevalence in resident physicians of the Specialty Hospital was 66% of total studied population (Figure 1).

Age variable was classified into two groups: in the first group 23-29 year old residents were included: a total of 28 resident physicians formed this group (56%). The second group included 30-37 year old residents, which gave a total of 22 resident physicians (44%) (Figure 2). The residency year variable was equally divided into two groups: the first group included residents in their three first years, which represented 60% of total residents, the second group was composed of residents in their three final years, this represented 40% of the studied population.
In statistical analysis, chi-square (χ2) test with alpha = 0.05 was used to compare the variables; temporomandibular dysfunction with respect to gender revealed that prevalence of temporomandibular dysfunction is significantly different for the gender variable (p = 0.013) (Figure 3).

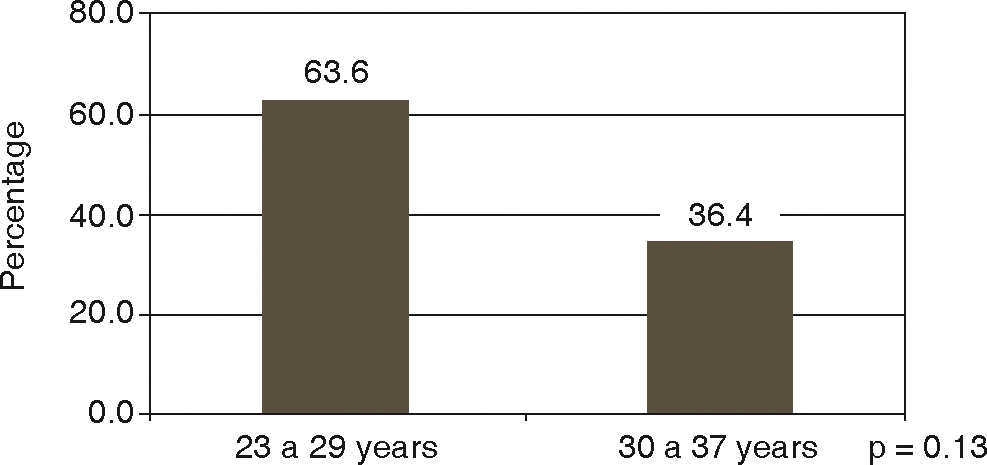
With respect to results of the variable analysis of surgical and non surgical specialties with specialties exhibited greater prevalence index of this disorder, 57.6%, when compared to non surgical specialties which represented 42.4%. Compared with chi-square (χ2) test, results, exhibiting p value = 0.13, were not significant (Figure 4). Relation of age variables and temporomandibular articulation dysfunction revealed greater frequency in subjects aged 23 to 29 years (66%) than in 30-37 year old subjects (36.4%). When conducting statistical analysis with chi-square (χ2) test, a p = .130 value was obtained. This value was not representative.

When measuring temporomandibular articulation dysfunction with respect to with residency years, greater prevalence (63.3%) was observed during the initial years when compared with the final years (42.4%). When conducting chi-square (χ2) analysis, a p = .626 was obtained.
DISCUSSION
When comparing results obtained on prevalence of temporomandibular dysfunction prevalence in resident physicians attached to the Specialties Hospital we obtained of 66% prevalence as related to worldwide evidence of this disorder. In USA and Scandinavian countries it was reported that over 50% of adult population suffered some sign of temporomandibular articulation dysfunction,11,12 systematic review of temporomandibular disorders revealed that this condition exhibited prevalence of 16 to 68%,2 this was similar to prevalence found in resident physicians population. Our study was the first one conducted to assess this disorder in a population of medical residencies, therefore, we did not count with other related studies.
In our study, behavior according to gender was statistically significant: it was more frequent in females p ≤ .013 when compared to studies conducted by Maynassont T, Egmerk I, where no pronounced differences according to gender were reported.3 Nevertheless, Warren, in 200113 reported that these disorders were more frequent in females than in males, and that this could be due to hormonal changes; they thus determined temporomandibular dysfunction prevalence in climacteric women,14 nevertheless, our study encompassed females with a mean age of 31.5 years. Another study in Brazil reported prevalence of temporomandibular dysfunction in females and subjects exposed to high levels of stress.15
Predominant age was 20-40 years, other authors point out that greater incidence of affliction is found at 21-30 years. Nevertheless, some other authors report not having found important differences among different age groups. In our study we found slight significant difference in age, the 23-29 year old group exhibited scarce predominance.
No previous studies were found with respect to relation between years of residency and temporomandibular dysfunction, nevertheless, there have been studies conducted to determine the degree of stress found during the first years of residency.16 Although our study did not measure the degree of stress, it is known that stress contributes to trigger temporomandibular articulation dysfunction. A study conducted by Arenas in 20069 mentions that resident physicians in their second and third year of specialty suffered greater daily stress as well as physiological stress. This was reflected in all at cardiovascular level, digestive tract (80%) such as gastritis and colitis, 65% at psychological level with manifestations of insomnia, anxiety and fear.
When establishing a comparison with our results on prevalence of temporomandibular dysfunction we observed that in subjects in the first three years of residency there was higher incidence of this condition than in subjects in their final years of residency. This can be associated to the fact that temporomandibular dysfunction is related to stress. Garnés Ros17 established that medical or non surgical specialties presented a higher level of stress than surgical specialties, which generally are more technical; nevertheless, differences in results were not significant. In our results on dysfunction of temporomandibular articulation prevalence, it was observed that non surgical specialties exhibited this condition when compared to surgical specialties, this could be related to stress levels. We would like to emphasize that the sole aim of our study was to assess prevalence, we were aware that worldwide, temporomandibular articulation dysfunction was intimately related to stress levels.
CONCLUSIONS
Prevalence of temporomandibular articulation dysfunction in the population of residents of the Specialties Hospital was 66%. This figure is similar to that reported for worldwide general population. We additionally found that, as well as in different studies of this disorder prevalence, females are more affected, this can be due to hormonal changes and to the level of stress they are subjected to.
It could be correlated to the first two years of residency, when subjects are subjected to greater stress and general anxiety, as well as to the relationship that might exist with respect to whether it is a surgical or non surgical specialty, according to the level of stress handled in each of them. Although the present study did not measure stress, we were aware of studies relating stress, anxiety, and temporomandibular dysfunction prevalence. Nevertheless, medical residencies population had not been assessed in previous studies with respect to this disorder which can indeed be limiting. This study established a precedent for further studies where he amount of stress related to temporomandibular articulation dysfunction might be assessed.
REFERENCES
1. J.M. Diabbets, L.T. van der Weele. Prevalence of TMJ symptoms and X-ray findings. Eur J Orthod. 1989, 11: 31-36 [ Links ]
2. M.F. Sena, K.S. Mesquita, F.R. Santos, F.W. Silva, K.V. Serrano. Prevalence of temporomandibular dysfuntion in children and adolescents. Rev Paul Pediatr. 2013, 31: 538-545 [ Links ]
3. T. Magnassont, I. Egermark. A longitudinal epidemiologic study of signs and symptoms of temporomandibular disorders from 15 to 35 years of age. J Orofac Pain.. 2000; 14: [ Links ]
4. J.F. Cano-Pantoja, J.L. Soto-Uribe, L.A. Cruz-Vallejo, M. Guzmán-Gómez. Prevalencia e indicadores de riesgo de la disfunción de la articulación temporomandibular en el personal del Campo Militar No. 1-A. Revista de Sanidad Militar. 1999; 53:198p [ Links ]
5. P.A. Pugno, D.S. McPherson, G.T. Schmittling, N.B. Kahn Jr. Results of the 2002 National Resident Matching Program: family practice. Fam Med. 2002, 34: 584-591 [ Links ]
6. M. Romani, K. Ashkar. Burnout among physicians. Libyan J Med. 2014, 9: 23556-23556 [ Links ]
7. W.W. Ishak, S. Lederer, C. Mandili, R. Nikravesh, L. Seligman, M. Vasa. Burnout during residency training: a literature review. J Grad Med Educ. 2009; 1:236p [ Links ]
8. T.D. Shanafelt, K.A. Bradley, J.E. Wipf, A.L. Back. Burnout and self reported patient care in an internal medicine residency program. Ann Intern Med. 2002, 136: 358-367 [ Links ]
9. O.J. Arenas. Estrés en médicos residentes en una Unidad de Atención Médica de tercer nivel. Cir Gen. 2006; 26:103p [ Links ]
10. H. Zheng, M. Patel, K. Hryniewicz, S.D. Katz. Association of extended work shifts, vascular function, and inflammatory markers in internal medicine residents: a randomized crossover trial. JAMA. 2006, 296: 1049-1050 [ Links ]
11. G. Agerberg, G.E. Carlsson. Functional disorders of the masticatory system: I. Distribution of symptoms by questionnaire. Act Odontol Scand. 1972; 30:597p [ Links ]
12. M.C. Mazengo, P. Kirneskari. Prevalence of craneomandibular disorders in adults of Halv Distric Dar-es Salvom, Tarsania. J Oral Reabil. 1998; 18:569p [ Links ]
13. M.P. Warren, J.L. Fried. Temporomandibular disorders and hormones in women. Cells Tissues Organs. 2001; 169:187p [ Links ]
14. G.E. Pérez, C.E. Aldana, F.M.G. Ruelas, R.R.M. Díaz. Frecuencia de trastornos temporomandibulares en mujeres climatéricas en el Instituto Nacional de Perinatología. Rev ADM. 2005; LXII:85p [ Links ]
15. N. Boscato, R.C. Almeida, C.D. Koller, A.A. Presta, M.L. Goettems. Influence of anxiety on temporomandibular disorders-an epidemiological survey with elders and adults in Southern Brazil. J Oral Rehabil. 2013; 40:643p [ Links ]
16. Accreditation Council for Graduate Medical Education. Common program requirements-duty hour requirements. 2003. Accessed: 4 October 2004. [ Links ]
17. Garnés Ros AF. Desgaste Laboral (Burnout) en Médicos de Urgencias de Hospital. [Tesis] Doctoral Universidad Miguel Hernández; 2001. [ Links ]
*This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
Received: January 2015; Accepted: May 2015
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
