










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista odontológica mexicana
versão impressa ISSN 1870-199X
Rev. Odont. Mex vol.19 no.1 Ciudad de México Jan./Mar. 2015
Original research
Prognosis method for risk assessment of dental caries induced by chocolate comsumption
Julio Fernando Cevallos Zumarán,* Antonio Armando Aguirre Aguilar§
* DDS, Trujillo University Graduate School Graduate.
§ DDS PhD, Professor at Graduate and Stomatology School.
University of Trujillo, Perú.
ABSTRACT
Aim: The aim of the present study was to propose a valuation method of stomatological caries risk due to chocolate consumption, based on DMFT and or S-OHI in 12 to 13 year old adolescents. Material and methods: A longitudinal study was conducted on 150 adolescents, which were divided into 15 groups of ten members each, according to DMFT and S-OHI; members consumed one chocolate tablet. Baseline salivary pH was measured at ingestion time as well as 10 minutes after intake. Results: It was determined that for the group of adolescents with very low DMFT, as well as for all S-OHI levels, baseline pH was 7.30 ± 0.12, and post-intake ph was 7.06 ± 16, p < 0.001. In the group of adolescents with low DMFT as well as for all S-OHI levels, baseline pH was 7.24 ± 0.18, and post-intake pH was 6.98 ± 0.18, p < 0.001. In the group of adolescents with moderate DMFT and for all levels of OHI-S, basal pH was 7.21 ± 0.18 and pH after consumption was 6.96 ± 0.21 p < 0.001. In the group of adolescents with high DMFT and for all levels of OHI-S, basal pH was 7.17 ± 0.15 and pH after consumption was 6.87 ± 0.18 p < 0.001. In the group of adolescents with very high DMFT and for all levels of OHI-S basal pH was 7.01 ± 0.34 and post consumption pH was 6.71 ± 0.34 p < 0.001. Conclusions: 10 minutes after chocolate intake, salivary pH level significantly decreased. This decrease was directly proportional to caries circumstances and oral hygiene levels. Nevertheless, in none of the groups did it reach critical levels for enamel demineralization. It did reach critical levels for dentin demineralization in the group with high DMFT and deficient OHI. Proposal: A prognosis method for assessment of stomatological risk of enamel caries caused by chocolate consumption was proposed. This method was based on DMFT assessment; for caries in dentin, the method used was based on DMFT and S-OHI assessment.
Key words: Saliva, cocoa, concentration of hydrogen ions, DMF index, oral hygiene index.
INTRODUCTION
In the field of dentistry, prevention is one of the main concerns. Within this scope, study of human saliva is an important scientific contribution, since saliva is considered one of the main factors of caries' stomatological risks.1,2
Dr Miller, in 1890, with his chemo-parasitic theory proved that oral bacteriae produced acids when fermenting diet carbohydrates, and that these acids dissolved enamel and caused its deterioration. But it was not until 1960 that Dr. Keyes established the fact that dental caries etiology obeyed a scheme composed by three interacting agents (host, micro-organisms and diet). These three factors were called Keyes triad. In 1978, Dr. Newbrun incorporated the «time» factor to the aforementioned interaction; these four factors are essential for the initiation of a caries lesion. Further on in time, saliva would be considered if not the most important, at least one of the principal agents to be considered for the development of a caries process.3-5
De-mineralization and re-mineralization processes occurring in the tooth's surface are important for the understanding of the mechanism of caries. Hydroxyapatite Ca10(PO4)6(OH)2 is the mineral component of enamel, dentin and cement .When in a neutral medium, hydroxyapatite is in balance with the local aqueous environment, which is saturated with calcium ions Ca2+ or PO4.6
Hydroxyapatite reacts with hydrogen ions at pH 5.5 or lower. Hydrogen ions preferentially react with phosphate groups of the aqueous environment located immediately adjacent to the crystal's surface. We can consider this process as a conversion of PO43- into HPO42-due to the addition of one hydrogen ion. HPO4 can no longer contribute to the normal balance of the hydroxyapatite, since it now contains PO4 instead of HPO4; therefore, the hydroxyapatite crystal is dissolved. This process is known as demineralization.6
Saliva is a complex exocrine secretion which originates from major salivary glands in 93% and minor salivary glands in the remaining 7%, It extends over all oral regions. It is sterile when it first comes from the salivary glands, but ceases to be so the moment it mixes with crevicular fluids, food remnants, micro-organisms and desquamated cells from the oral mucosa.7-11
The protective function of saliva is not limited to tissue lubrication and micro-organism removal; it has been noted that variations in salivary pH as well as its chemical composition can significantly alter the state of oral-dental health.1,7,12
PH of the oral cavity and of bacterial plaque is related to saliva's buffering capacity, which in turn is determined by the presence of buffering systems such as: bicarbonates, phosphates, ammonia and proteins among others. An intimate relationship between saliva's buffering capacity and caries incidence has been noted in patients.12
In 1940, Dr. Stephan showed that between 2 to 5 minutes after rinsing with a glucose or sucrose solution, plaque's pH decreased, only to return to its baseline levels in a 15 to 40 minute span, depending on the saliva characteristics of each subject as well as the type of stimulus.13
Salivary ph is a manner to express in a logarithmic scale, the concentration of hydrogen ions found in the salivary solution, thus determining acid or alkaline characteristics of the saliva. Salivary pH tends to neutrality, with an average value of 6.7, varying between 6.2 and 7.6.12,14
From the dental perspective, pH is critical when it dissolves dental tissues; it varies in different bacterial plaques, mainly depending on phosphate and calcium ion concentration; it is influenced by the neutralizing capacity and ionic strength of the environment. Critical pH is not constant, but it remains proportionate to calcium and phosphate concentrations in the saliva and plaque fluid.6 Even though lacking an exact value, it can be considered that critical ph in enamel surface is found to be between 5.3 and 5.7, and in dentin it ranges from 6.5 to 6.7.6
In 2010, Drs. Yabar E and Aguirre A15 undertook in Peru a study with the aim of determining the effect of the D'Onofrio sublime brand chocolate on the salivary ph of young adults aged 19 to 25 years. Experimental and control groups were formed with 26 young adults (cross over). It was found that 5 minutes after ingesting milk chocolate, salivary pH decreased significantly. When the same group of subjects chewed paraffin, their salivary pH increased significantly 5 minutes after chewing. Baseline pH in both groups did not exhibit significant differences.15
In 2011, Drs. Aguirre A and Vargas S undertook in Peru a study on salivary pH level variations in a group of 12-13 year old adolescents and their relation with S-OHI, in that study moderate DMFT was considered a criterion for sample selection. In the study it was concluded that salivary pH level significantly decreased with chocolate consumption, this decrease was related to the oral hygiene index, without reaching critical levels for enamel demineralization.16
Several authors have determined the fact that salivary pH is considered a risk assessment factor in caries. After observing behavior of different DMFT and IHO levels when ingesting a chocolate bar, we proposed a simple, rapid, clinical prediction method to assess stomatological caries risk due to chocolate consumption. The target was to devise a method that could be followed in all dental offices.
MATERIALS AND METHODS
The present prospective, longitudinal and comparative research project was adjusted to a pretest and post-test design. It was conducted at the Rafael Narvaez Cardenillas College of the National University of Trujillo. Saliva samples were harvested from 150 adolescents. The samples were determined by means of a formula to compare the effect of two study groups for quantitative variable.16
Inclusion criteria were: age ≥ 12 years < 14 years, informed consent and assent, suitable general health circumstances, nose-breathers, full permanent dentition, no orthodontic treatment or removable or fixed prostheses, no consumption of drugs which might have interfered with salivary functions.
Sample harvesting
Through random selection and according to DMFT and S-OHI 15 groups of 10 subjects were formed, (each one included all 5 DMFT levels in the three S-OHI classifications).
Subjects had refrained from ingesting food for two hours before the experiment. They were asked to rinse their mouth with fresh water, so as to remove any foodstuff rests. Two minutes were allowed to elapse so that subjects could adopt a comfortable position in the dental chair, and then assume a 90 degree position. Baseline saliva samples were harvested with the help of a saliva collector glass and funnel, so as to spit into the tube as indicated in the Tomas Self non-stimulated saliva collection method. After this, subjects were given a 30 gram Nestle Sublime chocolate tablet for consumption, and finally 10 minutes later, saliva was once more harvested so as to measure its pH.
Salivary pH recording
Salivary pH was recorded after saliva harvesting with the HANNA HI98128 potentiometer. This device gauged every 10 samples with a manufacturer-prepared substance. Between each sample, the potentiometer's electrode was rinsed with distilled water, and dried with absorbing paper. Salivary pH of each sample was recorded with a HANNA HI98128 potentiometer according to manufacturer's instructions, and respective files were recorded.
Statistical analysis and data interpretation
Data collected into the data recording tags were processed in an automated manner with the support of statistical package SPSS-15. Statistical analysis calculated the pH's standard deviation average, independent and paired groups Student «t» test was used; the difference was considered significant when the probability of error was lesser than 5% (p < 0.05).
RESULTS
The present study assessed salivary pH variations and determined risk caries caused by Sublime chocolate consumption in 12 and 13 year old adolescents.
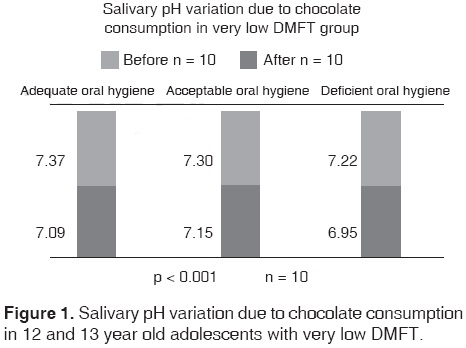
Within the very low DMFT group, subjects with S- OHI presented an average salivary pH of 7.37 ± 0.09 before chocolate consumption; after chocolate consumption it was 7.09 ± 0.13. Established salivary pH variation was thus 0.28 ± 0.15 p < 0.001; subjects with acceptable S-OHI presented average salivary pH of 7.30 ± 0.15 before chocolate consumption and 7.15 ± 0.17 after chocolate consumption. Established salivary pH variation was thus 0.15 ± 0.09 p < 0.001. Subjects with deficient S-OHI presented average of 7.22 ± 0.10 before chocolate consumption and 6.95 ± 0.11 after chocolate consumption, thus, established salivary pH variation was 0.27 ± 0.07 p < 0.001 (Figure 1).
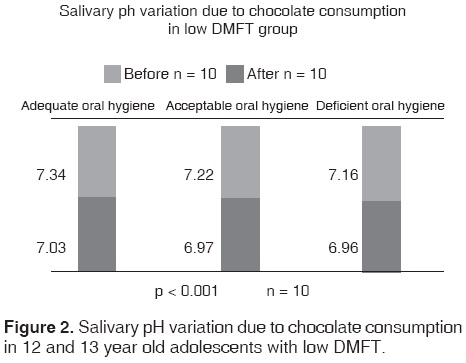
Within the low DMFT group, subjects with suitable S-OHI presented an average salivary ph of 7.34 ± 0.11 before chocolate consumption, and of 7.03 ± 0.18 after chocolate consumption. Established variation of salivary pH was thus 0.32 ± 0.11 p < 0.001. Subjects with acceptable S-OHI presented a slavery pH average of 7.22 ± 0.19 before chocolate consumption and of 6.97 ± 0.18 after chocolate consumption, establishing thus a salivary pH variation of 0.25 ± 0.08 p < 001. Subjects with deficient S-OHI presented average salivary pH of 7.16 ± 0.17 before chocolate consumption and of 6.96 ± 0.18 after chocolate consumption, thus establishing a salivary pH variation of 0.21 ± 0.05 (Figure 2).
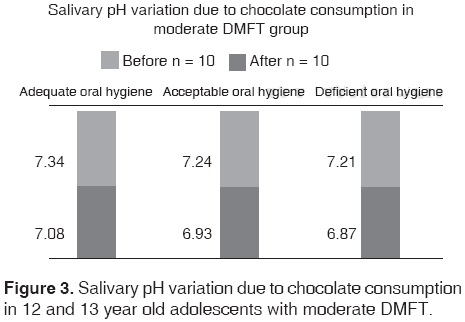
Within the moderate DMFT group, subjects presenting adequate S-OHI presented an average salivary ph of 7.34 ± 0.15 before chocolate consumption, and of 7.08 ± 0.18 after chocolate consumption, establishing thus salivary pH variation of 0.27 ± 0.05 p < 0.001. Subjects with acceptable S-IHO presented salivary pH average of 7.24 ± 0.17 before chocolate consumption and of 6.93 ± 0.23 after chocolate consumption, establishing thus salivary pH variation of 0.31 ± 0.11 p < 0.001. Subjects presenting deficient S-IHO presented average salivary pH of 7.21 + 0.20 before chocolate consumption and of 6.87 ± 0.18 after chocolate consumption, establishing thus a salivary pH variation of 0.34 ± 0.06 p < 0.001 (Figure 3).
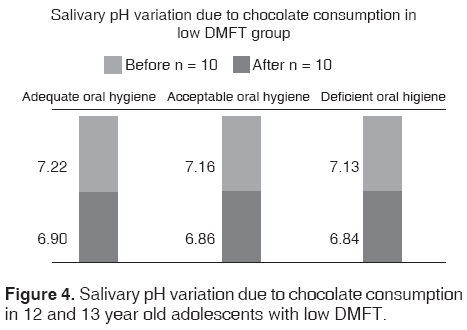
Within the high DMFT group, subjects with adequate S-OHI presented average salivary pH of 7.22 ± 0.10 before chocolate consumption and of 6.90 ± 0.18 after chocolate consumption, establishing thus a salivary pH variation of 0.32 ± 0.10 p < 0.001. Subjects with acceptable S-OHI presented average salivary pH of 7.16 ± 0.17 before chocolate consumption and of 6.86 ± 0.18 after chocolate consumption, establishing thus a salivary pH variation of 0.30 ± 0.04 p < 0.001. Subjects with deficient S-OHI presented average salivary ph of 7.13 ± 0.16 before chocolate ingestion and of 6.84 ± 0.18 after chocolate consumption, establishing thus a salivary ph variation of 0.29 ± 0.07 p < 0.001 (Figure 4).
Within the very high DMFT group, subjects with adequate S-OHI presented average salivary ph of 7.24 ± 0.10 before chocolate consumption, and of 6.94 ± 0.11 after chocolate consumption, establishing thus a salivary ph variation of 0.30 ± 0.06 p < 0001. Subjects with acceptable S-OHI presented average salivary pH of 7.14 ± 0.15 before chocolate consumption and of 6.84 ± 0.17 after chocolate consumption, establishing thus a salivary pH variation of 0.30 ± 0.10 p < 0.001. Subjects presenting deficient S-OHI presented average salivary ph of 6.66 ± 0.35 before chocolate consumption and of 6.34 ± 0.31 after chocolate consumption, establishing thus a salivary pH variation of 0.32 ± 0.06 p < 0.001 (Figure 5).

DISCUSSION
Studies conducted up to the present support congruent statistically significant value variation with the principle or Stephan's Curve, which revealsexistence of rapid plaque pH decrease after exposition to a sugared solution, chocolate in this case. Nevertheless these studies equally warn about the fact that this variation is insufficient to initiate demineralization processes in enamel or dentin.15,16
We greatly value this knowledge, but we must also bear in mind that studies have been conducted on subjects presenting moderate caries experience, with the aim of establishing a generalization of the effect of chocolate consumption on hard structures of the tooth.
Therefore, when assessing the group of adolescents exhibiting very low DMFT, at different levels of oral hygiene, even though establishing highly significant pH statistical variation in all three groups, we must bear in mind that this variation does not reach critical levels of demineralization for dentin or enamel, since values established as critical are 5.3 to 5.7 for enamel and 6.5 to 6.7 for dentin (Figure 1).
This same situation was present with adolescents exhibiting low, moderate and high DMFT, with different oral hygiene levels. In these cases, even though a highly significant pH variation was determined, it would not reach critical levels of demineralization in dental tissues (Figures 2 to 4 (3)).
The aforementioned studies coincide with reports from Drs. Yabar E and Aguirre A15 derived from a similar study conducted on young university students (19 to 25 years of age). This would enable us to further state that saliva's buffering ability and physiological behavior would not vary from adolescence to adult age.
We equally refer to studies of Drs. Aguirre A and Vargas S,16 when they conducted a similar study with 12 and 13 year old students, who presented moderate DMFT. Data obtained by those doctors are similar to those obtained in the present study.
A highly significant pH variation is equally established in the group of adolescents exhibiting very high DMFT: saliva acidification was 7.2 to 6.9 in adolescents with adequate oral hygiene, 7.1 to 6.8 in adolescents with acceptable oral hygiene and 6.7 to 6.3 in the group of deficient oral hygiene. This last group is considered at risk of dentin demineralization: in these subjects alterations in tooth enamel such as abfractions, erosion, caries, etc. would have exposed dentin to the oral environment and would have initiated a demineralization process after chocolate consumption (Figure 5).
Analysis of obtained results allows us to establish a method for stomatological risk prediction for enamel caries, via the sole assessment of DMFT, and for dentin caries in the high DMFT group by assessment of S-OHI.
CONCLUSIONS
After Sublime brand chocolate consumption, a significant salivary pH variation could be observed, which reached levels considered non-critical for enamel demineralization at all DMFT and S-OHI level, whereas for dentin tissue risk of demineralization was observed in the high DMFT, deficient S-OHI group.
Figure 6 depicts a predictive method for the assessment of stomatological risk for caries caused by chocolate consumption.

REFERENCES
1. Caridad C. El pH, flujo salival y capacidad buffer en relación a la formación de placa dental. ODOUS Científica (Internet). 2008 (consulta el 18 de febrero 2011); 10 (1): 25-32. Disponible en: http://servicio.cid.uc.edu.ve/odontologia/revista/v9n1/art3.pdf. [ Links ]
2. Seif T. Cariología. Venezuela. Edit. Actualidades Odontológicas Latinoamericana, C.A.; 1997. [ Links ]
3. Henostroza G, Henostroza N, Úrzua I. En: Henostroza G y cols. Caries dental: principios y procedimientos para el diagnóstico. Lima: Ripano; 2007, pp. 16-36. [ Links ]
4. Liébana J. Microbiología oral. Editorial Latinoamericana. Madrid. España. 1995. [ Links ]
5. Negroni M. Microbiología estomatológica. Fundamentos y Guía Práctica. Editorial Médica Panamericana. Buenos Aires 1999. [ Links ]
6. McIntyre J. Características y progresión de la caries dental. En: Mount GJ, Hume WR y cols. Conservación y restauración de la estructura dental. 1a ed. Madrid: Harcourt Brace; 1999. pp. 9-17. [ Links ]
7. Liébana UJ, Castillo AS, Placa B. En: Cuenca E, Cuenca SB. Odontología Preventiva y comunitaria. España: Editorial Masson; 2007. [ Links ]
8. Llena C. La saliva en el mantenimiento de la salud oral y cómo ayuda en el diagnóstico de algunas patologías. Med Oral Patol Oral Cir Bucal (Internet). 2006 (consulta el 12 de Abril 2011); 11:449-455. Disponible en: http://www.medicinaoral.com/medoralfree01/v11i5/medoralv11i5p449e.pdf. [ Links ]
9. Loyo K, Balda R, Gonzáles O, Lorena A, Gonzáles M. Actividad cariogénica y su relación con el flujo salival y la capacidad amortiguadora de la saliva. Acta Odontol Venez (Internet). 1999 (consulta 18 de Febrero 2011); 37 (3): 10-17. Disponible en: http://www.actaodontologica.com/ediciones/1999/3/actividad_cariogenica_relación_flujo_salival.asp. [ Links ]
10. Merino S. Relación entre los niveles de flujo salival y estrés en estudiantes de la escuela de estomatología de la Universidad Nacional de Trujillo. (Tesis para obtener el grado de bachiller en Estomatología.) Trujillo: Universidad Nacional de Trujillo; 2005. [ Links ]
11. Infantes E. Nivel de Flujo y pH salival en gestantes y no gestantes de 18-35 años de edad, que acuden al hospital IV Vítor Lazarte Echegaray. Estudio comparativo (tesis de bachiller en estomatología). Trujillo, Universidad Nacional de Trujillo; 2008. [ Links ]
12. Baños F, Aranda R. Placa dentobacteriana. AMD. 2003; 60 (1): 34-36. [ Links ]
13. Stephan R. Intraoral hydrogen ion concentration associated with dental caries activity. J Dent Res. 1944; 23: 257-266. [ Links ]
14. Jenkins GN. Fisiología y bioquímica bucal. Editorial Limusa. México 1993. [ Links ]
15. Yabar E, Aguirre A. Variación de pH salival en jóvenes por consumo de chocolate de leche. Vis Dent. 2011; 14 (1): 729-33. Lima Perú. ISSN 1812-1845. [ Links ]
16. Aguirre A, Vargas S. Variación del pH salival por consumo de chocolate y su relación con el IHO en adolescentes. Oral. 2012; 13 (41): 857-861. México. [ Links ]
Note This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam Mailing address:
Mailing address:
Antonio Armando Aguirre Aguilar
E-mail: clinicaaguirre@hotmail.com

