










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.18 no.1 Ciudad de México ene./mar. 2014
Case report
Rotary instrumentation: usage, separation and effect on postoperative endodontic complications
José Leonardo Jiménez-Ortiz,* Alma Nidia Calderón Porras,§ Benjamín Tello-García,II Héctor Manuel Hernández Navarro¶
* DDS, Master of Science in Endodontics, Head of Research Unit.
§ DDS, Professor, Montemorelos University School of Dentistry.
II DDS, Community Service Coordinator, Montemorelos University School of Dentistry.
¶ DDS, Master of Science in Orthodontics, Dean, Montemorelos University School of Dentistry.
Montemorelos University, Nuevo León, México.
ABSTRACT
Introduction of nickel-titanium instruments in the field of endodontics has made conventional root canal therapy more predictable and efficient. However, despite improvements in file designs and metal alloys, fracture of rotary instruments during endodontic treatment still represents a problematic, unwanted and frustrating complication. File separation often results from incorrect use or overuse of an endodontic instrument. If breakage occurs, patients should be informed about the incident and consideration should be given to whether or not to remove the fragment. This report describes a five year follow-up case of a mandibular molar with two separated endodontic rotary instruments lodged into the mesio-buccal and mesio-lingual canals which did not negatively affect the outcome of root canal treatment.
Key words: Endodontics, rotary instruments, fracture, outcome.
INTRODUCTION
In recent years, in the field of endodontics, the use of rotary nickel-titanium (NiTi) instruments has gained great popularity. NiTi instruments have been developed to simplify and improve the effectiveness of endodontic shaping procedures. Studies have reported the ability of rotary NiTi files to minimize procedural errors such as ledge and transportation, and create well-centered smooth canal preparations.1,2 However, a major concern with the use of rotary NiTi during root canal shaping is file breakage. In most cases file separation often results from incorrect use or overuse of an endodontic instrument.3 Although there is a perception that rotary NiTi instruments might unexpectedly fracture, there is evidence indicating that fractures involve many factors. The most important seems to be the clinician's conscious decision to use instruments for a limited number of times or until defects becomes evident.4 In scientific literature, there are descriptions of a number of treatment protocols for this procedural accident during cleaning and shaping of the root canal system, with varying degrees of success; among them we can count the following: the fractured instrument should be left in the canal and tissues in a coronary location with respect to the object should be treated according to standard endodontic procedures; the object should be bypassed and incorporated into the final root canal filling; surgical techniques for removal the object itself or the entire portion of the root with the object; introduction of instruments and techniques for retrieval within the tooth of the obstructing object.5 However, even in cases where file removal is successful, complications in the removal procedure might result in loss of considerable tooth structure and clinical complications such as root perforation.6,7 Thus it is very important to assess the potential difficulty in removal attempts of instruments' fragments and a possible adverse prognosis effect of this procedural complication. The purpose of this article was to report a five year follow up case of mandibular molar, with two separated endodontic instruments in the mesiobuccal and mesiolingual canal respectively, that did not adversely affect the outcome of root canal treatment.
CASE REPORT
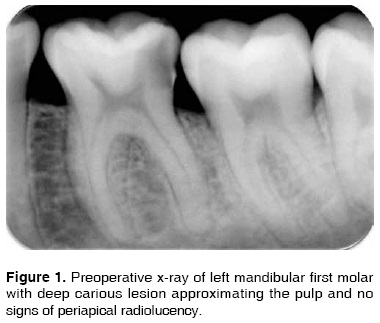
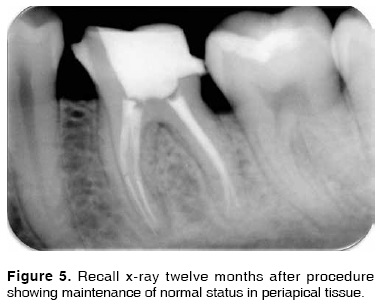
A 25-year-old female patient with a noncontributory medical history was referred to the private office of the main author (JLJO), with the main complaint of a spontaneous toothache in her left mandibular region experienced for three days. History revealed intermittent pain to hot and cold stimuli for the past month. A clinical examination revealed a carious mandibular first molar (tooth 3.6), which was tender to percussion. Palpation of the buccal and lingual aspect of the tooth did not reveal any tenderness. The tooth was not mobile and periodontal probing around the tooth was within physiological limits. Thermal test of the involved tooth with Green Endo Ice (Coltene/Whaledent, USA) caused an intense, lingering pain. A preoperative radiograph revealed distal radiolucency in the area next to the pulp space (Figure 1). Based upon clinical and radiographic findings, a diagnosis of symptomatic irreversible pulpitis and symptomatic apical periodontitis was emitted and endodontic treatment was suggested to the patient. After local anesthesia (1.8 mL Medicaine, articaine-epinephrine, 1:100,000, Septodont, France) and rubber dam isolation, an adequate endodontic access was made. On inspection with 3.0x magnification Surgitel prismatic loupes (General Scientific Corporation, USA), the pulp chamber floor showed four orifices corresponding to four root canals: mesiobuccal(MB), mesiolingual (ML), distobuccal (DB) and distolingual (DL). Negotiation of the root canal system was initially performed with a size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland). The working length (WL) of each canal was established with the Root ZX apex locator (J. Morita Inc, USA) and confirmed radiographically. All four canals were instrumented with ProTaper Universal NiTi rotary instruments (Dentsply Maillefer, Ballaigues, Switzerland) according to the manufacturer's instructions as follows: SX file was used to one half of the WL; S1 file was used up to 4 mm short of the apex; S1 and S2 files were used to the full WL; and F1, F2 and F3 files were used to the full WL. While cleaning and shaping of mesiobuccal and mesiolingual canals with rotary instruments, finishing files F1 and F2 fractured respectively (Figure 2). This was confirmed with a radiograph which showed the two broken instrument tips extending from the apical third to the middle of the canals (Figure 3). The patient was informed about the instrument separation, after this, the treatment option of removal of the fragment was conducted, but it was not possible to retrieve or bypass the broken ProTaper files. Then, under copious irrigation of 5% sodium hypochlorite, 17% EDTA (Vista Dental Products, USA) and a final irrigation with sterile saline, the canal located in a coronary position with respect to the object was treated according to standard endodontic procedures. Cleaning and shaping of the other two canals were completed without incident. After completion of the chemo-mechanical preparation, the canals were dried with sterile paper points, and filled with single cone filling technique, using ProTaper gutta-percha cones (Dentsply Maillefer, Ballaigues, Switzerland) and Sealapex cement (SybronEndo, USA). Access cavity was sealed with Provisit temporary filling (Casa Idea, México) and a postoperative radiograph was taken in order to assess the quality of filling in all canals (Figure 4). The patient did not experience pain or any postoperative complication, and an appropriate crown restoration was performed in a subsequent appointment to ensure adequate coronary seal. The follow-up radiograph taken 12 months later showed the maintenance of the normal status of the peri-radicular tissue (Figure 5). The patient was recalled three and five years postoperatively (Figure 6). At the recall appointments, the patient was symptom free and the tooth had been crowned. The patient will be followed yearly to monitor responses surrounding the root.




DISCUSSION
One of the main concerns in endodontic practice while using rotary NiTi instruments is the occurrence of separation. Reasons for file breakage include operator ability, preparation technique, improper use and overuse of the instrument, minute cracks inherent in the new instrument and root canal anatomy.8 When instrument separation occurs, the patient must be informed about the incident and proper documentation should be placed in his/her record for ethical and legal reasons. Although separated instruments in root canals do not always result in an unfavorable prognosis, instrument fractures prevent the removal of vital or non-vital pulp tissue which can lead to inflammation or infection.9 Considerations should be given to whether or not to remove the fragment either surgically or non surgically. Retrieving an instrument fragment in a canal may cause the excessive removal of dentin structure, decrease root strength, and even root perforation.6,7 Moreover, the success rate of removing the separated instruments in root canals mainly depends on the location of fractured segments and the degree of canal curvature.6,10 Alternatively, there is evidence obtained from systematic review and meta-analysis data from specialized practices and well-controlled university clinics5 which indicate that the prognosis for endodontic treatment when a fractured instrument fragment is left within a root canal is not significantly reduced. The prognosis is poorer if periapical lesions are present at the time of treatment, but only to the extent that effective canal disinfection is compromised. An important finding from this clinical case report was the absence of a preoperative periapical lesion, which served as the main prognostic factor for the successful management of such cases. After instruments breakage occurred in the tooth presented in this paper, decision of leaving the fractured instruments in the canals was made on the basis of diagnosis of symptomatic irreversible pulpitis and symptomatic apical periodontitis. Efforts to decrease failure risks were made after the accident, such as cleansing areas located in an area coronary with respect to the object cleaning and shaping according to standard endodontic procedures in order to incorporate it into the final root canal filling under copious irrigation with sodium hypochlorite, and 15% EDTA used for chelation. Nevertheless, avoidance of the problem is the best approach and clinicians should be proactive in instrumentation technique.11 In the present study, the ProTaper Universal System (Dentsply Maillefer, Ballaigues, Switzerland) was used in biomechanical preparation due their properties during root canal cleaning and shaping. These instruments consist of three shaping files (SX, S1, and S2) three finishing files (F1, F2, and F3) and two accessory finishing files (F4 and F5). These rotary NiTi files have been designed with gradually increasing taper over the length of their cutting blades, allowing each instrument to prepare a specific area of the canal. According to the manufacturer, the progressively tapered instrument system design, is supposed to increase the flexibility, and decrease torsional loads, instrument fatigue, and potential breakage.12 A recent cohort clinical study indicated that the incidence of file separation for the ProTaper rotary instruments was 2.4% and that these instruments may be safely reused clinically for at least four times.13 There are also reports in scientific literature suggesting that ProTaper F3 Instruments are highly susceptible to cyclic fatigue failure and should be reused with caution irrespectively of whether they were initially used for shaping straight or curved canals.14 Despite the fact that fracture of rotary NiTi files is a recognized complication in endodontics, the low incidence of these events supports their continued use during root canal instrumentation.15 To date, the best available evidence regarding prognosis of retained fractured instruments is from studies of case series, which offer a low level of evidence. Only two true case-control investigations were identified16,17 conducted 35 years apart, therefore, wide variations in clinical technique could be assumed. Treatment outcomes, however, have not changed significantly during the past several decades.18 Therefore, from a biologic standpoint, meta-analysis of these two studies seems justified. Case-control studies realistically and ethically provide the highest level of evidence possible in such investigations. Finally, as it was suggested in this report, it is necessary to organize appropriate follow-up of the patient in the event of any clinical complication. This allows periodic review and radiographic assessment to anticipate and deal with any potential problems. If deterioration of periapical health is detected, apical surgery or extraction should be considered.19 The follow-up radiographic exam of a case of mandibular molar with two separated endodontic rotary instruments in the mesiobuccal and mesiolingual canal respectively, at one, three and five years in the clinical case reported in this paper, showed the maintenance of the normal circumstances of tissue surrounding the root and a symptom- free patient with a restored tooth that did not adversely affect the outcome of root canal treatment.
CONCLUSION
This case highlights the fact that rotary instrument fractures do not always lead to an unfavorable prognosis. Their removal from root canals should be attempted, but bearing in mind the possibility of either bypassing it or leaving the fractured fragment inside the canal. The decision of the best available treatment options should be made contemplating pulp status, root canal morphology and position of the fractured instrument, type of instrument as well as clinician's skills. The conflict of opinion regarding clinical significance of this procedural complication during endodontic therapy makes it imperative for clinicians to be offered more definite evidence and information bases in order to be able to predict the potential consequences of fractured instruments left in the root canal system.
REFERENCES
1. Bonaccorso A, Cantatore G, Condorelli GG, Schäfer E, Tripi TR. Shaping ability of four nickel-titanium rotary instruments in simulated S-shaped canals. J Endod. 2009; 35 (6): 883-886. [ Links ]
2. Cheung GS, Liu CS. A retrospective study of endodontic treatment outcome between nickel-titanium rotary and stainless steel hand filing techniques. J Endod. 2009; 35 (7): 938-943. [ Links ]
3. Gambarini G. Cyclic fatigue of ProFile rotary instruments after prolonged clinical use. J Endod. 2001; 34 (5): 386-389. [ Links ]
4. Parashos P, Gordon I, Messer HH. Factors influencing defects of rotary nickel-titanium endodontic instruments after clinical use. J Endod. 2004; 30 (10): 722-725. [ Links ]
5. Panitvisai P, Parunnit P, Sathorn C, Messer HH. Impact of a retained instrument on treatment outcome: a systematic review and meta-analysis. J Endod. 2010; 36 (5): 775-780. [ Links ]
6. Souter NJ, Messer HH. Complications associated with fractured file removal using an ultrasonic technique. J Endod. 2005; 31 (6): 450-452. [ Links ]
7. Ward JR, Parashos P, Messer HH. Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: clinical cases. J Endod. 2003; 29 (11): 764-767. [ Links ]
8. Plotino G, Grande NM, Melo MC, Bahia MG, Testarelli L, Gambarini G. Cyclic fatigue of NiTi rotary instruments in a simulated apical abrupt curvature. Int Endod J. 2010; 43 (3): 226-230. [ Links ]
9. Lin LM, Rosenberg PA, Lin J. Do procedural errors cause endodontic treatment failure? J Am Dent Assoc. 2005; 136 (2): 187-193. [ Links ]
10. Rahimi M, Parashos P. A novel technique for the removal of fractured instruments in the apical third of curved root canals. Int Endod J. 2009; 42 (3): 264-270. [ Links ]
11. Di Fiore PM. A dozen ways to prevent nickel-titanium rotary instrument fracture. J Am Dent Assoc. 2007; 138 (2): 196-201. [ Links ]
12. West J. Progressive taper technology: rationale and clinical technique for the new ProTaper universal system. Dent Today. 2006; 25 (12): 64, 66-69. [ Links ]
13. Wolcott S, Wolcott J, Ishley D, Kennedy W, Johnson S, Minnich S et al. Separation incidence of protaper rotary instruments: a large cohort clinical evaluation. J Endod. 2006; 32 (12): 1139-1141. [ Links ]
14. Ounsi HF, Salameh Z, Al-Shalan T, Ferrari M, Grandini S, Pashley DH et al. Effect of clinical use on the cyclic fatigue resistance of ProTaper nickel-titanium rotary instruments. J Endod. 2007; 33 (6): 737-741. [ Links ]
15. Di Fiore PM, Genov KA, Komaroff E, Li Y, Lin L. Nickel-titanium rotary instrument fracture: a clinical practice assessment. Int Endod J. 2006; 39 (9): 700-708. [ Links ]
16. Crump MC, Natkin E. Relationship of broken root canal instruments to endodontic case prognosis: a clinical investigation. J Am Dent Assoc. 1970; 80: 1341-1347. [ Links ]
17. Spili P, Parashos P, Messer HH. The impact of instrument fracture on outcome of endodontic treatment. J Endod. 2005; 31: 845-850. [ Links ]
18. Friedman S. Expected outcomes in the prevention and treatment of apical periodontitis. In: Ørstavik D, Pitt Ford TR, eds. Essential endodontology: prevention and treatment of apical periodontitis. 2nd ed. Oxford: Blackwell Munksgaard Ltd; 2008. pp. 408-469. [ Links ]
19. Madarati AA, Watts DC, Qualtrough AJ. Opinions and attitudes of endodontists and general dental practitioners in the UK towards the intra-canal fracture of endodontic instruments: part 2. Int Endod J. 2008; 41: 1079-1087. [ Links ]
Note This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam Mailing address:
Mailing address:
José Leonardo Jiménez-Ortiz
E-mail: endodoncia@um.edu.mx

