










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista odontológica mexicana
Print version ISSN 1870-199X
Rev. Odont. Mex vol.17 n.4 Ciudad de México Oct./Dec. 2013
Case reports
Periodontal plastic surgery performed in clinically short crowns for prosthetic rehabilitation
Rosalía Martínez Hernández,* Ma. Guadalupe Marín González§
* Periodontist, Undergraduate and Graduate Professor, Research and Graduate School, National School of Dentistry, National University of Mexico (UNAM).
§ Professor, Periodontics Specialty, Graduate and Research School, National School of Dentistry, National University of Mexico (UNAM).
ABSTRACT
In recent years, esthetics has become paramount in dental treatments, raising high expectations in patients. Esthetic harmony is determined by the smile, which in turn is influenced by the position and dimension of teeth, gums and lips. Conditions affecting dental clinical crowns require intervention of several dental disciplines to restore function and esthetics. Lengthening of the surgical crown allows for the increase of supra-crest crown length as well as the re-establishment of biological thickness to balance restorative esthetic requirements with periodontal health. Case presentation: A female patient afflicted with delayed passive eruption was referred from the Prosthetics Department to undergo lengthening of crown to achieve prosthetic rehabilitation. Conclusions: Crown lengthening allows tissue preparation and achieves esthetic and physiological stability, achieving access to prosthetic margins preserving thus suitable prosthetic-periodontal unity.
Key words: Esthetics, biological thickness, crown lengthening, bone surgery.
INTRODUCTION
Currently, esthetics is paramount in all dental procedures, and patients are encouraged to entertain high expectations. It has thus become one of the main goals to attain when performing any treatment. Periodontal surgery can help in some cases to achieve this aim by providing a harmonious smile.1-3
Conditions which might affect esthetic harmony are: papillae loss, confined ridge defects, gingival recession, excessive gingival display, delayed passive eruption, lack of keratinized gingiva, gingival tattoo, unsightly gingival texture and aberrant frenum/muscle position.
Analysis of face and smile must be achieved in order to treat excessive gingival exposition or delayed passive eruption cases. The analysis must encompass height, shape and facial profile of the patient as well as his/her age and gender.
Facial height is divided into three thirds: the upper third is variable according to the hairstyle type of the patient; the middle and lower thirds are more related to oral esthetics. The middle third spans from the glabella (most prominent point between eyebrows) up to sub-nasal point (point underneath the nose). The lower third is measured from the sub-nasal point up to the soft tissue of the chin (which is underneath the chin). When measured in a resting position, the middle third is equal in length to the lower third.
The width of the face is typically the width of ''five eyes''. Looking from a frontal perspective, the four recognized basic facial forms are: square, long, square-long and ovoid. The three facial profiles are straight, concave and convex.4
The line of the smile must be assessed in a diversity of situations: at rest, during speaking and when smiling. During a full smile, the upper lip must rest at the level of medium-facial gingival margins of the upper front teeth. The lower lip must rest at the incisive borders of upper anterior teeth (Figure 1). In a full smile instance, the incisive borders of these teeth must run parallel to the curvature of the lower lip.

In some cases, after conducting oral and facial assessments, when excessive gingival exposition is detected, it might be necessary to determine its etiology. Scientific literature reports3,5,6 this condition as ''gingival smile''. It can be caused by skeletal deformities, vertical excess of upper jaw, short upper lip, insufficient clinical crown length or a combination of any of the aforementioned factors. Delayed passive eruption might also be a causing agent, in these cases, there is failure in the gingival margin location at the cement-enamel junction.
The following factors must be established in order to achieve suitable treatment: length of the clinical crown, length of the anatomical crown, apical-crown width of keratinized gingiva, alveolar crest location, position of teeth, position of frenulum, radiographic assessment and trans-gingival probing.
In order to determine the type of surgery to be performed (Table I) Coslet & al5 classify gingival smile as a function of the relationship established among gums, anatomical crown, cement-enamel junction (CEJ) and alveolar crest. Following these parameters they established the following types:
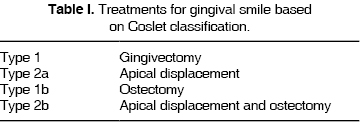
Type 1. The gingival margin is located in a incisive or occlusal position with respect to the cement-enamel junction. The gingival dimension of the gingival margin with respect to the muco-gingival line is acceptable. The muco-gingival line is in an apical position with respect to the alveolar crest.
Type 2. The dimension of the gingival margin to the muco-gingival line is within normal range. The muco-gingival line is at the level of the CEJ.
Sub-group a: CEJ/AC = 1.5 mm. There is normal insertion of gingival fibers to cement.
Sub group b: AC almost to the level of CEJ. Treatment plan is determined according to clinical type.
During surgical procedure, the tooth must be assessed as a biological unit,7 its support conditions must be determined, therefore, the biological width of insertion determines one of the main guidelines within the treatment. Healthy periodontium is a pre-requisite to be able to control gingival tissue response.8,9
The term ''biological width of insertion'' is based upon research conducted by Gargiulo in 1961.10 In that research, he described dimension and relationships in human dento-gingival junction: 0.69 mm ridge depth, 0.97 mm epithelial attachment, 1.07 mm connective tissue insertion, 2.04 mm total biological width. In cases when this space is invaded, an inflammatory process develops which produces gingival recession or insertion loss,8,11-13 depending on the gingival biotype (thick or fine).14 When analyzing the cement-enamel junction (CEJ)15 it must be considered that it is not at the same apical-crown height around the tooth. It is then common to trespass the biological width when placing restorations that do not respect their position.
Consultation with the prosthetics department allows determination of the type of restoration to be achieved,16-18 bearing in mind that the main objective is to preserve dental structure (2 mm) as well as periodontium preservation.19,20 All the following factors must be taken into careful consideration: position of the tooth within the arch, strategic value of the tooth, crown-root ratio before and after surgery, loss of mesio-distal space, aesthetics, endodontic state of the tooth, apical extension of fracture, caries or perforation, level of the alveolar crest, apical extension of previous restorations and space within the arch.8,10,16,21
Once all data has been gathered, diagnosis is emitted and treatment plan is designed. Periodontal surgery,19,20 by way of a crown lengthening process2,5,17,22 provides the opportunity to increase crown length preserving the subject's biological thickness.16,23
Scientific literature reports that prosthetic preparation can be initiated after 6 weeks of healing11, and final restoration must be placed within a span of 3 to 6 months.5,18,22
CLINICAL CASE
49 year old female patient referred by the Prosthetics Department of the Graduate School, National School of Dentistry, National University of Mexico UNAM. Diagnosis emitted was clinically shortened crowns due to bruxism, mal-adjusted restorations in upper centrals, with caries recurrence (Figure 2a). Upon first inspection the following was observed: temporomandibular articulation (TMA) presented crepitation of the right condyle; when performing opening movements, there was deviation to the left side of the lower jaw. There was malpositioning of teeth in the lower arch. The patient complained about having ''short teeth'' and wanted to correct them.

During the interview, the patient informed of both grandmothers being diabetic. She reported observing suitable oral hygiene, brushing three times a day and using dental floss. She informed of no other relevant pathological personal history.
Clinical assessment revealed excessive gingival exposition and clinically shortened crowns in teeth numbers 15, 14, 13, 11, 21, 22, 23, 24 and 25, as well as irregular gingival margin. X rays analysis revealed suitable crown-root ratio (Figure 2b) as well as suitable height of bone crests. Probing did not reveal periodontal pockets, nevertheless, there was bleeding in certain locations. Due to all the aforementioned factors, periodontal diagnosis emitted was localized gingivitis, with delayed passive eruption. Treatment was therefore crown lengthening procedures with tooth bone surgery 15 to 25 (Figure 2c).
Personal Plaque Control (PPC) was conducted. The patient was advised on brushing techniques as well as use of interproximal devices (Super Floss, Oral B®). At a later point, calculi were removed and teeth were polished.
Our Prosthetics Department provided a surgical guide designed on the diagnostic waxing. At a later point, a relaxation occlusal guard was manufactured and adjusted, mal adjusted restorations were removed stumps were re-constructed, and provisional teeth were placed in the whole upper arch. The Orthodontics Department was consulted in order to align lower teeth.
SURGICAL TECHNIQUE
Local anesthesia was administered (2% lidocaine with 1:100,000 epinephrine). Thereafter, trans-gingival probing was conducted to ascertain biological thickness and determine height and position of bone crest. Immediately after this, a periodontal probe was used to measure the vertical length of teeth earmarked for crown lengthening, from second upper left premolar up to upper right second premolar.
Later on, bleeding points were recorded, for this purpose the acetate provided by the Prosthesis Department was used as a guide, from second left upper premolar to second right upper premolar, on its vestibular face, so as to limit and trace the incision zone. For central teeth, the zenith direction was taken into account. The palatal area remained undisturbed.
When the zone was defined, incisions were performed with inner bevel and 15C scalpel blade (Figure 3a) on bleeding points. Incisions were performed from the medial aspect of teeth up to their distal aspect. Papillae located between teeth 11-21 and 21-22 were considered within the incision. Intra-groove incisions were then immediately performed, so as to obtain a band of gingival tissue which was then removed with Gracey's® curettes. Clinical assessment of the new gingival margin level was conducted, so as to establish suitable and harmonious dental dimension which could provide targeted aesthetics. Soft tissues were re-contoured until suitable dimensions were reached.

Once the desired height of the gingival margin was determined, a Hopkins periosteal elevator was used to raise a total thickness flap in order to gain access to the alveolar bone. It was observed that alveolar bone level was not uniform in all teeth.
An ostectomy was performed with rotary system with number three carbide round burr, making sure of not touching the roots and preserving suitable festoon. An osteoplasty was also performed in order to provide positive bone architecture (Figure 3b). At this surgical moment the measure from prosthetic margin to new bone crest was taken so as to obtain a 3 mm distance, preserving thus the biological width of the insertion (Figure 3c). Remaining bone attached to root surfaces was removed with Ochsenbein chisels.
Once a suitable distance was determined which would allow recreation of biological thickness and height of clinical crown to facilitate prosthetic rehabilitation, the flap was sutured with 0000 silk.
Upon completion of suturing process, it was observed that the vestibular frenulum was not well placed and did traction the flap. This situation could endanger the long-term stability of the newly created gingival margin. Therefore, it was decided to perform a frenectomy procedure with scalpel and 15c blade. Upon completion of procedure, 0000 suturing silk was used (Figure 3d). Surgical dressings were not placed.
The patient was instructed to take 10 mg ketocorolate every 8 hours for 3 days, and to rinse with 0.12 % chlorhexidine gluconate every 12 hours for 15 days.
POST-SURGICAL PERIOD
The patient was called 12 days after procedure for suture removal. It was observed that tissues were not swollen and presented suitable clinical conditions; for this reasons the patient was then instructed to initiate plaque control with a soft toothbrush (Sensitive, Oral B®). She was instructed to refrain, for the time being, from using inter-proximal cleansing devices.
15 days later provisional teeth were exchanged for new teeth manufactured with bisacrylic resin. These teeth were then cemented with temporary cement (Temps Bond Kerr®) (Figure 4a).

Six weeks after healing, the prosthetic procedure was reinitiated. Provisional teeth were removed and preparations for total crowns were initiated. At a later point, new provisional teeth were placed which provided better adjustment at the gingival margin (Figure 4b). At this stage, the patient was being orthodontically treated with removable devices in the lower jaw area. Ten months after surgery, final provisional teeth were placed (Figure 4c). At this point the patient presented fixed brackets for orthodontic treatment use.
Final, metal-free restorations were cemented 14 months after healing. At that point, tissues were firm and aesthetic.
RESULTS
During the described lengthening procedure, a gingival margin level was established in concordance with the desired crown length, decreasing thus gingival exposition.
The two central teeth required greater removal of soft tissue; the right lateral did not require modification of gingival margin level, the right canine required a 2 mm margin modification, the rest of teeth subjected to the procedure required soft tissue removal of 1 mm. Elevation of full-thickness flap allowed performance of suitable bone remodeling and .reduction surgery. It provided positive architecture and preserved a 3 mm distance from the bone margin up to the prosthetic preparation.
Suitable clinical characteristics were observed after a six-week healing period.
14 months later, periodontal tissues appeared clinically healthy, with gingival level harmony and proper adaptation of the final prosthesis.
22 months later, the gingival margin had remained stable, preserving suitable periodontal-prosthetic unity (Figure 5).

The described surgical procedure allowed placement of an esthetic and functional restoration. The smile was improved and the patient expressed satisfaction of the result (Figure 6).

DISCUSSION
Pontoriero and Carnevale8 studied during 12 months 84 teeth in 32 patients. Patients were re-examined at 30, 90, 180, 270 and 360 days. Upon examination gingival margin overgrowth was encountered. The authors determined that these findings could suggest presence of a tendency in the periodontium to reform a new physiological supra-crest gingival unity. Overgrowth of soft tissue began almost after one month from the moment when the crest height was defined during surgery. Factors which influenced the amount of coronary displacement of the marginal periodontal tissue seemed to be related to the gingival biotype, the thick type experienced the greater movement, as well as individual healing response. They mentioned the fact that several authors, when determining the amount of tissue to be removed, have suggested using a 3 mm (Ingber 1977), 2.5 to 3.5 mm (Palomo 1978) and 4 mm (Rosenberg 1980) periodontal support surgical removal.
Lanning & al11performed crown lengthening procedures in 23 patients, and assessed results at 3 and 6 months of healing time. They reached the conclusion that biological thickness in treated locations were re-established to their original vertical dimension after 6 months. Therefore, they could affirm that no statistically significant variation of the gingival margin height was found, a constant 3 mm gain in crown structure could be observed after 3 and 6 months.
Coslet & al5 suggested use of a classification in order to establish suitable clinical diagnosis, which would enable determination of treatment plan for patients presenting excessive gingival exposition or delayed passive eruption. This classification would take as a parameter the position of the bone crest and the gingival margin with respect to the cement-enamel junction.
Herrero & al21 conducted research where 12 students of different academic levels intervened. The research aimed at performing crown lengthening procedures to 21 teeth in 16 patients. The study revealed the fact that more experienced periodontists achieved better results. Effectiveness in treatment with respect to greater experience has been shown in other clinical studies, therefore, surgeons must be more aggressive in their surgical procedures, and must take measures, while operating, to provide optimal distance for a healthy gingival unit around the restored tooth.
Dea & al24 studied 43 teeth in 25 patients subjected to surgical crown lengthening, after a 6 month healing period. Re-assessments were conducted at 1, 3 and 6 months. Results at 6 months revealed the fact that tissue over-growth reduced crown height when compared to the initially determined during surgery. This seemed to be related to the height to which the flap was sutured, to the subjects' individual healing characteristics, to the reformation of biological width, to a suitable positive bone architecture during surgery, to regulation of restorative processes and to the individual post-surgical plaque control.
Brägger & al25 assessed 85 teeth in 25 patients after a 6 months healing period. They found minimal changes at the level of the marginal gingival tissue, which had been assessed before surgery, and after 6 weeks and 6 months. He considered that the position in which the flap was sutured determined long term position.
The crown-lengthening procedure presented in this study achieved suitable long term clinical results because diagnosis of excessive gingival exposition was properly performed, since it considered gingival margin position and bone crest with respect to the cement-enamel junction. Bone surgery was performed within proper dimensions, preserving biological thickness.
Surgical procedure allowed total rehabilitation for the patients who exhibited satisfactory esthetic results.
CONCLUSIONS
The possibility of working with other dental disciplines allows the establishment of proper diagnosis and treatment plan, aiming at common goals established by patient expectations as well as involved dental areas.
When initiating any treatment it is necessary to assess the periodontal circumstances of the patient since placement of any restoration which might invade biological thickness will lead to loss of insertion in cases when the gingival biotype is thick; if gingival biotype is thin recession will occur.
Surgical crown-lengthening procedures reduce gingival exposition and allow tissue preparation for later rehabilitation. Physiological and esthetic stability are achieved, access to prosthetic margins is gained, and suitable periodontal-prosthetic unity is accomplished.
REFERENCES
1. Studer S, Zellweger U, Schärer P. The aesthetic guidelines of the mucogingival complex for fixed prosthodontics. Pract Periodontics Aesthet Dent . 1996; 8 (4): 333-41 quiz 342. [ Links ]
2. Jorgensen MG, Nowzari H. Aesthetic crown lengthening. Periodontology 2000 . 2001; 27: 45-58. [ Links ]
3. Reedy MS. Achieving gingival esthetics. A Am Dent Assoc . 2003; 134 (3): 295-304. [ Links ]
4. Davis NC. Smile design. Dent Clin North Am . 2007; 51 (2): 299-318. [ Links ]
5. Levine RA, Mc Wire M. The diagnosis and treatment of the gummy smile. Compendium 1997; 18 (8): 757-766. [ Links ]
6. Konikoff BM, Jhonson DC, Schenkein HA. Clinical crown length of the maxillary anterior teeth preorthodontics and postorthodontics. J Periodontol . 2007; 78: 645-653. [ Links ]
7. Lee EA. Aesthetic crown lengthenig: classification, biologic rationale, and treatment planning considerations. Pract Proced Aesthet Dent . 2004; 16 (10): 769-778. [ Links ]
8. Pontoriero R, Carnevale G. Surgical crown lenghtening: a 12-month clinical wound healing study. J Periodontol . 2001; 72: 841-848. [ Links ]
9. Claman L, Alfaro MA, Mercado A. An interdisciplinaty approach for improved esthetic results in the anterior maxilla. J Prosthet Dent . 2003; 89: 1-5. [ Links ]
10. Padbury Jr A, Eber R, Wang H-L. Interactions between the gingival and the margin of restorations. J Clin Periodontol . 2003; 30: 379-385. [ Links ]
11. Lanning SK, Waldrop TC, Gunsolley JC, Maynard JG. Surgical crown lengthening: evaluation of the biological width. J Periodontol . 2003; 74: 468-474. [ Links ]
12. Yamamoto T, Kinoshita Y, Tsuneishi H, Umemura O, Watanabe T. Estimation of the remaining periodontal ligament from attachment-level measurements. J Clin Periodontol . 2006; 33 (3): 221-225. [ Links ]
13. Broadbent JM, Williams KB, Thompson WM, Williams SM. Dental restorations: a risk factor for periodontal attachment loss? J Clin Periodontol . 2006; 33: 803-810. [ Links ]
14. Sanavi F, Weisgold AS, Rose LF. Biologic width and its relation to periodontal biotypes. J Esthetic Dent . 1998; 10 (3): 157-163. [ Links ]
15. Olson M, Lindhe J. Periodontal characteristics in individuals with varying form of the upper central incisors. J Clin Periodontol . 1991; 18: 78-82. [ Links ]
16. Davarpanah M, Jansen CE, Vidjak FM, Etienne D, Kevir M, Martínez H. Restorative and periodontal considerations of short clinical crowns. Int J Periodont Rest Dent . 1998; 18: 425-433. [ Links ]
17. De Paoli S, Nevins M, Cappetta EG. The biologic width: crown lengthening. Carranza clinical periodontology. Cap. 21 pp 319-328, 10a. ed. Newman, Takei, Klokkewuld, Carranza. Ed. Elsevier Sounds, 2006. [ Links ]
18. Smukler H, Chaibi M. Periodontal and dental considerations in clinical crown extension: a rational basis of treatment. Int J Periodont Rest Dent . 1997; 17: 465-477. [ Links ]
19. Towensed ChL. Resective surgery: an esthetic application . Quintessence Int. 1993; 24: 535-542. [ Links ]
20. Towensed Cerryl Prerestorative Periodontal Plastic Surgery. Creating the Gingival Framework for the Ideal Smile . Dentistry Today. 2004; 130-133. [ Links ]
21. Herrero JB, Scott PS, Maropis RA, Yukna. Clinical comparison of desired versus actual amount of surgical crown lengthening. J Periodontol . 1995; 66: 568-571. [ Links ]
22. Takei, Bevilacqua, Cooney. Surgical crown lengthening of the maxillary anterior dentition: aesthetic considerations. Pract Periodont Aesthet Dent . 1999; 11 (5): 639-644. [ Links ]
23. Kokich VG, Nappen DL, Shapiro PA. Gingival contour and clinical crown length: their effect on the esthetic appearance of maxillary anterior teeth. American J Orthodontics . 1984; 86 (2): 89-94. [ Links ]
24. Deas DE, Moritz AJ, McDonnell HT, Powell ChA, Mealey BL. Osseous surgery for crown lengthening: a 6-month clinical study. J Periodontol . 2004; 75 (9): 1288-1294. [ Links ]
25. Brägger U, Lauchenauer D, Lang NP. Surgical lengthening of the clinical crown. J Clin Periodotol . 1992; 19: 58-63. [ Links ]
Note This article can be read in its full version in the following page http://www.medigraphic.com/facultadodontologiaunam Mailing address:
Mailing address:
CDEP. Rosalía Martínez Hernández
E-mail: cdep.mh8239@gmail.com

