










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista odontológica mexicana
Print version ISSN 1870-199X
Rev. Odont. Mex vol.15 n.4 Ciudad de México Oct./Dec. 2011
Case report
Ovoid pontic design through gingival contour. Report of two cases
Reyes Moreno G,* Rios Szalay E§
* Graduate, Oral Prosthesis Specialty, Graduate School and Research Division, National School of Dentistry, National University of Mexico.
§ Professor, Oral Prostheses Department, Graduate School and Research Division, National School of Dentistry, National University of Mexico.
Received: 3 November 2005.
Accepted: 9 April 2010.
ABSTRACT
Collapse in the anterior maxillary region is one of the most frequently found problems in patients who have endured extractions, especially in zones which represent a great aesthetical challenge. Treatment is often administered lacking proper case planning, and therefore might originate very important defects in the alveolar process periodontal architecture. There are periodontal and prosthetic techniques which can solve this type of situations. The use of ovoid pontics combined with periodontal plastic surgery techniques is mainly administered to patient rehabilitation, and can achieve satisfactory functional and aesthetic results. The purpose of this study was to show two clinical cases where both techniques were used. In the first clinical case, a fixed partial prosthesis of three ceramic units In-Ceram ® devoid of metal was manufactured, using the ovoid pontic technique. In the second case, a Maryland type prosthesis of optimized ceramic polymer reinforced with fiber glass was fabricated. The prosthesis contained an ovoid pontic combined with a subepithelial connective tissue graft to reconstruct the periodontal architecture of the alveolar process in the zone of the missing tooth. Results thus achieved give a natural, aesthetic and functional appearance to the prosthesis pontics.
Key words: Ovoid pontic, plastic periodontal surgery, aesthetics.
INTRODUCTION
Prosthetists frequently face the complex challenge of substituting teeth in edentulous areas, where the pontic shape must fulfil functional, periodontal and aesthetic requirements. Treatments carried out with no proper former case planning cause important defects in the periodontal architecture of the alveolar process, as mentioned by Herbert1,2 and Seibert,3 who provide a classification of these defects. There are many shapes of pontics to choose from, the right selection for each case will have significant bearing on a better prognosis and final result of the treatment. Pontics have been classified4,5 and can be selected according to the particular case. The classification is as follows:
1. Saddle ridge lap
2. Modified saddle ridge lap
3. Flute peak
4. Bullet point
5. Hygienic
6. Ovoid
Dewey6 first described ovoid pontics in 1933. Nevertheless , it is not until the 90's when the use of this pontic resurged and was considered a recommended technique.7-22 This technique offers satisfactory functional, periodontal and aesthetic results always provided the case has been carefully selected. Sometimes, to obtain better results, it is necessary to resort to specific periodontal surgical techniques. Authors like Langer and Calanga,23 Cohen24,25 and Garber26 frequently mention the roll technique, the ponch technique, graft of free connective tissue, graft of epithelial connective tissue as well as inlay type graft. These types of procedures allow the remodeling of the alveolar process periodontal architecture, allowing as well the opportunity to create gingival contours to give the prosthesis a natural and aesthetic appearance.
In modern restorative dentistry there is a diversity of prosthetic designs in use. There are also improved systems which combine functional and aesthetic characteristics which improve with the passing of time. The Maryland type prosthesis, popularized at its onset by authors like Howe27 Livatidis and Thompson28 and Rochette29 offers in some cases a conservative manner for tooth preparation. Notwithstanding, the metal substructure of the prosthesis can be seen through the dental structure, giving it a greyish hue and decreasing its value in aesthetic terms. Presently this type of prosthesis has undergone some changes; since the advent of metal free dental materials and new systems this metal translucency constitutes no longer a problem.
CLINICAL CASE PRESENTATION
Clinical case number 1
Three unit fixed partial prosthesis metal free ceramic In-Ceram® (VitaZahnfabrik, Co. KG).
34 year old male patient having a three unit metal-acrylic fixed partial prosthesis from tooth 11 to tooth 22, the pontic was in tooth 21 (Figure 1). The gums presented generalized gingivitis in both arches, nevertheless in the site of the prosthesis there was great increase of fibrous tissue, due to the design and maladjustment of the prosthesis. Coupled with this situation the patient suffered a certain degree of mental impairment. This fact caused a more severe gingival increase due to the patient s difficulty for brushing and the side effects of medication he ingested.

Radiographically a slight horizontal bone loss was observed at the level of interdental crests, the edentulous space was appropriate for the elaboration of a prosthesis. When planning treatment, it was considered to manufacture a metal-porcelain fixed partial prosthesis since the teeth were already worn down for a complete coverage. Nevertheless, for aesthetic and periodontal reasons, a metal free prosthesis of the In Ceram system was selected due to its characteristics of aesthetics, resistance, marginal seal and biocompatibility with gingival tissues.30 Likewise, a gingivoplasty procedure in the anterior maxillary site was recommended to restore an ideal contour to the periodontal architecture of the alveolar process as well as its general periodontal treatment. Once the treatment plan was selected, the metal-acrylic prosthesis was removed, a quick setting self-curing acrylic provisional prosthesis was applied. For this purpose a silicon guide was used, taken before a diagnostic waxing, so as to have the patient ready for the periodontal surgery. The gingivoplasty of the anterior maxillary area was performed with a number 11 scalpel blade, and slice cuts were carried out. Once the desired periodontal architecture contour was achieved, the provisional prosthesis was augmented through the use of Jet (Lang) acrylic® into the mouth. It was trimmed, perfectly polished and provisionally cemented with Tempbond ® cement Finally, a surgical pad was applied to the area and a healing time of 5 months was observed. During this healing period general periodontal treatment was maintained. Once the healing came to its term, the teeth were once more prepared. With a diamond bur shaped like an American football, a 2 to 3 mm niche was prepared in the gum of the edentulous area. This procedure was carried out with the purpose of creating over the gum the gingival contour for an ovoid pontic A three week healing period was observed. The provisional prosthesis was once again put in place. This provisional prosthesis had previously received self-curing acrylic at the base of the pontic to simulate the shape of the niche. The gum was allowed to heal for 3 to 4 weeks (Figure 2). After this period, an impression was taken for the manufacture of the final prosthesis with the use of PVS (polyvinyl siloxane).

The manufacture of the In Ceram ® prosthesis was carried out in two phases: sintering and infiltration. With these processes a substructure of aluminium foil reinforced with zircon glass was established to confer resistance and hardness to the final product. Once the In-Ceram core was obtained, the substructure was ready for the placement of the Vita alpha type dental ceramic. Once the prosthesis was finished, it was tried in the mouth and shape, marginal proximal and incisal contours, texture and marginal sealing were assessed.
There are many criteria for selecting a cement. Conventional cements can be used, such as zinc phosphate, polycarboxilate, resin based cements31 and glass ionomers.32-34 This last one, due to its constant evolution, is highly recommendable: it performs an excellent chemical bond to dentin, presents low solubility to oral fluids, and shows cariostatic properties through its constant release of fluoride. An important characteristic to be taken into consideration is the bonding capacity of the cement to the ceramic system as well as to the remaining tissue and its excellent behaviour when in contact with humidity (Figure 3).

With the use of both periodontal and prosthetic techniques the result is a natural appearance fixed partial prosthesis, which creates the illusion of the pontic emerging through the gum. The use of the ovoid pontic technique allows for functional and favorable aesthetics.
Clinical case number 2
Maryland type prosthesis made of optimized ceramic polymer reinforced with glass fiber. The patient was a 14 year old male student. He presented absence of tooth 11 (Figure 4) due to trauma from a bicycle accident sustained approximately one year before. The patient used as provisional prosthesis a Hawley type retainer. Upon clinical examination, the patient showed moderate gingivitis around the cervical area of the teeth. The edentulous area presented a slightly reduced space in mesiodistal direction for the proper aesthetic manufacture of the prosthesis. Nevertheless, due to the extraction, a collapse of the bone table in vertical and vestibular-palatine direction could be observed.

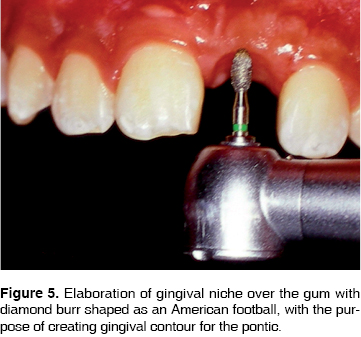
Treatment plan originally contemplated rehabilitation through a dental implant, but for financial reasons this option was discarded. The patient requested a fixed prosthesis, and to preserve his abutment teeth as intact as possible. Therefore, a Maryland type prosthesis was selected, since one of its main indications is a conservative way of dental surface wear, another characteristic of these prostheses is to be able to count with metal free systems for the building of the prosthesis. Prior to the construction of the prosthesis a subepithelial connective tissue graft was placed, for the reconstruction of the defect in the edentulous area of the alveolar process. Once the treatment plan was chosen, periodontal surgery was performed. In this surgery, a flap was raised to uncover the defect zone. A portion of subepithelial connective tissue from the palatine area was taken and placed over the defect area. The flap was sutured and covered with a surgical pad as well as the donor area of the palate. Finally a Hawley type retainer was placed to protect both areas. A healing period of 5 months was observed during which time the treatment was continued. Once the graft healing period had elapsed, a 2 .5 mm deep gingival niche in the edentulous zone was built (Figure 5) with an American football shaped diamond bur to obtain the desired gingival contour for the ovoid pontic.
A Marylan d type design acrylic provisional prosthesis was placed with the aim of simulating the shape of the gingival niche just manufactured. This provisional appliance was adhered with resin, following conventional technique, to obtain temporary results. Once the healing of the gingival niche was completed, an ameloplasty was performed in the mesial area of teeth 12 and 21, to obtain a more appropriate mesio-distal width in the elaboration of the prosthesis. Impression was taken with PVS, and a record was taken with a facial arch (Hanau) to obtain maxillary occlusal plane relationship. Once the master model and the antagonist were obtained, the procedures for the prosthesis elaboration were carried out following the Targis/Vectris® system. This system uses a glass fiber substructure as well as optimized ceramic polymer.35-44 This material allows for good aesthetic and functional results and offers an appropriate security margin for treatment success. Once the prosthesis was finished, it was placed into the mouth, and shape, incisal, marginal and proximal contours were assessed. Texture, color and marginal fit were equally evaluated. With adhesion in mind, cementation was performed with the Variolink II system (Ivoclar, Vivadent)® recommended by the prosthesis elaboration system (Figure 6).

Results obtained with periodontal surgery for the reconstruction of alveolar process defect, offer the necessary circumstances for applying the ovoid pontic technique. It affords, through the gingival niche elaborated in the gum, the creation of the illusion of the pontic emerging from the periodontium. Associated to this, is the fact that through the metal free Targis/Vectris® system (optimized ceramic polymer) satisfactory functional and aesthetic results are obtained.
DISCUSSION
Patients increasingly demand natural looking oral restorations. It is therefore necessary to use all possible resources to obtain predictable functional and aesthetic results, especially in areas where aesthetics is a priority. With the advent of new systems and dental materials for the manufacturing of prostheses, it is possible to attain the desired success; that includes satisfaction of the patient, the dentist and the dental laboratory through a precise diagnosis and proper inter communication. Through experience accumulated with the passing of time in the use of the ovoid pontic as well as with periodontal plastic surgery techniques, aesthetical, functional and natural looking dental treatments can be achieved. Results obtained in these cases can support Dewey6 who, through the use of radicular shaped prosthetic extensions inside the alveoli of recently extracted teeth, stated that there existed a connective tissue formation around the ceramic portion of the root shaped extensions, thus providing a natural and inflammation free appearance around the prosthesis. Studies by Vavazos,45 Constantidines,46 Dylina8 and Bowels46 were also in agreement. These studies assess gingival tissue under pontic moderate pressure, preserving the tissue health free from inflammation and allowing as well the appearance of pontic emergence from the inside of the gingival tissue.
CONCLUSIONS
• Important aesthetic criteria related to periodontal techniques need to be taken into consideration in cases where there are defects in the periodontal architecture of the edentulous alveolar process so as to provide a prosthesis with natural and aesthetic appearance.
• The use of ovoid pontics is another oral rehabilitation technique that can be used in cases where aesthetics is a priority.
• Use of periodontal plastic surgery techniques to rebuild defective alveolar processes is an option within our reach to achieve satisfactory aesthetics results.
• Treatment through the use of ovoid pontic in some cases does not require surgical intervention. Therefore, the formati
on of a gingival niche with a round burr or a burr shaped as an American football does not represent an increase in treatment cost.
REFERENCES
 Mailing Address:
Mailing Address:
Dr. Enrique Rios Szalay
E-mail: enriosza@servidor.unam.mx
Note
This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
1. Abram H, Kopezky RA, Kaplan AL. Incidenece of anterior ridge deformities in partially edetulous patients. J Prosthet Dent 1987; 57: 191-4. [ Links ]
2. Garber DA, Rosenberg SE. The edentulous ridge in fixed prosthodontics. Comp Cont Educ 1981; 2: 212-23. [ Links ]
3. Seibert JS. Reconstruction of deformed partially edentulous ridges, using full thickness onlay grafts. Technique and wound healing. Comp Cont Educ Dent 1983; 17 (Pt 1): 437.54. [ Links ]
4. Behrend DA. The desing of multiple pontics. J Prosthet Dent 1981; 47: 634-8. [ Links ]
5. Howard WW, Ueno H, Pruitt CO. Standards of pontic design. J Prosthet Dent 1982; 47: 493-5. [ Links ]
6. Dewey KW. An experimental study of tissue reactions about percelain root. J Dent Res 1933; 13: 459-72. [ Links ]
7. Basseltt JL. Replacement of missing mandibular lateral incisor whit a single pontic all-ceramic prosthesis: A case report. Prac Periodont Anesthet Dent 1997; 9: 455-61. [ Links ]
8. Dylina TJ. Contour determination for ovate pontic. J Prosthet Dent 1999; 82: 136-42. [ Links ]
9. Howard NY. Optimizing anterior esthetic: Combining porcelain and periodontal considerations in single-tooth replacement: A case report. J Esthet Dent 1997; 9: 295-305. [ Links ]
10. Kern M, Thompson VP. Bonding to glass infiltrated alumina ceramics: Adhesive methods and their durability. J Prosthet Dent 1995; 73: 240-9. [ Links ]
11. Posdhadley AG. Gingival response to pontics. J Prosthet Dent 1968; 19: 51-6. [ Links ]
12. Prestipino V, Passero P, Ingber A, Wyman B. Preserving the topography of the extraction site: The external gingival support splint. J Esthet Dent 1994; 6: 259-66. [ Links ]
13. Reel DC. Establishing esthetic contours of the partially edentulous ridge. Quintessence 1988; 19: 301-10. [ Links ]
14. Rufenacht C. Fundamentals of esthetic . Quintessence Publishing Co; 1990: 263-77. [ Links ]
15. Salama H, Salama MA, Garber D, Adar P. The interproximal height of bone: A guide post to predictable a esthethic strategies and soft tissue contours in anterior tooth replacement. Prac Periodont Anesthet Dent 1988; 10 (9): 1131-41. [ Links ]
16. Serio FG, Strassler HE. Periesthethic troubles hooting solutions for the unexpected. J of Esthet Dent 1997; 9: 317-26. [ Links ]
17. Smidt A, Goldstein M. Augmentation of a deformed residual ridge for the replacement of a missing maxillary central incisor. Prac Periodont Anesthet Dent 1997; 11 (2): 229-32. [ Links ]
18. Spear FM. Maintenance of the interdental papilla following anterior tooth removal. Prac Periodont Anesthet Dent 1999; 11: 21-8. [ Links ]
19. Stein RS. Pontic residual ridge relationship: A case report. J Prosthet Dent 1996; 16: 251-84. [ Links ]
20. Studer S, Zellweger, Scharer P. The aesthetic guidelines of the mucogingival complex for fixed prosthodontics. Prac Periodont Anesthet Dent 1996; 8: 333-41. [ Links ]
21. Trushkowsky R. Esthetic alternative to conventional resin-bonded fixed partial denture whit in-ceram. J of Esthet Dent 1994; 6: 115-20. [ Links ]
22. Zitamann NV, Marinello CP. Anterior single-tooth replacement. Clinical examination and treatment planning. Prac Periodon Anesthet Dent 199; 11 (7): 847-58. [ Links ]
23. Langer B, Calanga L. The subepitelial connective tissue graft. J Prosthet Dent 1980; 44: 363-7. [ Links ]
24. Cohen ES. Ridge augmentation utilizing the subepitelial connective tissue graft: A case report. Prac Periodont Anesthet Dent 1994; 6: 47-53. [ Links ]
25. Cohen ES. Ridge enhancement and socket preservation utilizing the subepitelial connective tissue graft: A case report. Prac Periodont Anesthet Dent 1995; 7: 53-8. [ Links ]
26. Howe DF. Anterior fixed partial denture utilizing the acid etch technique and a cast metal framework. J Prosthet Dent 1997; 37: 28-35. [ Links ]
27. Livatidis GJ, Thompson PV. Etched casting: An improved retentive mechanism for resin-bonded retainers. J Prosthet Dent 1982; 47: 52-8. [ Links ]
28. Rochette AAL. Attachment of a splint to enamel of lower anterior teeth. J Prosthet Dent 1973; 30 (4): 418-23. [ Links ]
29. Sorensen JA, Torres TJ. Marginal fidelity of ceramic crowns whith different margin desing. J Dent Res 1990; 69: 279-85. [ Links ]
30. Kern M, Glaser R. Cantilevered all-ceramic resin-bonded fixed partial dentures: A new treatment modality. J Esthet Dent 1997; 9: 255-64. [ Links ]
31. Christensen GJ. Glass ionomer as a luting material. J Am Dent Assoc 1990; 120: 59-62. [ Links ]
32. Johnson GH, Powell LV, Derouen TA. Evaluation and control post-cementation pulpal sensitivity: Zinc phosphate and glass ionomer luting cements. J Am Dent Assoc 1993; 124: 39-46. [ Links ]
33. McComb D. Retention of casting whit glass ionomer cement. J Prosthet Dent 1982; 48 (3): 285-8. [ Links ]
34. Bartsch F. El Puente inlay con la técnica Targis/Vectris. Rev Int Téc Dent 1999: 2-15. [ Links ]
35. Bischoff H, Neubarth C, Pohl F. A somewhat unsual clinical ase restoration whit Targis/Vectris. Quintessence 1997; 23 (6): 776-87. [ Links ]
36. Clunet-Cose B. Targis/Vectris. Ivoclar 1997 Feb. Informe Técnico No. 124: 1-5.
37. Dickerson WG, Rinaldi Peter. The fiber-reinfoced inlay-supported indirect composite bridge. Prac Periodont Anesthet Dent 1996; Suplement: 1-4. [ Links ]
38. Fahl N, Cassellini RC. Tecnología FCR/Cerómero: El futuro de la odontología estética adhesiva biofuncional. Signature 1998; 3: 5-11. [ Links ]
39. Feinman RA, Smidth A. A combination porcelain/fiber reinforced composite bridge: A case report. Prac Periodont Anesthet Dent 1997; 9: 925-9. [ Links ]
40. Hornbook DS. Placement protocol for an anterior fiber-reinforced composite restoration. Prac Periodont Anesthet Dent 1997; 9: 1-5. [ Links ]
41. Korber S, Korber H. Puente fijo de fibra de vidrio. Primeros resultados de la prueba clínica del puente fijo de fibra de vidrio. Targis/Vectris. Informe técnico. Quintessence 3a. Edición 1996.
42. Korber K. El sistema de puente fijo reforzado con fibra de vidrio Targis/Vectris. Valoración de la técnica de aplicación. Quintessece 1997; 48 (6): 839-60. [ Links ]
43. Rosenthal L, Trinkner T, Pescatore C. A new system for posterior restorations : a Combination of ceramic optimized polymer and fiber reinforced composite. Prac Periodont Anesthet Dent 1997; 9: 6-10. [ Links ]
44. Cavazos E. Tissue response to fixed partial denture pontics. J Prosthet Dent 1968; 20: 143-53. [ Links ]
45. Tripodakis AP, Constantidines TA. Tissue response under hyperpressre from convex pontics. J Periodontics Restoratire Dent 1990; 10(5): 408-14. [ Links ]
46. Bowels RO. Fixed bridges whit special reference to tissue contact pontics and inlay abutments. J Am Dent Assoc 1931; 1521-32. [ Links ]

