










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista odontológica mexicana
Print version ISSN 1870-199X
Rev. Odont. Mex vol.15 n.4 Ciudad de México Oct./Dec. 2011
Original research
Short term determination of effectiveness and sustainability to fight halitosis of three commercial mouthwashes
Luis Fernando Jacinto Alemán,* Juan Carlos Hernández Guerrero,* Maria Dolores Jiménez Farfán,* Armando López Salgado§
* Immunology Laboratory, Graduate and Research Division, School of Dentistry, National University of Mexico (UNAM).
§ Fixed and Removable Prosthesis Department, Graduate and Research Division, School of Dentistry, National University of Mexico (UNAM).
Received: 22 March 2010.
Accepted: 11 May 2010.
ABSTRACT
Introducción: Halitosis is an adverse emission of odour from the oral cavity. Approximately 90% of all halitosis cases are related to oral health. Volatile sulphide compounds (VSC) constitute the main component of halitosis, they are produced by anaerobic bacteria located on the dorsum of the tongue and in periodontal pockets. Mouthwashes with antimicrobial agents are effective in the treatment of halitosis, Nevertheless, commercial diversity presents a problem when choosing the right one. Objetive: To determine the effectiveness and sustainability of three commercial mouthwashes against the halitosis. Material and methods: 78 participants were randomly divided into one control and three experimental groups. Organoleptic measurements and basal levels of VSC were taken at 1, 3 and 24 hours after use. Central tendency dispersion measurement and statistical analysis were established. Results: The findings of this research indicate a decrease in organoleptic levels and VSC after 1st and 3rd hour use of mouthwashes in three experimental groups. Conclusions: Results obtained in the present study indicate that mouth rinsing with essential oils, triclosan and cetylpirydine chloride represents a positive option for the treatment of halitosis.
Key words: Halitosis, mouthwashes, sustainability, VSC.
INTRODUCTION
Halitosis, or bad breath is an unfavourable social and physical condition affecting the human race; oral microflora is rated as the main etiologic factor.1 Halitosis can be classified into true halitosis, pseudohalitosis and halitophobia. True halitosis can be subdivided into physiological halitosis, that is, when no evident systemic disease or pathological affliction can be found to originate the bad breath, and pathological halitosis which occurs as a result of infectious disease in the oral tissues. Pseudohalitosis is a mental disorder in which patients believe they have bad breath and nevertheless there is no halitosis. Halitophobia occurs when there is no physical or social proof to indicate the presence of halitosis before or after treatment.2
Volatile sulphide compounds (VSC) especially hydrogen sulphide, methyl mercaptan and dimethylsulphide are the main components of bad breath.3 These compounds are produced by gram negative bacteria located in the tongue dorsum and periodontal pockets. They metabolize diet aminoacids into byproducts containing sulphide or VSC, and this, even in small concentrations, causes foul odour. Caries and periodontal disease can modify the composition of microflora, and therefore, cause halitosis.4,5
The best part of treatments designed to counterattack halitosis are based on elimination or decrease of dental bacterial plaque, as well as VSC levels through physical or chemical mechanisms to be implemented during oral hygiene practices. A very popular halitosis treatment is the use of a mouthwash before of after brushing teeth. Nevertheless, the great diversity of compounds and substances such a cetylpiridinium chlorhide, clorhexidine, triclosan and essential oils, among others, can hinder the choices of patients interested in eliminating halitosis.6
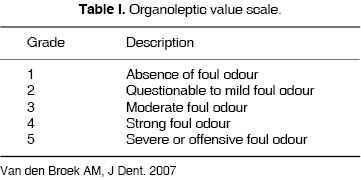
The most accurate technique to use, within methods used to qualify halitosis, is the organoleptic test through a qualified judge. In this test, the judge rates halitosis degrees into five categories. Another test to determine VSC levels would be through the use of instrumental techniques (gas chromatography or portable sulphide meter).7,8 The aim of this research was the short term evaluation with respect to effectiveness and sustainability for the elimination of halitosis of three commercial brands of mouthwashes.
MATERIALS AND METHODS
The study group was composed by 78 subjects (57 women and 21 men), selected from a population of 127 patients who attended private practice appointments. All of them presented adequate conditions of oral, periodontal and general health. Admittance criteria were: presence of at lest 20 natural teeth, and minimum grade of two in the organoleptic test. Dismissal criteria were: severe caries, presence of oral or general disease (with exception of carcinomas, adenocacinomas and diabetes), history of allergy to oral hygiene products, use of drugs or antibiotics during the month previous to the initiation of the study, previous oral surgery, presence of periodontitis and pregnancy. All included participants granted written consent. Participants were instructed in the (Stillman) brushing technique, without toothpaste and a soft Oral B brush (Oral B, Procter & Gamble,® USA).
Participants received instructions with respect to restrictions to be observed during the study period. Neither participants, nor qualifying judge could ingest food for the 90 minutes preceding the basal measurement. They were instructed as well to refrain from smoking, drinking alcoholic beverages and eating hot and spicy foods 24 hours before the basal measurement. They were advised to avoid use of scented products (soap and/or deodorants) during the study. Participants were randomly divided into four groups; three were experimental groups: Triclosan (T Total Plax Original, Colgate ®), Essential oils (EO, Listerine Original Antiseptic Johnson & Johnson®) and cetylpirydinium chlorhide (CC, Astringosol, Complete, Mouth Wash GlaxoSmithKline®) and one control group (deionized water).
The study was divided into five stages:
Stage 1: Basal level measurements were carried out following organoleptic technique and VSC measurement. Organoleptic measurement consisted in the perception of breath of every participant, at a 30 cm distance and made by a judge who qualified the perception of the aroma according to a scale (Table I). The organoleptic examiner had to include the following characteristics: non smoker, non drinker, lacking systemic diseases (conditions) and observing a 20 minute recess between one examination and the next. VSC measurement was achieved with a Halimeter or portable monitor (Halimeter, Brochure 2004, range 0-400mV=0-1999 ppb.Interscan Corp®, Chatworth CA). To obtain the level of VSC in parts per billion (ppb) each patient took the aspiration pipette in the mouth, holding it with lips only, and blowing softly during a minute.
Stage 2: According to the treatment group where he was assigned, each participant rinsed his mouth with 20ml of the designated product during 30 seconds (CC and EO groups) and 60 seconds (T group) according to instructions of the manufacturer.
Stage 3: One hour after rinsing, new organoleptic and VSC levels were measured. Restrictions to be observed were repeated to the patients.
Stage 4: Three hours after the initiation of the procedure new organoleptic and VSC levels were recorded. Restriction parameters were reinforced with the patients. Patients were also explicitly told to brush their teeth only with the designated toothbrush without use of any dental paste.
Stage 5: Twenty-four hours after basal measurement and having asked the patient to brush his teeth, organoleptic and VSC measurements were taken of all participants.
For both results (organoleptic and VSC levels) mean and standard deviation were obtained. Statistical analysis of organoleptic and VSC results were undertaken through the ANOVA test of repeated measurements (p ≤ 0.05) using software SPSS 13 (Chicago Il).
RESULTS
The study was composed of 78 Hispanic origin participants, mean age 27.05 years (± 8.12 years), ages ranging from 18-43 years. Twenty one participants (27%) were male and 57 (73%) female. Twenty seven participants (35%) were smokers and 46 (59%) reported alcohol consumption. Control group consisted of 18 participants; group T was formed by 21 participants, group EO counted with 20 and group CC was formed by 219 subjects. The global basal result of the organoleptic test was 2.56. VSC levels were 213.57 ppb in all 78 participants, nevertheless men presented higher values of organoleptic and VSC levels (Table II). Statistical analysis of measurements repeated for each group indicated that the accomplished reductions were significant (Tables III and IV). In group T organoleptic analysis indicated important decreases during the first and third hour (42.59 and 11.72% respectively). VSC levels decreased in the first and third hour in 28.94% and 8.71% respectively. During the same period, Group EO showed reductions of 62.5% and 43.73% organoleptic measurement, and 35.77% and 19.85% in VSC levels. Organoleptic measurement for group CC showed a 37.38 and 18.57% reduction after 1st and 3rd hour measurement, and VSC levels showed reductions of 18.8% and 6.78% respectively in the first and third hour (Tables III and IV).
DISCUSSION
The present essay was designed to determine the short term effect of mouthwashes in halitosis treatment. Each product's 24 hour sustainability was analyzed. Three organoleptic and VSC level measurements were taken after using each mouth rinsing agent. It was found that all three mouth rinses promoted important reductions in measurements taken 1 hour and three hours after use, nevertheless, none of them generated decreases 24 hours after use. Mean age of the sample was 27.05 ± 8.12 years, ages ranging from 18 to 43 years. Participants were mainly in the third decade of life. It must be considered that halitosis is not only a health disorder, it is also an unwanted social condition affecting personal relations among young adults.1,8 This can be promoted by social habits and behaviours which could increase the risk of suffering halitosis, like alcohol and tobacco consumption.9 This study showed that 35 and 59% of the subjects in the sample were, respectively, smokers and drinkers. These two conducts increase the risk of suffering gastritis and peptic ulcers, conditions which increase halitosis. It is crucial for dentists to support the patient and follow up his changing of habits to improve his general health and thus eliminate halitosis.10
Results of this study indicate that group T showed important reductions in the organoleptic test as well as in the VSC levels taken 1 hour and 3 hours after use of the mouthwash. Moran & al11 showed that mouthwashes containing triclosan did not present effective sustainability 24 hours after use. This could be due to variable solubility and bioavailability patterns, according to the diluent used. Nevertheless it has been demonstrated that this composite can decrease plaque in 20-30% and could thus, not only help in reducing halitosis but also help decrease other oral disorders like caries and periodontitis.12
Group EO showed higher reduction percentages for both measurements in the first and third hour. Originally essential oils were considered agents that masked bad breath, nevertheless, recent evidence has shown them to be agents with ability to decrease oral microflora. Bauroth,13 in a long term study, demonstrated the effectiveness of these composites in gingivitis treatment, since they promote a reduction in plaque levels, even in interproximal areas. It has also been demonstrated that a brief and prolonged use of these agents promotes reduction of supragingival and subgingival plaque and of bacteria like Capnocytiphaga sp, F nucleatum, Vellionella sp, all which could be indirectly related with VSC level reduction.14 It is important to point out that recent research question chronic usage of alcohol containing mouth washes, among which can be counted those with essential oils, since they can be considered as an impending risk for the development of oral neoplasia.15 Cetylpirydinium chlorhide is an ammonia quarternary cationic antiseptic with proven antimicrobial activity. This composite, combined with chlorhexidine and zinc lactate, has been used for halitosis treatment and microorganism reduction of supragingival plaque and saliva in a two week treatment.16 Results of group CC showed a lower percentage of basal reduction, this can be due to the fact that perhaps a more prolonged usage might be required to obtain stronger effectiveness. This composite is water and alcohol soluble, has the ability to reduce superficial tension and counts with a broad spectrum over varied microorganisms including bacteria and fungi of the oral microflora. All the aforementioned properties make this composite a positive alternative for halitosis treatment.17
CONCLUSIONS
People wanting to solve halitosis problems face the dilemma of selecting the proper oral mouthwash due to the variety of available products in the market.
Based on results obtained in this study, we observed the behaviour of three experimental groups with three different active substances. Results obtained showed that all three groups presented significant reductions in organoleptic measurements and VSC levels, in measurements taken 1 hour and three hours after usage of the mouthwash. Group EO showed greater reduction followed by group T, and finally group CC. In all three groups no sustainable result was observed after 24 hours of usage of the mouthwash. Dentists should not only recommend a mouthwash when patients request it, the dentists main objective must be to diagnose each parameter on the etiology of that case of halitosis, and thus design and implement all-encompassing strategies which will produce the best results as well as patient's satisfaction.
REFERENCES
 Mailing Address:
Mailing Address:
Luis Fernando Jacinto Alemán
Laboratorio de Inmunología,
División de Estudios de Postgrado e Investigación, Facultad de Odontología,
Universidad Nacional Autónoma de México,
D.F. 04510. México.
E-mail: inmuno1@live.com.mx
Note
This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
1. Bosy A. Oral malodor: philosophical and practical aspects. J Can Dent Assoc 1997; 63 (3): 196-201. [ Links ]
2. Zbys F, Hamad A, Mona N, Trent O, Vinícius P. Enjuagues bucales para el tratamiento de la halitosis (Revisión traducida) . En: La biblioteca Cochrane Plus 2008, Numero 4. Oxford: Update Software Ltd. Disponible en http://www.update-software.com (Traducida de Cochrane Library, 2008 Issue 3. Chichester, UK: John Wiley & Sons, Ltd.
3. Young A, Jonski G, Rölla G. Variation in oral volatile sulphur compound formation. Acta Odontol Scand 2002; 60 (6): 321-324. [ Links ]
4. Socransky SS, Manganiello SD. The oral microbiota of man from birth to senility. J Periodontol 1971; 42 (8): 485-496. [ Links ]
5. Wåler SM. On the transformation of sulfur-containing amino acids and peptides to volatile sulfur compounds (VSC) in the human mouth. Eur J Oral Sci 1997; 105 (5 Pt 2): 534-537. [ Links ]
6. Roldán S, Herrera D, O'Connor A, González I, Sanz M. A combined therapeutic approach to manage oral halitosis: a 3-month prospective case series. J Periodontol 2005; 76 (6): 1025-1033. [ Links ]
7. Tonzetich J. Direct gas chromatographic analysis of sulphur compounds in mouth air in man. Arch Oral Biol 1971; 16 (6): 587-597. [ Links ]
8. van den Broek AM, Feenstra L, de Baat C. A review of the current literature on aetiology and measurement methods of halitosis. J Dent 2007; 35 (8): 627-635. [ Links ]
9. Suzuki N, Yoneda M, Naito T, Iwamoto T, Yamada K, Hisama K, Okada I, Hirofuji T. The relationship between alcohol consumption and oral malodour. Int Dent J 2009; 59 (1): 31-34. [ Links ]
10. Loesche WJ, Kazor C. Microbiology and treatment of halitosis. Periodontol 2000 2002; 28: 256-279. [ Links ]
11. Moran J, Addy M, Newcombe RG, Marlow I. A study to assess the plaque inhibitory activity of a new triclosan mouthrinse formulation. J Clin Periodontol 2000; 27 (11): 806-809. [ Links ]
12. Cummins D, Creeth JE. Delivery of antiplaque agents from dentifrices, gels, and mouthwashes. J Dent Res 1992; 71 (7): 1439-1449. [ Links ]
13. Bauroth K, Charles CH, Mankodi SM, Simmons K, Zhao Q, Kumar LD. The efficacy of an essential oil antiseptic mouthrinse vs. dental floss in controlling interproximal gingivitis: a comparative study. J Am Dent Assoc 2003; 134 (3): 359-365. [ Links ]
14. Fine DH, Markowitz K, Furgang D, Goldsmith D, Charles CH, Lisante TA, Lynch MC. Effect of an essential oil-containing antimicrobial mouthrinse on specific plaque bacteria in vivo . J Clin Periodontol 2007; 34 (8): 652-657. [ Links ]
15. Werner CW, Seymour RA. Are alcohol containing mouthwashes safe? Br Dent J 2009; 207 (10): 488-489. [ Links ]
16. Roldán S, Winkel EG, Herrera D, Sanz M, Van Winkelhoff AJ. The effects of a new mouthrinse containing chlorhexidine, cetylpyridinium chloride and zinc lactate on the microflora of oral halitosis patients: a dual-centre, double-blind placebo-controlled study. J Clin Periodontol 2003; 30 (5): 427-434. [ Links ]
17. Hu D, Li X, Sreenivasan PK, DeVizio W. A randomized, double-blind clinical study to assess the antimicrobial effects of a cetylpyridinium chloride mouth rinse on dental plaque bacteria. Clin Ther 2009; 31 (11): 2540-8. [ Links ]

