










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista odontológica mexicana
Print version ISSN 1870-199X
Rev. Odont. Mex vol.15 n.3 Ciudad de México Jul./Sep. 2011
Case report
Squamous cell carcinoma in the tongue and Plummer-Vinson syndrome. A case report
Alejandro Donohue-Cornejo,* Dalia Abril Guzmán-Gastelum,* Daniel Constandse-Cortéz,* Luis Alberto Gaitán-Cepeda,§ Carlos Reyes Escalera§
* Stomatology Department, Biomedical Sciences Institute, Ciudad Juárez University.
§ Clinical and Experimental Pathology Laboratory, Graduate School, School of Dentistry, National University of Mexico.
Received: 06 May 2010.
Accepted: 29 June 2010.
ABSTRACT
The Plummer-Vinson syndrome, called sideropenic dysphagia, is characterized by dysphagia, iron deficiency, anemia and the presence of esophageal webs, and it has been identified as a risk factor for developing squamous cell carcinoma of the upper gastrointestinal tract. The cases of patients suffering Plummer-Vinson syndrome that develops intraoral carcinomas are very rare. We present one case of 45 years-female with diagnosis of sideropenic dysphagia who develops a squamous cell carcinoma of the tongue. The patient present at Oral Medicine and Oral pathology clinic at Dental School of the Autonomous University of Ciudad Juárez, México by glossodynia, glossopyrosis and dysphagia of 8 months of evolution. The medical file revealed antecedents of non-specified chronic anemia, with blood transfusions at medical institutions. The intraoral examination showed depapilation of two anterior thirds of the tongue. An ulcerated swallow with indurate borders site in the left lateral border of the tongue of unknown evolution was observes. An incisional biopsy was done and a histopathological diagnosis of squamous cell carcinoma of the tongue was emitted. In our knowledge this is the third case reported in the scientific literature of a lingual squamous cell carcinoma develops in a patient suffering Plummer-Vinson syndrome. The 3 reported cases are coincident in age, gender and oral features. The pertinence of to continue including to sideropenic dysphagia like a risk factor to develop intra-oral carcinomas is discuses.
Key words: Plummer-Vinson syndrome, sideropenic dysphagia, squamous cell carcinoma, tongue.
INTRODUCTION
Plummer-Vinson syndrome is a rare syndrome characterized by dysphagia, esophageal webs and chronic iron deficiency anemia. Oral characteristics include glossitis, glossopyrosis, glossodynia, and angular cheilitis.1 Its etiology is unknown although autoimmune, genetic, infectious and nutritional factors have been proposed as a cause.2 Approximately 10% of patients suffering Plummer-Vinson syndrome develop squamous cell carcinoma principally in the hypopharynx and esophagus.3 Reported cases of patients suffering Plummer-Vinson syndrome who develop oral squamous cell carcinomas are scarce. Cases of squamous cell carcinoma in the tongue are even rarer.2 In order to increase the knowledge of the association between oral squamous cell carcinoma and Plummer Vinson syndrome, a case of a patient with diagnosis of Plummer Vinson syndrome who developed squamous cell carcinoma of the tongue is reported.
CASE REPORT
In May 2004, a 45 years female came to the Oral Medicine and Oral Pathology clinic at Dental School of the Autonomous University of Ciudad Juárez (México). She presented dysphagia, glossodynia and glossopyrosis. The dysphagia had approximately eight months of evolution, having increased in the past six months. The glossodynia and glossopyrosis were constant and exacerbated with hot or spicy foods. A history of unspecified chronic anemia treated with several hematologic transfusions was mentioned in the anamnesis. A weight loss greater than 10% of the total body weight of unexplained origin was also referred. The esophageal endoscopy, performed by a private physician, identified esophageal webs. The blood cells analysis showed low hematocrit and hemoglobin values as well as anisocytosis and hypochromic microcytosis. The iron's kinetic test corroborated iron deficiency. For all the aforementioned reasons, a diagnosis of Plummer-Vinson syndrome was emitted, and consequently treatment with iron supplement was initiated.
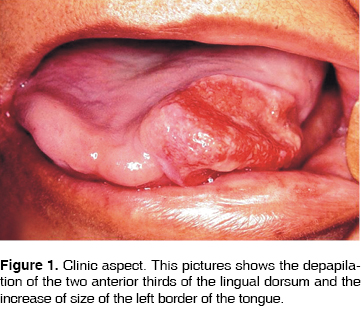
The intraoral physical examination revealed atrophy of the dorsum of the two anterior thirds of the tongue. In the left lateral border of the tongue a size increase of unknown evolution was observed. The tumor mass extended towards the dorsum and ventral region of the tongue. Clinically, this lesion was composed by an erythematous-whitish ulcer of irregular borders (Figure 1). To palpation the tumor was firm and painful. The patient disacknowledged alcoholic and smoking habits. With a presumptive diagnosis of squamous cell carcinoma, the patient was referred to the maxillofacial surgery clinic of the same institution for incision biopsy. The surgical sample was fixed at 10% buffered formalin, embedded in paraffin and cut at 5 micrometers, to be stained with the Hematoxylin and Eosin stain technique.
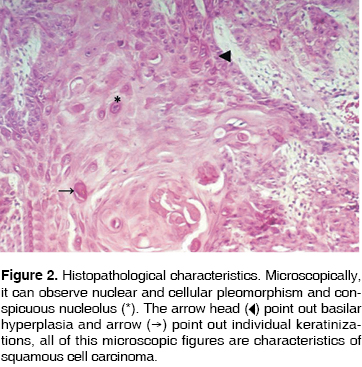
Microscopically the lesion was characterized by neoplastic cells of epithelial origin, with individual or group keratinizations; cellular and/or nuclear pleomorphism; hyperchromatic nuclei; increased mitosis and abnormal mitosis (Figure 2). The basal membrane was lost with infiltration of neoplasic epithelial cells into muscle and connective tissue. A diagnosis of squamous cell carcinoma of the tongue was emitted. The patient was referred to an Oral Cancer Center to receive surgical and radiotherapy treatment. To date, after 5 years, the patient is in remission and under close follow up.
DISCUSSION
It has been proposed that patients suffering Plummer-Vinson syndrome show increased sensitivity to develop squamous cell carcinoma. This leads to consider Plummer-Vinson syndrome as a pre-cancerous condition to esophagus and stomach.4 An increased incidence of post-cricoid squamous cell carcinoma is associated with Plummer-Vinson syndrome. The association between Plummer-Vinson syndrome and pseudopapilar carcinoma of the pancreas5 has also been suggested. Although the etiology of Plummer-Vinson syndrome is unknown, iron deficiency has been suggested as the principal factor in its development. The epithelium of the upper digestive tract is susceptible to iron deficiency because its fast cellular exchange rate produces a decrease in the iron-dependent enzymes.1 Therefore, epithelial changes observed in patients with Plummer-Vinson syndrome may be due to a depletion of the oxidative enzymes of epithelial cells. This change produces atrophic glossitis, angular cheilitis, coiloniquia, fragility and thinning of nails, brittle hair, and of particular relevance to this report, promotes the development of squamous cell carcinomas.6 However in some patients, iron therapy is insufficient to reverse the changes and improve patients afflicted with sideropenic dysphagia. For the aforementioned reasons, it has been proposed that factors other than iron deficiency exist in the pathogenesis of the syndrome.1
In scientific literature, to our knowledge, only two cases of squamous cell carcinoma developed in the tongue of Plummer-Vinson syndrome patients have been reported.7,8 In 1967, a 52-year female with iron deficiency and squamous cell carcinoma of the dorsal surface of the tongue was reported.7 In 1970, Santoro et al8 reported a case of a 42-year old woman afflicted with dysphagia, anemia, and asthenia who clinically showed loss of lingual papilla and presence of a firm borders lingual ulcer. Histopathologically, the diagnosis of squamous cell carcinoma was also confirmed. The clinical description of only two reported cases of lingual squamous cell carcinoma in patients with Plummer-Vinson syndrome is coincident with the case presented here, e.g. women in their fifth decade showing a bordered firm ulcer located in the posterior area of the lateral borders of the tongue.
The etiology of the squamous cell carcinoma of the tongue is associated with tobacco and alcohol consumption.9-11 The medical file of the present case didn't show any habit (alcohol, tobacco), suggested as in association with Plummer-Vinson syndrome. However, the fact that in the last decade the presence of squamous cell carcinoma of the oral cavity,10 especially in the tongue,11 has been reported in young subjects who had not been exposed to risk factors raises the possibility that in the present case, both entities have developed simultaneously.
It is important to point out that the Plummer-Vinson syndrome has been definite as a risk condition for the development of oral cavity squamous cell carcinoma. Review of the literature shows few reported cases of squamous cell carcinoma of the oral cavity in patients with Plummer-Vinson syndrome. The latest one reported a patient with celiac disease and Plummer-Vinson syndrome also affected with lingual squamous cell carcinoma.2 The only two reports of patients with carcinoma of the oral cavity also suffering of Plummer-Vinson syndrome have been published over 30 years ago. A possible reason for this fact could be that the Plummer-Vinson syndrome is associated with vulnerable social conditions, specifically poverty and malnutrition; therefore, improvements in socio-economic changes in different societies will bring as a consequence a decrease in incidence and prevalence of this syndrome. This supposition was established by the mid-70's3 and subsequently confirmed in Swedish population.12 However, in developing or underdeveloped countries where malnutrition could be a common event, the general dentist, and in particular the specialist in oral medicine must be alert to the presence of probably malignant lesions in women afflicted malnutrition (anemia) and lingual depapilation.
REFERENCES
 Mailing Address:
Mailing Address:
Dr. Luis Alberto Gaitán Cepeda
Laboratorio de Patología Clínica y Experimental,
División de Estudios de Posgrado e Investigación,
Facultad de Odontología,
Universidad Nacional Autónoma de México.
Circuito institutos s/n Ciudad Universitaria,
Coyoacán 04510, Distrito Federal, México
Teléfono/Fax:(52) 55-56-22-55-59
E-mail: lgaitan@servidor.unam.mx
Note
This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
1. Novacek G. Plummer-Vinson syndrome. Orphanet J Rare Diseases 2006; 1: 36. doi. 10.1186/1750-1172-1-36. [ Links ]
2. Jessner W, Vogelsang H, Püspök A, Ferenci P, Gangl A, Novacek G, Bodisch A, Wenzl E. Plummer-Vinson syndrome associate with celiac disease and complicated by postcricoid carcinoma and carcinoma of the tongue. Am J Gastroenterol 2003; 98 (5): 1208-9. [ Links ]
3. Larsson LG, Sandström A, Westling P. Relationship of Plummer-Vinson disease to cancer of the upper alimentary tract in sweden. Cancer Res 1975; 35(11 pt2): 3308-16. [ Links ]
4. Kim KH, Kim MC, Jung GJ. Gastric cancer occurring in a patient with Plummer-Vinson syndrome. World J Gastroenterol 2005; 11 (44): 7048-50. [ Links ]
5. Khan FY, EL-Hiday AH, Morad NA. Plummer-Vinson syndrome associated with solid pseudopapillary tumor of the pancreas. Chin Med J 2007; 120 (17): 1553-5. [ Links ]
6. Rincón SRA, Hani AA, Alvarado BJ. Síndrome de Plummer-Vinson. Rev Col Gastroenterol [online]. 2004; 19 (4): 288-29. [ Links ]
7. La Grassa M, Tamburo De Bella A, Beltrame A. The Plummer-Vinson syndrome within the general pictures of precancerous condition of the tongue. Riv Ital Stomatol 1967; 22 (12): 1458-71. [ Links ]
8. Santoro E, Gambardella P, Piscicelli I. On the Plummer-Vinson syndrome with precancerous lesion of tongue. Rass Int Clin Ter 1970; 50 (12): 753-61. [ Links ]
9. Just-Sarobé M. Smoking and skin. Actas Dermosifilogr 2008; 99 (3): 173-84. [ Links ]
10. de Moura CMJR, Alves HH, de Souza L, Livingstone D, Hardy MD, Costa TR, Mamede RCM. Prognostic factors in squamous cell carcinoma of the oral cavity. Rev Bras Otorrinolaringol 2008; 74: 861-6. [ Links ]
11. Wang YH, Chen YF, Guo ZM, Zhang Q, Liu TR, Chen FJ. Reason for recurrence and prognostic analysis of early stage squamous cell carcinoma of the oral tongue. Chin J Can 2009; 28 (5): http://www.cjcsysu.cn/cn/article.asp?id=15334 [ Links ]
12. Wahlberg PC, Andersson KE, Biörklund AT, Möller TR. Carcinoma of the hypopharynx: analysis of incidence and survival in Sweden over a 30-year period. Head Neck 1998; 20 (8): 714-9. [ Links ]

