










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.15 no.3 Ciudad de México jul./sep. 2011
Case report
Congenital adrenal hyperplasia salt loss. Clinical case
Nitzia Ayared Díaz García,* Ávalos Verónica Ávalos,* Rodolfo Fragoso Ríos,§ Vicente Cuairán RuidíazII
* Dentist, Specialist in Pediatric Stomatology.
§ Head of the Stomatology Pediatric Service-Mexico Children's Hospital Federico Gómez.
II Head of the Stomatology Department, Mexico Children's Hospital Federico Gómez.
Received: 5 November 2007.
Accepted: 26 February 2008.
ABSTRACT
Hereditary disorders related to the adrenal glands, with a deficient production of hormones (cortisol and aldosterone), and an androgen overproduction.1 Clinical manifestations: hypotension, anorexia, nausea, abdominal pain, hyperpigmentation of skin folds and palm lines. Girls present: ambiguous genitals, pubic, axillary and facial hair, hoarse voice, abnormal menstrual periods. Boys present precocious development, alterations in genitals, pubic and axillary hair.2 Oral manifestations are: hyperpigmentation around the lips, mucosa and gingival margin. A clinical case is presented of a six-year old female patient diagnosed with salt losing CAH or CAH seeking treatment at the Hospital Infantil de México Federico Gómez (HIMFG) (Federico Gomez Mexico s Children Hospital ). The dental department specialist sought inter-consultation with the Endocrinology Department in order to plan a dental treatment for the patient. Treatment consisted of stainless steel crowns and extraction of primary teeth. Pits and fissures sealants were applied, brushing techniques were taught and fluoride gel was applied. As an anti stress preventive measure, the patient's daily steroid dose was adjusted to avoid acute adrenal failure. The patient s hypertensive medication was not suspended. Amoxicillin (50 mg) was used an hour before the procedure as an antibiotic prophylactic measure. Multidisciplinary services ensure effective and safe dental procedures.
Key words: Congenital adrenal hyperplasia, antistress.
INTRODUCTION
Adrenal Hyperplasia refers to a group of inherited disorders of the adrenal gland, characterized by a deficiency of the hormones cortisol and aldosterone and an overproduction of androgen, it is inherited as an autosomal recessive form. Its main effect is the lack of an enzyme (21-hydroxylase), required by the adrenal glands to produce the cortisol and aldosterone hormones. (3) Due to blockage of the hormone synthesis, there is an abnormal feedback, and steroids are transformed into androgens, which produce an early appearance of male characteristics.4
There are two kinds of CAH: severe (loss of salt) which is the most common, and presented in this case, and mild (which leads to neither genital ambiguity nor salt loss).
Congenital adrenal hyperplasia (CAH) presents as clinical characteristics a defect in the biosynthesis of cortisol. The decrease in the production of cortisol determines a compensatory increase of Adrenocorticotrophic Hormone (ACTH), this hormone stimulates steroid synthesis and results in overproduction of steroids without blockage.
Clinical characteristics of CAH are: in most severe cases, a complete absence of adrenal cortex function, patients present salt loss crisis and neonatal genital virilization that determines genital ambiguity in female newborns (classical salt-loss type).5
Some oral manifestations are hyperpigmentation around lips, mucosa and gingival margin.6
CAH diagnosis is based on family medical history, genetic tests to determine the sex of the newborn, as well as laboratory tests to measure the levels of aldosterone and cortisol, as well as 17-OH progesterone, serum electrolytes, 17-ketosteroids or 17-hydroxycorticosteroids; x-ray exams to determine bone age.7
There are four syndromes related to CAH which are: adrenogenital syndrome, Cushing's syndrome, hyperaldosteronism, and feminization. The aim of the treatment is to normalize hormonal levels through the daily administration of cortisol: dexamethasone, fludrocortisone or hydrocortisone. During stressful periods additional doses of these drugs are required. It is not recommended to suddenly suspend steroid administration for fear of causing an adrenal failure.8
As part of the cosmetic- functional treatment, female patients with external masculine genitals may need corrective surgery between the first and the third month of life.9
Dental treatment requires the consent of the treating physician in order to administer prophylactic antibiotic treatment with Amoxicillin 50 mg one hour before the dental procedure; as well as a Prednisone dose adjustment. According to the protocol that states Prednisone doses should be increased in those patients who take less than 30 mg a day, if the dose administered falls under this amount, the human body is not prepared to manage a stressing situation, which in the dental office may cause an adrenal crisis. This can be avoided duplicating the normal dose before and after the dental procedure; subsequently the specialist may prescribe the regular dose. Treatment with antihypertensive drugs must not be interrupted.10
Objective
To document the oral and dental management of patients with Congenital Adrenal Hyperplasia.
To provide the knowledge for the dental care of this patient taking into consideration that dental procedures are stress factors and the dental clinician must be able to recognize and avoid an acute adrenal crisis.
CLINICAL CASE
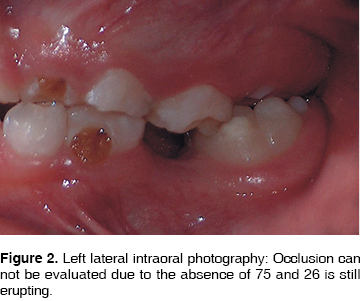
Six years and two months female patient diagnosed with Congenital Adrenal Hyperplasia salt-loss type. The patient was born and lives in Mexico City, and was sent to the Dental Pediatric Clinic by the Endocrinology Department of the HIMFG. At her admittance clinical and radiological examinations of oral cavity were performed. Clinical data were: poor oral hygiene, hydrated and vascularized soft tissues, moderate generalized gingivitis associated to dental plaque, adequate frenulums implantation, symmetric parabolic upper arch, horseshoe lower arch form, molar occlusion was not able to be evaluated due to the fact the permanent molars were erupting, absence of the a lower right molar could be observed (75), it had previously been removed in a private practice (Figures 1 and 2). There are fissures and restored interproximal cavities (Figures 3 and 4). In the X-ray of lower right second molar (85) a lesion in the furca could be observed.



When evaluating socioeconomic level and oral health of the parents they presented tooth decay and broken fillings and considering that caries is an infectious communicable disease, according to the Tinanoff criteria,12 the patient might be classified as a high risk for caries. Therefore, the same criteria were applied to manage caries, considering the child and the tooth decay, extension and location of the lesion, age of the patient, evaluation and re-evaluation of the activity of the lesion, results of previous therapies, natural history and caries progression, expectations and preferences of the parents and practitioners12 (Table I). Caries management was in agreement with high risk caries cases. This patient s natural history of caries shows carious lesions of multiple severity caused by an inadequate hygienical and feeding habits.

Consultation was carried out with the Endocrinology Service. The endocrinologist received a consultation sheet which included data on the patient: name, age, sex, and diagnosis. The sheet included information in the sense that the patient required invasive and extensive oral rehabilitation and for this reason it was necessary to increase her Prednisone dose before and after the dental procedure.
The objective of the treatment was in agreement with caries risk. This was preventive and restorative. Dental treatment was carried out in four sessions. Behavioral management was performed using the technique known as ''Tell-Show-Do'' and positive reinforcement.
Local anesthesia was applied: Lidocaine 2% with Epinephrine 1:100,000 UI as recommended pediatric dose by Dr. Malamed (4.4 mg/kg maximum dose); giving the patient a total amount of 36 mg per appointment. Oral rehabilitation consisted in restorations with stainless steel crowns on 55, 54, 53, 65, 64, 63, 74, 84 teeth, as well as the application of pit and fissure sealants on 36 and 46 teeth; tooth 85 was extracted.
A preventive hygienic program was developed; it consisted on the use of plaque disclosing tablets, regular tooth brushing with an appropriate brushing technique (Bass technique) after each meal, the use of dental floss, mouth rinses with clorhexidine 0.12% during 7 days the first week and then three days the first week of each month; topic fluoride application and periodical checkups every three months (Figures 5 and 6)


It is important to consider preferences and expectations of parents and operator: parents, with the advice of the dental professional, are the ones who must make decisions for their offspring s dental therapy; the dental professional is obliged to inform them about alternative therapies based on scientific evidence, results of risk assessment analysis, expected outcomes, and costs (Table II).

DISCUSSION
Salt-loss CAH refers to a group of inherited disorders of the adrenal glands, characterized by a deficiency of the hormones cortisol and aldosterone and an overproduction of androgen; it is an autosomal recessive disease. Female patients present sexual ambiguity and male patients a high virilization.8
The objective of the treatment is to normalize the hormonal levels through the daily administration of cortisol: dexamethasone, fludrocortisone, or hydrocortisone. During stress periods (surgery or serious disease) additional doses of these medications are needed to avoid an adrenal crisis.9
CONCLUSIONS
Congenital Adrenal Hyperplasia is a disease that requires important dental and oral considerations in order to offer a treatment: safe, adequate, comprehensive and focus enhancing the quality of life of the patient. It is important to follow an anti-stress protocol for those patients with cortisone-based treatments in order to prevent an adrenal reaction that might compromise the life of the patient.10
Age is the only characteristic to be taken into account when devising child management of caries.12
1. Natural history of caries: the earlier the child is colonized by the cariogenic group of bacteria, streptococcus mutans, the greater will be the caries risk. The permanent colonization of this group of bacteria occurs only after the eruption of the tooth, the colonization results from transmission of this organism from the supplier of primary care usually the mother. The teeth that are first exposed to a cariogenic environment are the first to show signs of the disease.12
2. History of therapy evidence: caries progression depends on the site of the lesion, the risk level and the activity of the lesion, as well as age of patient. The soft lesions on oral, lingual surfaces, even with cavities might be treated with preventive measures, meanwhile fissures or proximal lesions with caries may require restorative therapy to limit the progression. Caries activity may be evaluated through the observation of the progression speed of the existing lesions or for the incidence of new lesions.12
3. Caries risk evaluation: the goal of caries risk evaluation is to offer specific preventive or restorative care according to the individual needs of the patient. Previous experience of caries is still the best indicator of the future development of caries. It has been suggested that low weight at birth is an indicator of caries risk in primary teeth, due to its association with enamel hypoplasia and other defects in the enamel or indirectly for being a sign of family low socioeconomical level. Among other caries risk indicators are: the age of child colonization with cariogenic flora, streptococcus mutans level, based caries results, dental plaque evidence in upper anterior teeth and socio-demographic factors as education and income of the parents.12
4. Expectattions and preferences of parent and operator: the parent with the professional advice of the dental clinician is the one who must decide upon dental treatment. The dental clinician is obliged to inform about the alternative therapies based on scientific evidence, results of the caries risk evaluation, expectations and costs.12
Preventive therapy: the decision for preventive therapy is based on the understanding of risk indicators for the child.12
1. Fluoride: If the fluoride content is optimum or unknown, the drinking water may be analyzed to establish the amount of fluoride in it and if it is necessary prescribe to the patient systemic fluoride according to the fluoride water content and patient age. Fluoride supplements must be given to children in communities where the water is not fluoridated, as well as for children who are identified with a moderate or high caries risk and whose parents understand the risks and benefits of fluoride supplements. The most commonly used method for topic fluoride application is through dental paste twice daily. Fluoride products professionally applied or home care application must be recommended according to the present risk caries of the patient.12
Diet: Early caries has been related to a high frequency of sugar intake, including , be it through the use of feeding bottle or training glasses. For those individuals with a high risk of caries control of frequency of sugar intake might be an important element of the caries prevention program.12
Oral hygiene: The deficient oral hygiene contributes to the caries activity. The use of dental brush, mouth rinses, and professional dental cleaning are considered basic elements of caries prevention programs.12
Restorative therapy:
Caries progression
Lesions with cavities
Integrity tooth maintenance
At the end of the treatment
Evidence reaffirmation
Modification of the therapy
Clinical case
REFERENCES
 Mailing Address:
Mailing Address:
Vicente Cuairán Ruidíaz
Director del Departamento de Estomatología
Hospital Infantil de México ''Federico Gómez''
Tel. 55 98 72 59, 52 93 95 90 -93
Celular: 044 55 54 38 9900
E-mail: vicentecuairan@prodigy.net.mx
Note
This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
1. Andreoli TE, Barrett JC, Carpenter CCJ, Plum F. Compendio de Medicina Interna. 4a ed. México: Mc Graw-Hill, 1999: 150-236. [ Links ]
2. Burkart JM et al. Endocrinology. In: Brenner and rector's the kidney. 7th ed. BM Brenner (ed). Philadelphia, Saunders, 2004. [ Links ]
3. Eknoyan G, Shifer MJ. Endocrinologia and génetica. 2002; 346: 2010. [ Links ]
4. Forni LG, Hilton PJ. Current concepts: Endocrinologia and génetica. N Engl J Med 1997; 336: 1303. [ Links ]
5. Meyer. Endocrinologia. Crit Care Clin 2000; 16: 29. [ Links ]
6. Little JW, Falace DA, Millar CS, Rhodus. Tratamiento odontológico del paciente bajo tratamiento médico . 5ta. Harcourt/Mosby; España 2000: 245-251. [ Links ]
7. Díaz LM, Castellanos JL. Trastornos de la hemostasia inducidos por el empleo de medicamentos. Medicina Oral 1999; 4: 552-563. [ Links ]
8. Schiffl H, Swartz MD. Daily hemodialysis and the outcome of acute renal failure. N Engl J Med 2002; 346: 305. [ Links ]
9. Chandraker A et al. Transplantation immunobiology. In: Brenner and rector's the kidney. 7th ed. B Brenner (ed). Philadelphia, Saunders, 2004: 2759-84. [ Links ]
10. Limaye AP et al. Quantitation of BK virus load in serum for the diagnosis of BK virus-associated nephropathy in renal transplant recipients. J Infect Dis 2001; 183: 1669. [ Links ]
11. Pescovitz MD, Govani M. Sirolimus and mycophenolate mofetil endocrinologia. Am J Kidney Dis 2001; 38: S16. [ Links ]
12. Tinanoff N. Pediatric dentistry. Clinical decision making for caries management in children. 2002; 24 (5): 386-392. [ Links ]

