










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista odontológica mexicana
Print version ISSN 1870-199X
Rev. Odont. Mex vol.15 n.2 Ciudad de México Apr./Jun. 2011
Original research
Prevalence of early childhood caries and socioeconomical level
Delia Montero Canseco,* Patricia López Morales,§ Roberto Carlos Castrejón PérezII
* Graduated, Odontopediatrics Department.
§ Professor, Odontopediatrics Department.
II Department of Oral Public Health.
División de Estudios de Postgrado e Investigación (DEPeI) Facultad de Odontología; UNAM.
ABSTRACT
Early childhood caries (ECC) is a particular destructive form of caries that destroys dental structures of children during the first 3 years of life. Objective: To find out if there is an association between caries prevalence and socioeconomical level in children who attended the pediatric dental clinic at Universidad Nacional Autónoma de México (UNAM) during the school year 2006-2007. Material and methods: A transversal study was performed with a sample of 100 patients ranging from 12 to 48 months of age. An oral examination was carried out to determine the presence of caries. A questionnaire was applied to the parents to establish their socioeconomical level. Results: The prevalence of early childhood caries in the sample was 59.5%. A statistical significant difference by gender and age (χ2 = 43.27 p =0.001) was found. In relation to the average of teeth affected in children it was greater (2.8 ± 1.75) when the father had technical or professional studies (F = 4.5, p = 0.01). And also when the mother had studied junior high or high school (3.05 ± 2.69) (F = 3.9, p = 0.02). When children consumed 3 or more sodas or soft drinks daily, there was an increase in the number of teeth to be extracted (1.91 ± 2.06) (F = 3.3 p = 0.03) that also occur when children ate candies during twice the day (2.09 ± 2.07) (F = 4.6 p = 0.12). Conclusions: The prevalence of ECC was high, and the educational level of the parents and dietary habits of the children were directly related to the presence of tooth decay of the surveyed underage patients.
Key words: Tooth decay, socioeconomic level, early childhood caries.
INTRODUCTION
Dental caries is considered a public health problem in developing countries like Mexico, where there is a lack of prevention programs. Therefore low income communities present a high prevalence of caries.1
Dental caries is an infecto-contagious disease characterized for the destruction of dental hard tissue and caused by the action of the acids produced by microorganisms that form dental plaque.2 One of the worst types of this infection is the one that affects children in early childhood. Malnutrition practices can initiate progressive dental caries of the buccal and lingual surfaces of maxillary and mandibular deciduous teeth in newborn and pre-school children.3
American Academy of Dental Pediatrics4 (AADP) guidelines has defined Early Childhood Caries (ECC) as:
"Early childhood caries is the presence of one or more carious surfaces (with or without cavity), lost surfaces (due to caries) or filled surfaces in any deciduous tooth of a child ranging between birth and 71 months of age"
ECC is similar to other forms of dental caries in older children with the characteristic that this disease develops fast from a white spot or decalcification to a cavity.5
Lopez del Valle et al.6 reported that in 1995 Duperon during a workshop sponsored by Centre of Control Disease and Prevention (USA) suggested "Early Childhood Caries" (ECC) as the most appropriate concept to describe the disease. Ismail7 in 1999 suggested that ECC should be defined as:
"The presence of any sign of dental caries in any surface during the first 3 years of life"
From a microbiological point of view, the development of ECC can be divided into three stages:8
1. Primary infection by S. mutans .
2. Accumulation of pathogen microorganisms ( S. sobrinus and Lactobacillus ) because of prolonged exposition to cariogenic substrates.
3. Fast enamel demineralization and formation of cavities in dental structure.
The main etiological factor of ECC is S. mutans that when in conjunction with S. sobrinus , becomes more acidogenic and aggressive than mutans and lactobacillus groups.
Berkowitz9 mentions that in children with ECC, S. mutans levels exceed 30% of the cultivable plaque flore, whereas, in children with low cariogenic activity the levels pertain to 0.1%.
The concept of early childhood caries has changed during the years. In the following list we provide synonyms10 still in use:
• Bottle caries
• Bottle syndrome
• Breast feeding dental caries
• Infant feeding syndrome
• Rampant infant caries
Primary risk factors11,12 to early childhood caries are:
• Feed the newborn at nap or nighttime with bottles containing liquids additioned with some kind of sweetener.
• Allow breast feeding during the night.
• Continue bottle feeding after the first year of life.
• Lack of dental hygiene practice performed by adults.
• Socioeconomical factors.
Several authors7,12,13 have classified early childhood caries in stages. Each stage has been characterized for the degree of destruction, for the site of destruction and according to the age of the child, the number of teeth affected and the severity of the lesions.
Few studies have been published in Latin America about ECC. PAHO5 in 2004 organized a meeting with 23 Oral Health Head Officials in La Habana, Cuba. Only 6 of the attending countries have researched on ECC. Prevalence reports are as follows: Nicaragua 81%, Bahamas 58%, Honduras 60% in children under 6 years of life; Chile 85%, Ecuador 13.2% and Colombia 60% in pre-school children.
Zimbron14 in 2000 reported that 95% of Mexican children under 6 years of age suffered from dental caries. Velazquez et al.15 in 1995 carried out a study in Mexican children ranging from 6 to 10 years, finding a 95% caries prevalence in deciduous teeth.
MATERIAL AND METHODS
A transversal study included a sample of 100 patients ranging from 12 to 48 months of age attending for the first time the Pediatric Dental Clinic, of Division de Estudios de Postgrado e Investigación (DEPeI) FO, UNAM during the school year 2006-2007.
The study variables were: caries presence in early childhood, teeth to be extracted, primary teeth, socio economical level and infant nutrition.
Socio economical level is defined as: the social, economic and cultural conditions of an average individual of a certain group or nation.16
The socio economical level information was obtained through a questionnaire applied to parents, previous to an Informed Consent. To assess the social economical level the guidelines of the Department of Social Work of the Hospital Infantil de Mexico "Federico Gómez" were used (father occupation, mother occupation, educational level of parents, type of housing and child nutrition including candies and soft drinks intake).
The intraoral examination was done by a second year student of pediatric dentistry course, who was previously trained to diagnose caries and teeth to be extracted (Kappa test 0.80).
To register in the index the caries and teeth to be extracted WHO criteria were utilized.17 These criteria state that a dental surface is classified as carious when there is softening of the floor or walls of the surface being examined. The latter implies that incipient carious lesions in the white spot stage are not considered carious the same as those remineralized lesions that although pigmented presented hard surfaces. Following WHO guidelines a tooth to be extracted is the one where the crown has been destroyed and can not be restored, or when caries had progressed much that pulpar exposition is obvious and dental rehabilitation is not possible, or when there are only root fragments. The number of deciduous teeth was also accounted as follows:

The statistical analysis of the data was done through central tendency measurements (average and standard deviation), measurements to compare percentages (χ2 test) and variance analysis (ANOVA) to determine if there were statistically significant difference between the values obtained by the presence of caries, teeth to be extracted and the age, sex and socio economical level.
RESULTS
A 100 patients were examined, 58 boys (58%) and 42 girls (42%) ranging from 14 to 48 months of age with a media of 34.6 ± 8.3 months. Three age groups were formed randomly mixed. In the first one there were children from 14 to 24 months, in the second 25 to 35 months and in the third one from 36 to 48 months of age.
In relation to the deciduous teeth distribution by age, it was observed that 57.6% of the deciduous teeth were present in the interval ranging from 36 to 48 months. It was observed that 49.8% belonged to boys and 68% belonged to girls. There was a statistically significant difference in the percentage of deciduous teeth in boys and in girls (χ2 = 50.94 p = 0.001) and (χ2 = 43.27 p = 0.001), respectively (Table I).
Comparing the prevalence for gender and age, the girls group 36 to 48 months showed the greatest prevalence of ECC (70.0%), in boys the same age prevalence was 52%. This agrees with the prevalence of the groups by age in general where prevalence of boys 36 to 48 months was 59.5%. A statistically significant difference was observed in relation of the distribution of the percentage of deciduous carious teeth by age in boys and girls (χ2 = 47.38, p = 0.012) and (χ2 = 36.63, p = 0.013) respectively (Table II).
In relation to educational level of parents, it was concluded that the average of teeth affected by ECC was greater among the children when the father had technical or professional studies (2.8 ± 1.75) comparing to those that had finished the elemental school (2.0 ± 2.0). A statistically significant difference was observed according the average number of teeth affected by ECC and educational level of parents (F = 4.5, p = 0.01). When Tukey's test was carried out, the difference between the group of parents with junior high and high school and the group of parents with technical and professional studies (p = 0.009) was found. In relation to maternal educational level, it was observed that the average of teeth affected by ECC was greater between children whose mothers had junior high school or high school studies (3.05 ± 2.6) than in those whose mothers who only had finished elementary school (1.3 ± 1.8). A statistically significant difference was observed in relation to the average of teeth affected by ECC and mother's educational level (F = 3.9 p = 0.02). When Tukey's test was carried out, the difference was found between the group of mothers with elemental school and the group of those with junior high and high school (p = 0.049) (Table III).
In relation to parents' occupation it was concluded that the number of teeth affected by ECC was greater for children when the mother was a housewife (9.2 ± 3.5) compared to the group whose mothers had a technical occupation (4.6 ± 1.1). In relation to fathers, it was observed that the average was greater when they were labourer (11 ± 2.8), compared to the group where the fathers were merchants (7.5 ± 3.6). There were no statistically significant differences in relation with the number of carious teeth between the father and the mother occupation (F = 1.18 p = 0.325) and (F = 0.619 p = 0.325), respectively (Table IV).
In relation to children diet, the average of teeth to be extracted was higher (1.91 ± 2.06), that those who did not intake soft drinks (0.50 ± 1.16), a statistically significant difference was noted (F = 3.3 p = 0.03). When the Tukey's test was carried out, it was found that between the group of children that did not consume soft drinks compared to the group of children that consumed three or more soft drinks (p = 0.040), meanwhile, in the case of candies, the group of children that consumed two or three candies daily, the number of extractions was greater (2.09 ± 2.07) in comparison to those that only consumed one (0.64 ± 1.20). Although it must be noted that in relation to candies consumption there was not statistically significant difference (F = 4.6 p = 0.12) (Table V).
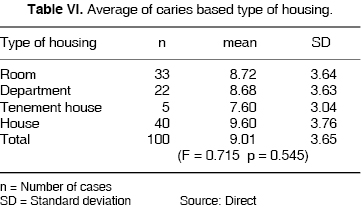
The results in relation to the kind of housing showed that the average of teeth affected ECC was greater (9.6 ± 3.76) among the children who lived in a house in comparison to those that lived in a tenement house (7.60 ± 3.04). However, there were not statistically significant differences by the housing type (F = 0.715, p = 0.545) (Table VI).
DISCUSSION
The dental caries prevalence in the Mexican children population examined was 59.5%, however comparing it with the percentages found in studies made in Mexico by Zimbron14 (95%), Velazquez et al.15 (96%) was smaller. The differences can be attributed to:
• To diverse sizes of the samples.
• Operational definition of dental caries.
• If deciduous or permanent dentition were considered united or separated.
• Age of children.
• Presence of mixed dentition.
• Number of examiners.
In this research the filled and recurrent carious teeth were not considered since all patients were attending dental treatment for the first time, therefore caries prevalence could vary compared to previous researches.
On the other hand, diagnostic criteria for the three studies were the same and the survey takers who participated in both studies did it under WHO guidelines.17
Other common aspects of the three studies, was the great destruction found in deciduous dentition. Probably due to the fact that it is considered temporary and it is not a priority.
This concept is limited if we consider consequences of dental caries in pre-school children. These consequences can be pain associated with infectious processes, disruption caused by loss of space due early to extraction of deciduous teeth, difficulties in chewing properly, adoption of negative oral habits, and possible association between high caries prevalence in deciduous dentition, which in turn extrapolates to the permanent dentition.
When compared to studies carried out in Latin America, caries prevalence in the examined Mexican sample, is in agreement with countries such as: Bahamas (58%), Honduras (60%) Colombia (60%). In all studies, participant's age was under 71 months.5,8
Scarcity of national information on the subjects reflects on the limited number of published studies.14, 15 In some cases it has been decided not to carry out rigorous statistical sampling, following instead studies based on convenience sampling.
Results obtained in this study cannot be inferred for children's population, they should be taken as first results of a basic information. It is suggested to include in further research papers additional socioeconomical aspects so as to improve instruments geared to obtain information on the relationship between early childhood caries and the family socioeconomical level. The sample should be formed with same number of both genders in the same age interval. Also to be considered is the Oral Hygiene index and previously treated patients. Whenever possible it is advised to include a caries free sample group.
CONCLUSIONS
• Prevalence of early childhood caries in examined Mexican population was high (59.5%).
• A relationship was found between early childhood caries and the socioeconomical family level, which in turn was related to the scholar level of the parents.
• In the children's diet, soft drink intake was associated to the average of deciduous teeth which needed extraction.
REFERENCES
 Address correspondence:
Address correspondence:
Delia Montero Canseco MD
Galicia Núm. 24,
Col. Álamos, 03400,
Del Benito Juárez,
Phone. 55 30 39 04
Cell phone. 04455 37273209
E-mail: demont_808@hotmail.com
Note
This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam
1. Gavito HF, Magaña BV, Fragoso RR. Índice de caries y su relación con el estrato socioeconómico. Dentista y Paciente 1998; 8(2): 32-40. [ Links ]
2. Stephen M. Caries de la infancia temprana. FDI 1998; 7(4): 16-20. [ Links ]
3. Barberia LE, Boj QR. Odontopediatría . Editorial Masson. 2da. edición. Barcelona, España. 2002: 181-183. [ Links ]
4. American Academy of Pediatric Dentistry (AAPD). Oral Health Polices and Clinical Guidelines. Pediatric Dentistry 2003: 25 (Suppl. 7). [ Links ]
5. Milgrom P, Weinstein P. Caries de la niñez temprana: Una perspectiva multidisciplinaria para prevención y tratamiento de la condición . Universidad de Washington, Seattle, WA. Panamericana Formas e Impresos S.A. Colombia, 2006. [ Links ]
6. López VLM, Gudiño FS, Machuca-Portillo MC. México; Centro Sudamérica y el Caribe latino: Perspectiva actual de la condición de la caries de la niñez temprana en la región. En: Milgrom P, Weinstein P: Caries de la niñez temprana: una perspectiva multidisciplinaria para prevención y tratamiento de la condición . Universidad de Washington, Seatlle, WA. Panamericana Formas e Impresos S.A. Colombia, 2006 [ Links ]
7. Ismail AL, Sohn W. A systematic review of clinical diagnostic criteria of Early Childhood Caries. J Public Health Dent Summer 1999; 59(3): 171-91. [ Links ]
8. Nelson FP. Caries del biberón Capítulo 11. En: Léa Assed B. Tratado de Odontopediatría . Editorial Amolca. Tomo 1, Colombia, 2008. [ Links ]
9. Berkowitz JR. Causes, treatment and prevention of early childhood caries: a microbiologic perspective. J Can Dent Assoc 2003; 69(5): 304-7. [ Links ]
10. Amid I, Ismail B, Determinants of health in children and the problem of early childhood caries. Pediatric Dentistry 2003; 25(4): 328-333. [ Links ]
11. Noelle LH, Joon K, Christopher VH. Caries-risk factors for hispanic children affected by early childhood caries. Pediatric Dentistry 2002; 24(6): 536-542. [ Links ]
12. Hubertus JM, Van W, Stöckli. Odontología Pediátrica . Editorial Masson. Barcelona, España. 2002. [ Links ]
13. Wyne AH. Early childhood caries: nomenclature and case definition. Dent Oral Epidemiol 1999; 27: 313-5. [ Links ]
14. Zimbrón LA. Experiencias en la Facultad de Odontología de la UNAM, Universidad Nacional Autónoma de México. Las Universidades y la meta de la salud para todos en el año 2000. Conferencia presentada en la Reunión de Rectores de Universidades y Directores de Escuelas y Facultades del Área de la Salud, México. 9 al 11 de abril 1984: 399-412. [ Links ]
15. Velázquez MO, Vera HH, Irigoyen CEI, Mejía GA, Sánchez PTL. Rev Panam Salud Pública/Pan Am J Public Health 2003; 13(5): 320-326.
16. Diccionario Enciclopédico Ilustrado Danae. Grupo Editorial Océano S.A. Barcelona, España. 1993. [ Links ]
17. OMS World Health Organization: Oral Health Surveys. Basic Methods, ed 3. Geneva, WHO 1987. [ Links ]

