











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction1
Ever since the beginning of the previous century, various studies have shown a negative correlation between unemployment and the mental health of the unemployed. For immigrants, however, there are indications that the relation between unemployment and mental health could be different than among the general population. Furthermore, a correlation does not imply that unemployment is the reason of mental health problems. This paper investigates the impact of unemployment on the mental health of Mexican immigrants and other Latin Americans, comparing them with the native non-Hispanic white and African-American population, analyzing more or less homogeneous population groups with diverse economic, social, and cultural backgrounds.
Factors such as economic restructuring and the labor market have been shown to contribute to increase unemployment among certain ethnic groups (Wilson, 1991). Recent studies show that in times of economic crises, the difference between the unemployment rates of white natives and Latin American groups widens (Kochhar, Espinoza, and Hinze-Pifer, 2010). For example, in 2006 the unemployment rate for non-Hispanic white natives was 4.1 %, whereas for Mexican immigrants it was 4.8 %. In 2010, the rate for the former increased to 8.7 % and to 12.4 % for the latter, whereas the rate for African-Americans went from 9.9 to 17.1 %. Also, health in general and mental health in particular differ between population groups, although the relation is not straightforward, evidenced by what is known as the Hispanic health paradox: It is frequently observed that Hispanics report better health than non-Hispanic white natives despite their generally less favorable economic and social situation (Markides and Coreil, 1986). There is evidence that unemployment is one of the causes of mental health problems (Paul and Moser, 2009), but migration complicates relations between labor, economic restructuring, and mental health.
Our hypothesis is that unemployment has a negative impact on a person’s mental health, and that this effect is stronger in economically and socially more vulnerable population groups, in particular Mexican immigrants and-to a lesser extent-other Latin Americans and Afro-Americans, than for non-Hispanic native whites. To test this we estimate probit models with instrumental variables, on the basis of information from the 1999 and 2009 National Health Interview Surveys (NHIS). The analysis aims to compare people according to their ethnicity and place of birth2, dividing them into five groups: Mexican immigrants; Mexican-Americans (individuals born in the United States defining themselves as of Mexican origin); other Hispanics (including Puerto Ricans and Latin Americans from countries other than Mexico, either immigrants or U.S.-born); African-Americans born in the United States, and the native non-Hispanic white population. The years of study have been chosen as they coincide with periods of economic stability (1999) and crisis (2009).
This introduction is followed by a section with a brief back ground on unemployment and mental health in the United States. The third section describes the data being used, and the fourth explains the econometric framework. The fifth section presents the results of the analysis, and the sixth and final section discusses the outcomes and poses some conclusions.
Unemployment and Mental Health: A Background
In the United States, minorities such as African-Americans and Mexican immigrants have historically been more affected by unemployment than the non-Hispanic white natives (Caicedo, 2010). Differences in unemployment rates between native whites and African-Americans have been the subject of several studies performed from various theoretical perspectives (human capital, economic restructuring, social networks; e.g., Stratton, 1993; Browne, 1997; Fairlie and Sundstrom, 1999; Granovetter, 1995). The results can be employed to explain the differences observed between the rates for natives and Latin Americans, although Castells (1998) argues that a different situation is experienced by Latin American immigrants, whose family structures are stronger and whose social networks provide them with important support regarding labor information and references, a factor that makes it easier for them to get a job (Granovetter, 2005). Granovetter (1995:133) argues that African-Americans are at a disadvantage when it comes to using these informal channels of job information, as they are underrepresented in the employment structure itself; the more nonblack friends African-Americans have, the easier their labor integration becomes. In the case of the Hispanic population, Borjas and Tienda (1985) claim that discrimination is one of the factors explaining their higher unemployment rates, although Wilson (1998) argues that for African-Americans, racism is not a direct explanation for their high level of unemployment, but that it is also linked to the transformations in the productive structures of cities: The demand for lower-qualified workers has dropped, and since African-Americans are significantly less qualified than white citizens, unemployment hits them harder.
The so-called Hispanic health paradox has been reported for several diseases and also for mortality. While typically socioeconomically disadvantaged, Hispanics often report better health than non-Hispanic whites in the United States (Markides and Coreil, 1986; Martinez, Aguayo-Tellez, and Rangel-Gonzalez, 2015; Fuller Thomson et al., 2013). Whereas many ethnographic studies find that the Mexican-origin population presents psychiatric problems at levels similar to those observed in the non-Hispanic white natives (Vega et al., 1984), Alegría et al. (2008) found that psychiatric disorders are less frequent among those who have Latin American origins but were born in the United States than among non-Hispanic natives, and that immigrants report lower rates of psychiatric disorders than U.S.born-Hispanics, suggesting that the Hispanic health paradox may also apply with respect to mental health. Studies have shown that the population with Mexican-origins presents lower rates of admission in hospitals specializing in mental health (Vega and Rumbaut, 1991; Carrasquillo, Carrasquillo, and Shea, 2000; Guarnaccia, Martínez, and Acosta, 2005). These results have raised discussions on whether the lower number of Mexican-Americans admitted to these hospitals is due to a lower occurrence of mental disorders or to a lower number of individuals making use of this type of services. It has been pointed out that Mexican culture somehow helps muffle the effects of stress factors on individuals, and that it is also more tolerant of abnormal behavior a member of the family might show (Vega and Rumbaut, 1991). Others find that one of the factors that stop Hispanic immigrants from reporting mental health problems and seeking professional help to solve them is the great limitation involved in trying to communicate in the English language (Carrasquillo, Carrasquillo, and Shea, 2000; Ku and Waidmann, 2003; Guarnaccia, Martínez, and Acosta, 2005; DuBard and Gizlice, 2008). Grant et al. (2004) point out that the lower rates of mental disease among Mexican immigrants compared with Mexican-Americans and non-Hispanic white natives are due to a selection effect of emigration; that is, individuals with good physical and mental health are more likely to migrate to the United States. Also, the migratory process itself as well as the subsequent social and cultural adaptation of the immigrant to the receiving society play a very important role in their mental health (Portes and Rumbaut, 1994; Bhugra and Jones, 2001). Vega, Kolody, and Valle (1987) add socio-demographic characteristics to this list, such as low level of education, low income, unemployment, marriage breakups and being undocumented. More generally, discrimination also has been identified as a factor negatively affecting mental health (Pascoe and Richman, 2009).
Studies performed around the world in the areas of psychiatry, social psychology, and sociology illustrate that unemployment can deteriorate workers’ mental health. Contemporary research leads to the conclusion that unemployed individuals show lower levels of psychological well-being, a higher level or anxiety and depressed feelings, and a lower level of self-esteem and life satisfaction (Garrido, 2009; Mossakowski, 2009; Kennedy and Mc Donald, 2006).
Del Pozo et al. (2002) argue that when individuals lose their jobs, there is a fast deterioration of their mental health due to the absence of “psychosocial contributions,” the impossibility of predicting and planning for the future and the loss of a valued social position. The authors show that the longer the unemployment condition extends, the stronger the mental health deterioration. Moreover, high unemployment levels have even been related to high suicide rates (Milner, Page, and La Montagne, 2013). Schaufeli (1992) points out that the relation between un employment and mental health is not direct but, on the contrary, is mediated by the individual’s personal characteristics, such as a high level of self-esteem and a low level of neuroticism or mental instability. The ILO (2000) claims that in today’s context of economic restructuring, where in addition to unemployment a noticeable deterioration of labor conditions is observed, mental illnesses are more present than ever among workers. Thapa and Hauff (2005) have found a strong link between the lack of paid work and psychological anguish among immigrants in particular. In a meta-analysis, Paul and Moser (2009) compare results concerning the effect of unemployment on mental health in more than 300 cross-sectional and longitudinal studies. Their conclusion is that there is overwhelming evidence that unemployment increases psychological problems, and that this is a causal effect. The relation between mental health and unemployment is not necessarily due to unemployment causing mental disorders, as mental problems may also result in job loss. For example, Ettner, Frank, and Kessler (1997) find that psychiatric disorders reduce the probability of being employed, while Nelson and Kim (2011) identify that a mental illness increases the hazard of job termination. In the analysis we account for this possibility of bidirectional causality.
Considering that we compare an economic boom with a crisis year, the findings reported by Dávalos and French (2011) are relevant; they conclude that economic downturns have a negative impact on the health-related quality of life (HRQL) indicator, a measure that goes beyond the incidence of illnesses but that refers to the perceived physical and mental health. The mental HRQL measure particularly worsens during economic downturns. Similar effects of economic downturns on mental health are reported by Ruhm (2000; 2003), while for several other (physical) diseases he finds a counter-cyclical relation, i.e., their incidence is lower during downturns. Charles and De Cicca (2008) show that worsening (local) labor market conditions lower mental health status, especially among African-Americans and less-educated males.
Data
The National Health Interview Survey (NHIS; IHIS, 2012) gathers information on the non-institutionalized civil population of the United States. Every year, approximately 35,000 households (85,000 people) are interviewed, but even though samples are taken from all states, the survey is representative only at the national level. The African-American and Hispanic parts of the population are overrepresented in the sample. The survey does not allow the distinction between documented and undocumented immigrants (NHIS, 2012). In every household one adult (18 years and over) is selected to complete a set of questions on health conditions, health-care services use and health-related behaviors. For the years 1999 and 2009 we selected adults between 18 and 65 years of age who were part of the labor force and who answered questions about their mental health.
Unemployment in 1999 and 2009
Regarding unemployment rates, between 1999 and 2009 there was a large increase in unemployment levels for all groups, but with certain differences among them. In 1999, the United States was in a time of economic stability, whereas the country had a long struggle to overcome the financial crisis that hit in 2008. During 1999, the unemployment rate among non-Hispanic white natives was 2.1 %, and in 2009 the rate was 7.7 % (Table 1). Among African-Americans, unemployment rates were double those of the non-Hispanic white natives both in 1999 and 2009. In 1999 African-Americans had a 5.3 % rate; this number was 15 % in 2009. Over this 10year period the unemployment rates among Latin Americans also tripled; rates for immigrants from Mexico went from 3.4 % in 1999 to 11.4 % in 2009, whereas the rate for Mexican-Americans went from 4.2 to 12.1 % and for other Hispanics from 4.1 to 12.2 %, though there is no significant difference between these three groups (Table 1). While non-Hispanic whites’ unemployment remained at the lowest absolute level, the group also experienced the proportionally largest growth in joblessness.
Table 1 Unemployment rates by ethnicity and year, 1999-2009
Source: Own calculations on the basis of the NHIS, 1999 and 2009 (IHIS, 2012).
(a) “Other Hispanics” includes Puerto Ricans.
(b) p-values of F-tests; testing in each ethnic group if the unemployment rates in 1999 and 2009 are the same (last column), respectively. In each year, if the unemployment rates are the same in all ethnic groups (last two rows, the last row only with the three Hispanic groups).
Health Condition
In the NHIS, an effort is made to identify individuals’ risk of suffering mental problems. The survey includes six questions on the basis of which a risk of Non Specific Psychological Disorder indicator is built using the Kessler 6 scale (Kessler et al., 2002). This is a measurement tool originally designed by Kessler and Mroczek (1994) that consists of ten questions on the basis of which symptoms associated with depression and anxiety can be identified. Kessler et al. (2003), however, demonstrate that the scale based on the six questions included in the NHIS is as effective to detect mental health disorders as the one based on 10 questions. With the Kessler 6 scale the risk of suffering from a psychological dis order can be identified, but it is not possible to determine whether the disorder is depression or anxiety.
The following questions were put to a sample of adults 18 or older: “During the past 30 days, how often did you feel (1) that everything was an effort, (2) hopeless, (3) nervous, (4) restless or fidgety, (5) so sad that nothing could cheer you up, and (6) worthless.” The possible answers are: “(0) None of the time, (1) A little of the time, (2) Some of the time, (3) Most of the time, and (4) All of the time.” Assigning scores 0-4 to the answers and adding up the six indicators gives a scale that moves between the values 0 and 24. Individuals with values of 13 or more points have a high risk of experiencing severe non-specific psychological disorders (Kessler et al., 2003:188)3.
Table 2 presents the percentages of people with severe non-specific psychological disorders, using the above-mentioned definition. In 1999, the percentage of non-Hispanic white natives with mental disorders in the sample was 1.6 %, and in 2009 it went up to 2.1 %. Among those with a Mexican background we see reductions of the incidence of mental disorders, though the differences between 1999 and 2009 are not statistically significant. On the other hand, we see a very slight increase among other Hispanics, which results in a significant difference between the three His panics groups in 2009 despite the absence of a difference in 1999 (Table 2, last row).
Table 2 Severe mental health condition according to Kessler-6 scale (%), 1999 and 2009
Source: Own calculations on the basis of NHIS, 1999 and 2009 (IHIS, 2012).
The data seem to confirm the Hispanic health paradox dis cussed in section 1 for Mexican immigrants in 2009 but not in 1999, and neither for Mexicans born in the United States or the other Hispanics; despite a generally weaker socio-economic situation, reflected also by the high unemployment rates, mental health problems among Mexican immigrants are lower than among non-Hispanics. The information provided in Table 2, however, does not generally confirm that the numbers for mental health would increase parallel to the rise in unemployment. In particular, for Mexicans, we find a (small and statistically insignificant) decrease in the prevalence of severe mental health problems. Nevertheless, this does not imply that there is no causal relation for Mexicans; it could exist but be broken due to other characteristics.
Empirical Framework
In this section we perform an econometric analysis that seeks to demonstrate whether unemployment can be considered a causal factor of the prevalence of serious mental health disorders. The instrumental variable technique that is applied, discussed in the next subsection, permits establishing causal relationships in the absence of longitudinal data.
Econometric Framework
For this analysis we use the dichotomous measure for the individual incidence of serious mental health disorders based on the Kessler-6 screening scale of non-specific psychological distress as presented in Table 2. Our main explanatory variable is the individuals’ unemployment status. However, this is a potentially endogenous variable; it could be that someone became unemployed after suffering from a mental illness. As indicated in the literature review, it is not clear whether individuals reported mental health problems due to losing their jobs or whether they became unemployed because they experienced a mental health problem.
In order to identify a causal relation between mental health and unemployment, it is necessary to take into account the-potential-endogeneity of unemployment. In non-longitudinal non-experimental data like such as we deal with here, using instrumental variables (IV) is an approved technique to accomplish this. Given that we use a dichotomous indicator for mental health, and taking into account the equally dichotomous nature of unemployment, the IV approach leads us to the application of a bivariate probit model (Wooldridge, 2010:594-599). Just as with the more common linear IV models, such as two-stage least squares (2SLS), instruments must have a strong relationship with the endogenous explanatory variable, whereas they should not have a direct effect on the variable of interest. In our case, that means we need variables that have a strong relation with the individual’s unemployment but that have no direct effect on their mental health status (other than through the unemployment status).
In short, the model establishes two (probit) equations: one for mental health (MHi*) and one for unemployment (UNi*), where unemployment is also included in the equation for mental health as an explanatory variable:
 (1)
(1)
 (2)
(2)
where MHi* and UNi* are unobserved latent variables, the- continuous-counterparts of the observed variables, mental health MHi, and the unemployed status UNi, respectively. The observed variable MHi is equal to 1 if MHi*>0 and equal to zero in the opposite case; the observed variable, unemployment UNi, is equal to 1 if UNi*>0 and equal to zero otherwise. The vector of exogenous variables included in both equations is Xi, whereas vector Zi contains the instrumental variables giving account of the endogeneity of unemployment that are only included in the unemployment equation. The model’s equations are estimated jointly, allowing for a correlation between error terms ui and vi. Parameter λ measures the causal effect of unemployment on the prevalence of severe mental disorder, if we can assure that the instruments included in Zi adequately account for the endogeneity problem. In fact, with valid instruments, we can test whether or not endogeneity is an issue that requires correction; if we can reject an endogeneity problem, a simple single probit model formed by equation (1) only instead of a bivariate probit model (equations 1 and 2) is more efficient and should be preferred. The subsection “Endogeneity of Unemployment” addresses this.
Other Explanatory Variables
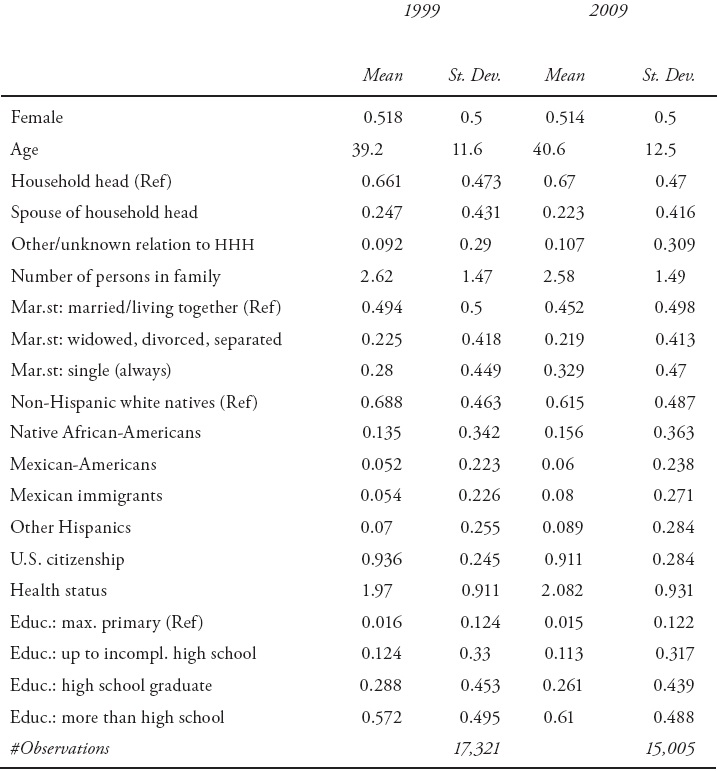
Table 3 shows the descriptive statistics of the other variables (Xi) that are used in the explanation of mental health problems, in addition to the unemployment status. The sample of observations used in the model for 1999 contained slightly more women than the sample for 2009, 51.8 % versus 51.4 %, while the sample in 2009 was slightly older, 39.2 in 1999 versus 40.6 years. The family size was virtually equal in the two years, but in 2009 fewer people reported to being married (49.4 % in 1999 versus 45.2 %). The number of people who reported to being the head of house hold has increased from 66.1 % in 1999 to 67 %, mainly at the expense of spouses of households heads (a reduction from 24.7 % in 1999 to 22.3 %). The number of non-Hispanic white natives in the sample has decreased from 68.8 % in 1999 to 61.5 %, compensated by increases in each one of the other groups (note that this does not mean that the share of “non-whites” in the population has grown, because we did not use the sample weights). The share of people with more than a high school education was larger in 2009 than in 1999 (61 % versus 57.2 %), while the self-assessed health in 2009 was marginally better than in 1999, although for both years we can say that the average respondent was in good health.
Table 3 Explanatory variables, 1999 and 2009
Source: Own calculations on the basis of NHIS, 1999 and 2009 (IHIS, 2012).
Endogeneity of Unemployment
We briefly discuss our instruments and the conclusions regarding the issue of the potential endogeneity of unemployment in the explanation of mental health problems. We performed instrumental variable (IV) analysis with different sets of instruments in linear probability models. As said, we need variables that explain the unemployment status of individuals but that are not directly related with mental health problems. Usually, regional or macro variables such as the regional unemployment rate are considered good candidates. A high unemployment rate in the region of residence is likely to increase the probability that a sampled respondent is unemployed, while there is no reason to expect that there is a strong direct effect on individual mental health problems other than through the individual’s unemployment. Furthermore, not less important, the impact of the individual’s unemployment and mental health status on the regional unemployment rate is small. Hence, the regional unemployment is exogenous and qualifies as an instrumental variable (although recent studies such as Behanova et al. (2013) and Walsh et al. (2013) find indications that urban unemployment rates and neighborhood-level socioeconomic status may have a direct effect on mental health).
We construct regional unemployment rates for the four regions that we can distinguish in the data, while we allow for variation by ethnic group (whites, African-Americans, and His panics) and by level of education (primary, incomplete high school, completed high school, and more than high school). The rates are calculated within the data by averaging the observed unemployment in each of the relevant groups; in order to assure exogeneity, for the calculation of the average unemployment rate for a specific respondent we exclude that respondent from the calculation.
Hence, only the other observations with the same characteristics (region, ethnicity, education) are used for the calculations for each individual; the respondent does not enter the calculation of the value that applies to him/her. The first row of Table 4 shows the descriptive statistics of this variable, while Table 5 presents the test results for this instrument in a 2SLS (linear probability) model. The tests indicate that the instrument explains the individual unemployment status, although for 2009 the identification is not very strong. The endogeneity tests suggest that there is no endogeneity problem; the null hypothesis of the exogeneity of unemployment is not rejected. An additional indication of the absence of an endogeneity problem is provided by the estimation of the correlation ρ between the error terms ui and vi in equations (1) and (2). The last row in Table 5 reports the estimations of ρ in each of the models. In none of the estimations there is an indication that the error term of the explanation of mental health and unemployment are correlated.
Table 4 Instrumental variables, descriptive statistics, 1999 and 2009
Source: Own calculations on the basis of the NHIS, 1999 and 2009 (IHIS, 2012).
Table 5 Indicative tests of the validity of the instrumental variable: regional unemployment (a)

Source: Own calculations on the basis of the NHIS, 1999 and 2009 (IHIS, 2012).
(a) Tests performed in the linear probability instrumental variable model, where more tests are available than in the dichotomous models for instrumental variables. An over-identification is not reported because the model is exactly identified.
(b) Stock-Yogo critical value for 10 % maximal IV size: 16.38, 15 % maximal IV size 8.96.
In order to give more evidence of the validity of our conclusion regarding the validity of the instruments and the absence of an endogeneity problem, we performed additional analyses with more instruments. With more than one instrument, also an over-identification test also can be performed, that is, whether the instruments can be excluded from the mental health equation. In Table 6 we add an indicator whether the respondent talked to or saw an eye doctor during the previous 12 months. The identification improves, although in 2009 it remains weak. The over-identification tests do not provide any evidence that one or more of the proposed instruments should be in the main equation. Again, the endogeneity tests do not reject the exogeneity of the individual employment, a conclusion that can be drawn more convincingly now given that the validity of the instruments has been accredited better. Adding the language of the interview, English versus (a combination with) Spanish, as an additional instrument leads to the same conclusion.
Table 6 Indicative tests of the validity of the instrumental variables: Regional unemployment, talked to/saw an eye doctor (a)

Source: Own calculations on the basis of the NHIS, 1999 and 2009 (IHIS, 2012).
(a) Tests performed in the linear probability instrumental variable model, where more tests are available than in the dichotomous models for instrumental variables.
(b) Stock-Yogo critical value for 10 % maximal IV size: 19.93, 15 % maximal IV size 11.59.
Hence, we conclude that our instruments are valid, and with these instruments we do not find an indication that we have a problem with endogeneity. In other words, we conclude that the occurrence of unemployment is not the result of a serious mental health problem. The implication of this finding is that the simple probit model formed by equation (1) gives a causal explanation of the effect of unemployment on mental health problems.
Results: The Effect of Unemployment on the Workers’ Mental Health
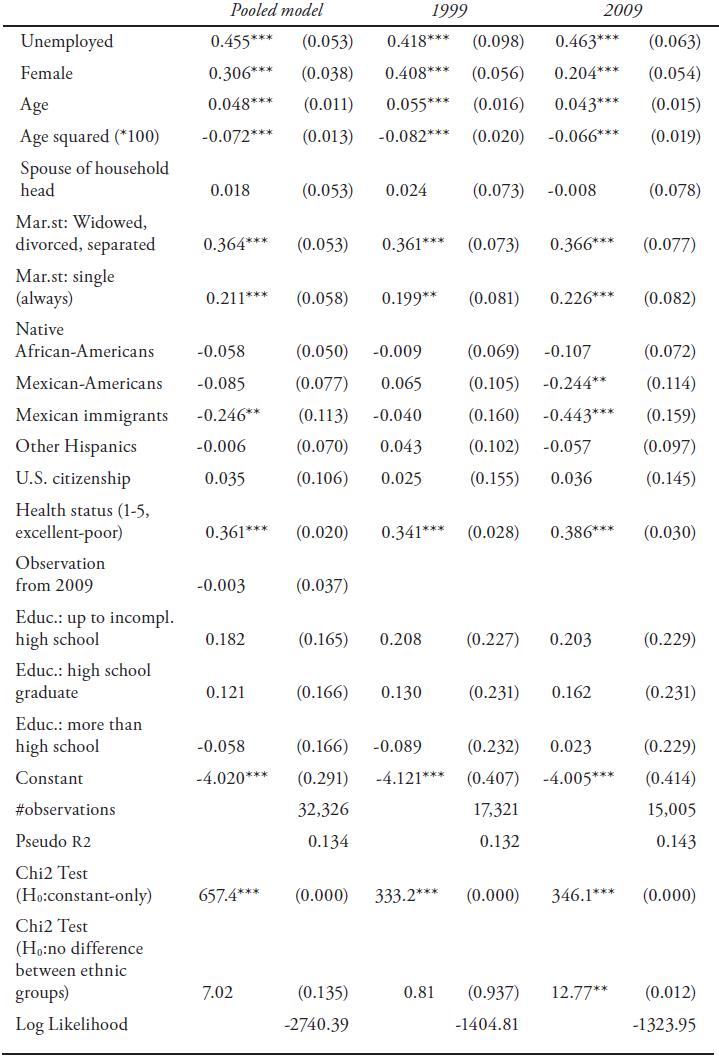
The first column of Table 7 shows the results of the estimation of the model with the pooled data set combining information for the years 1999 and 2009. First, it is necessary to highlight the highly significant effect unemployment has on the probability of suffering serious mental health disorders: Unemployment causes a high prevalence of mental health problems. Other relevant aspects are that, under the same circumstances, women and the elderly population are more likely to report mental health issues (although age effects show a decreasing rate, as indicated by the significantly negative estimate for the squared age variable). Unmarried people show a higher tendency to experience mental health problems, where those who are single due to a marriage breakup or the death of their partner are even more prone to develop that type of problem than those who are alone by their own choice.
Table 7 Probit models for the explanation of the occurrence of a serious mental health problem, 1999 and 2009
Source: Own calculations on the basis of NHIS, 1999 and 2009 (IHIS, 2012). *p<0.10, **p<0.05, ***p<0.01.
Regarding education, we did not find significant differences between the reference group formed by people with a primary education level alone and people with some level of secondary education, with high-school education, or with a higher level of education. It is important to notice that in this analysis the ethnic group one belongs to does not seem to be a highly relevant factor when it comes to mental health: in the pooled sample, the only exception to this is that Mexican immigrants show a significantly lower propensity to suffer mental health problems in comparison with the non-Hispanic white natives. Those with a poorer general (self-reported) health, measured on a five-point scale ranging from excellent (1) to poor (5), are more likely to suffer from mental health problems. Estimating the model without self-assessed health gives a slightly higher effect of unemployment on mental health, which could be because part of those who report poor general health do that for mental health problems, but also because the impact of bad health on unemployment will be captured by its indicator, if health status is not among the explanatory variables for mental health.
It is also important to take into account that the year indicator is not significant, which suggests there are no differences in the prevalence of mental disorders between 1999 and 2009, even though the descriptive information revealed a relative increase in the number of people with a mental disorder in 2009. However, changes in the composition of the population could result in different estimates for the effect of each individual characteristic in both years. Because of this, in columns 2 and 3 of Table 7, the same model is estimated for each year separately. The effect of unemployment on mental health in 2009 is slightly higher than in 1999, although the difference is not statistically significant. The effect of gender on mental health is different in both years. Although in both 1999 and 2009 women showed a greater tendency to experience mental health problems, the breach between men and women was reduced in 2009. Another important finding of this analysis is that the role of the ethnic group has changed from one year to the other. In 1999 there were no statistically significant differences between the ethnic groups and the non-Hispanic white natives after we controlled for the other characteristics, whereas in 2009 Mexican-Americans, and especially Mexican immigrants, reported a lower tendency to suffer a serious mental health problems than non-Hispanic white natives.
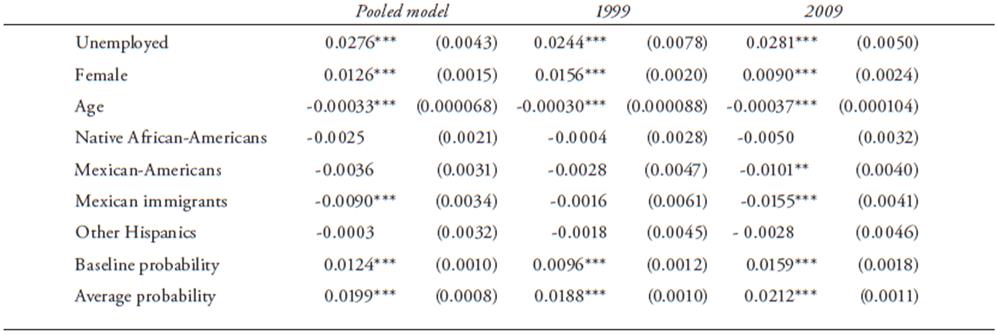
Table 8 presents the marginal effects of the variables that show interesting differences in their estimates between 1999 and 2009 on the incidence of serious mental health problems. Marginal effects have an advantage in that they can be interpreted as changes in probabilities when the characteristics differ; the numbers reported in this table are calculated by predicting the probability of a mental health problem for every respondent in the sample while fixing one characteristic and comparing the average probabilities when it applies with the situation where it does not apply (for age, the difference in probabilities of a mental health problem at each individual’s true age and one year older-while taking into account that also the squared age changes-is calculated, hence the number reflects the impact of one additional year on the probability of a severe mental disorder). For example, the first entry in column 1 of Table 8 tells us that the probability of a mental health problem in case of unemployment is 2.76 percentage points higher than with employment. The last row in the table reports the average probability, while the penultimate row reports the “baseline probability” that applies for employed white males. This implies that the impact of unemployment on mental health is large, given the baseline and average probabilities of 1.24 and 1.99 %, respectively.
Table 8 Marginal effects of selected variables on mental health problems, 1999 and 2009
Source: Own calculations on the basis of NHIS, 1999 and 2009 (IHIS, 2012). *p<0.10, **p<0.05, ***p<0.01.
Table 9 shows the impact of the change in the composition and makes the change in the effects of the parameters even clearer by listing the out-of-sample predictions. In the first panel, the predicted probability of mental health problems in the sample of 1999 using the parameter estimates of that same year (row a, giving the same result as in Table 8) respectively, and using the parameters found in 2009 (row b) is presented. The results show that the average predicted probability of a mental health problem is rather similar under the two different parameter sets. The second panel of Table 9 shows the predicted probabilities in the sample of 2009 with the parameters estimated for 1999 (row c), and the parameters found in resp. 2009 (row d). Also, in the 2009 sample we find that the average predicted probability of a mental health problem is rather similar in both parameter sets. Hence, keeping the same sample but using different parameters does not change too much, while keeping the same parameters but changing the sample (comparing row a with c and row b with d) leads to a major shift in predicted probabilities. This suggests that the differences between 1999 and 2009 are not the result of differences in the reaction to the characteristics, but instead are the consequence of changes in them between the two years.
Table 9 Within-sample and out-of-sample predictions, 1999 and 2009

Source: Own calculations on the basis of NHIS, 1999 and 2009 (IHIS, 2012). *p<0.10, **p<0.05, ***p<0.01.
Effects in Subsamples by Gender and Ethnic Group
The estimations presented in Table 7 indicate a large difference between men and women regarding the incidence of mental health problems. In Table 10, the effect of unemployment on the mental health of men and women is estimated. The greater incidence translates into higher baseline probabilities and also in a stronger effect of unemployment on the mental health of women, both in the pooled sample, as well as in the samples for 1999 and 2009. Nevertheless, in 2009 the differences in the effect of unemployment on mental health between women and men are reduced, compared with 1999. Although the difference does not appear to be significant, it suggests that the increased unemployment during the crisis has hit harder on the mental health of men while among women the changes between 1999 and 2009 are small.
Table 10 Effect of unemployment on mental health, by gender (a)
(a) Preliminary tests suggest the validity of the instruments is maintained in the subsamples.
Source: Own calculations on the basis of NHIS, 1999 and 2009 (IHIS, 2012). *p<0.10, **p<0.05, ***p<0.01.
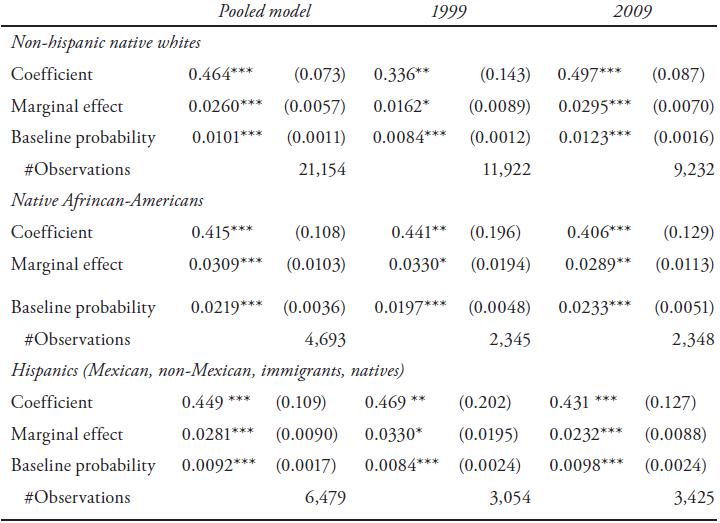
Estimates of the effect of unemployment on mental health in subsamples, with respect to ethnic group, are presented in Table 11, comparing native whites, African-Americans, and Hispanics4. A first result is that the baseline probabilities in 1999 are rather similar for native whites and Hispanics, and that only for whites they strongly increased in 2009, but not for Hispanics. For African-Americans, in both years the baseline probability of reporting a mental health problem is more than double the probability that native whites or Hispanics report such problem. Especially in 1999, the impact of unemployment on mental health among African-Americans and Hispanics is clearly larger than among native whites (though with overlap ping confidence intervals): the latter seemed to be less sensitive for mental issues due to unemployment. However, we find that the impact of unemployment on mental health problems rose between 1999 and 2009 for native whites but decreased for African-Americans and Hispanics. As a consequence, the impact of unemployment for native whites in 2009 is slightly larger than in the other ethnic groups. The economic downturn in 2008 appears to have affected the mental problems of the native whites in a more substantial way than in the other groups that are traditionally more disadvantaged. For Hispanics, the marginal effect was on the higher end in 1999, but is on the lower end in 2009.
Table 11 Effect of unemployment on mental health, by ethnic group (a)
(a) Preliminary tests suggest the validity of the instruments is maintained in the subsamples.
Source: Own calculations on the basis of NHIS, 1999 and 2009 (IHIS, 2012). *p<0.10, **p<0.05, ***p<0.01.
Discussion and Conclusions
The results confirm our hypothesis and are consistent with those of other studies cited in this article: unemployment has a large negative impact on the mental health of the unemployed. Al though we expected to find greater propensities to experience psychological disorders in 2009, when an unprecedented growth of unemployment rates in the United States had started, our findings reveal that there are no major differences between the probability of experiencing severe mental health problems between 1999 and 2009. Another important result is the higher propensity to experience severe mental health problems for women, as well as for those who are single by their own choice and for the elderly, after controlling for other differences. Also, we find indications that the impact of unemployment on the incidence of severe mental health problems among women is stronger, but that the difference between men and women is smaller in the crisis of 2009 than in the boom of 1999. Moreover, the economic down turn in 2009 appears to have affected the mental problems of the native whites in a more substantial way than among African Americans and Hispanics, groups that are traditionally more dis advantaged economically and socially; it seems that the crisis hit hard also among those who may have felt rather safe. Moreover, we find indications that at least part of the changes over time in the prevalence of mental health problems relates more to changes in the composition of the studied groups, i.e., to changes in the predominant characteristics such as an increased number of immigrants from Mexico, than to the changes in the impact of each of the characteristics.
An outcome that catches our attention, but that also confirms the results of previous research and has been coined the Hispanic health paradox, is the low prevalence of mental disorders among immigrants of Mexican origin. The paradox is also reflected by the finding that-comparing 1999 with 2009-the economic crisis seems to have increased the impact of unemployment on mental health among native whites while reducing its relevance for Hispanics. It is useful to point out some factors that can be behind these outcomes. First, it is possible, as noted in other studies, that the lower prevalence of mental disorders is associated with the selectivity of emigration, i.e., the healthier and younger people who are capable to work decide to emigrate. The relevance of the group composition that is found in our data, appears to confirm this possibility, although selection is not the only way to generate differences in composition. Second, a greater tolerance for mental illnesses and support networks formed by family, relatives, and friends is another factor that could explain the low propensity of Mexican immigrants to experience this kind of distress. With the data at hand we could not control for the differences in social networks and their role in the explanation of the difference variation in the prevalence of mental health issues. The same holds for the conditions and expectations that the immigrants had before deciding to find try their luck in the United States. For instance, a recent migrant's situation in that country may be worse compared to with their U.S.-born counterparts, but still be better than the original situation, which could counteract feelings of frustration and failure that would have arisen in other circumstances. Moreover, it is also necessary to mention that immigrants have shorter unemployment durations than the non-Hispanic white native population (Department of Labor, 2012), while it is known that mental disorders increase with longer periods of unemployment. Altogether, Mexican-Americans and the (heterogeneous) group of other Hispanics appear to be more similar to U.S.-born African Americans or native whites than the Mexican immigrants.
Ideally, future research should be done with longitudinal data that follows individuals over time and includes information about social, psychological, but also cultural factors, which would en able a strengthening of the identification of causal effects without the need to use instrumental variable techniques, as well as improve the comparison of different ethnic groups.
An implication of our findings that is relevant for the ongoing discussion regarding the U.S. immigration policy reform, is that (Mexican) immigrants do not seem to be the high burden for the costs of the health-care system in the United States that they are sometimes claimed to be.

