











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Multiple sclerosis (MS) is a chronic inflammatory demyelinating disease of the central nervous system. It is most common in adults and affects more than two million people worldwide. It follows a variable progression, leading to disability and high costs for healthcare systems1,2. Diagnosis is based on the Mc-Donalds criteria, the expanded disability status scale (EDSS) which assesses disease progression and magnetic resonance imaging (MRI). MRI plays an important role in clinical practice by enabling accurate diagnosis. It helps to understand the evolution of the disease and to evaluate treatments by monitoring response to treatment3-5. All of this is based on the McDonald criteria, but until now, these criteria have not included the cortical lesions that have been recently described6-9.
Cortical lesions are more frequently observed in primary and secondary progressive forms, affecting the cerebral and cerebellar cortex, particularly in the hippocampus and cerebellum10,11. They are less common in acute and remitting forms but tend to be larger in size. Considered an additional pathological substrate, they contribute to cognitive decline in these patients. Cortical lesions are significant in the neurodegenerative phase of recurring variants2,12,13. Magnetic resonance imaging assessment of cortical lesions in MS patients improves disease monitoring and diagnosis and enables precise treatment targeting by providing a detailed understanding of lesion location and morphology7,12,14-16.
The purpose of this study was to provide a description of the most common location and morphology of cortical lesions among MS patients receiving treatment at a tertiary care hospital at Puebla, Mexico.
Materials and methods
A retrospective, descriptive study was conducted on patients with MS who received treatment at a tertiary care hospital of the Mexican Social Security Institute (IMSS). Patients diagnosed with relapsing-remitting, secondary-progressive, and progressive-relapsing MS by cranial magnetic resonance imaging were included in the study.
The McDonald criteria are used by neurologists to make a diagnosis of MS9,13. Based on the current classification of progressive, non-progressive, activity-including, and activity-excluding variants, patients meeting the operational definitions outlined below were included in the study13,17.
The MS subtypes were defined as:
– Relapsing-remitting: Clearly defined episodes of new or increasing neurological symptoms, such as vision problems, vertigo, generalized weakness, ataxia, and loss of bladder control, are followed by periods of recovery or remission13,17.
– Secondary-progressive: characterized by evidence of disability accumulation over time, with or without relapses or new activity observed in MRI images13,17.
– Progressive-relapsing: Deterioration in neurological function or accumulation of disability from the onset of symptoms, with initial periods of relapse and/or remission13,17.
Procedure
The diagnosis of the subtype of MS was provided by the neurology service, in addition, age, sex, EDSS score, and annual relapse rate were evaluated, which were data collected during outpatient visits; the Montreal Cognitive Assessment (MOCA) was used to evaluate cognitive impairment, taking < 26 points as cognitive impairment, according to the recommendations of the MACFIMS consensus18.
The morphology, location, and number of cortical lesions were taken from the final report of the radiodiagnostic and imaging service.
Results
A total of 25 patients were included, 10 (40%) were men and 15 (60%) were women.
The most common MS subtype was relapsing-remitting, found in 23 (92%) patients, while secondary-progressive was less common, found in 2 (8%) patients. Cognitive impairment was observed in only 5 (20%) patients.
The most common location of cortical lesions was the parietal region (Fig. 1), found in 21 (84%) cases, followed by the temporal location, found in 4 (16%) cases.
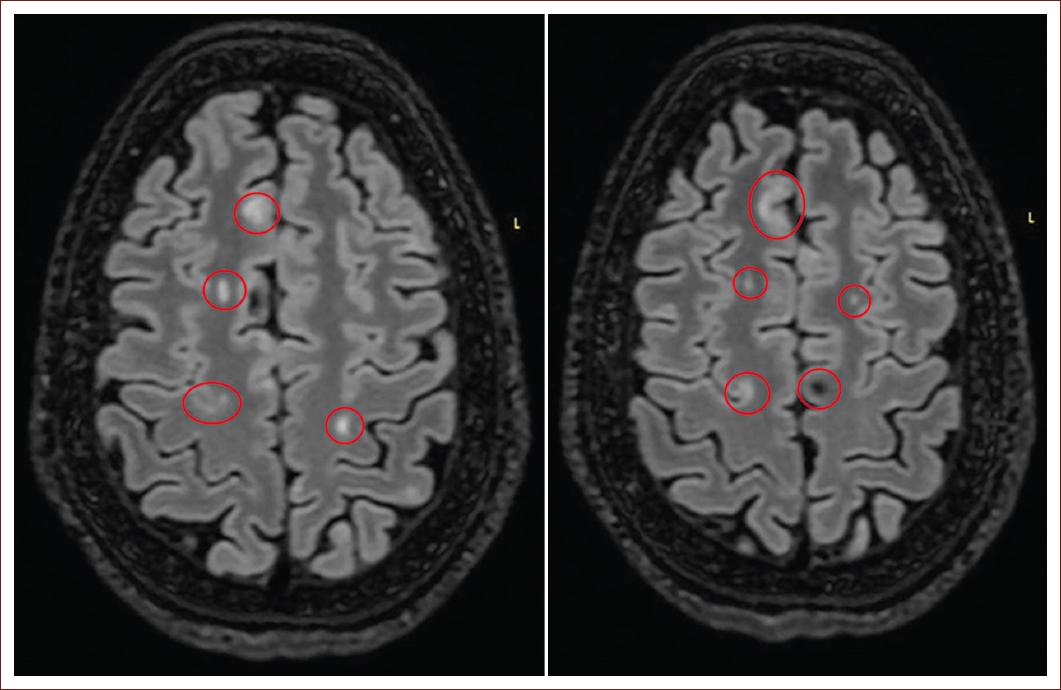
Figure 1 Fluid attenuated inversion recovery enhanced sequence, axial plane, subcortical, and juxtacortical frontoparietal demyelinating plaques.
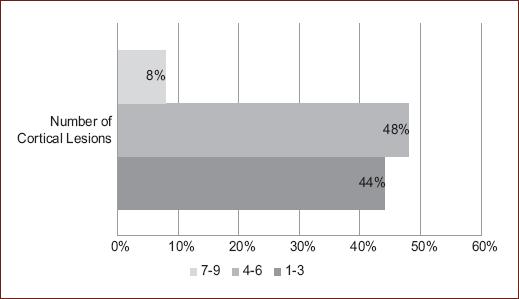
The most common morphology was juxtacortical (Fig. 1), found in 64%, and mixed, found in 36%. On the EDSS scale, the most frequently observed scores were 0.0 and 3.5 (Fig. 2). According to the number of cortical lesions, 4-6 (48%) were the most common (Fig. 3).
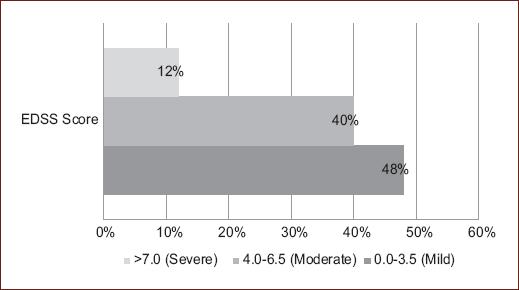
Figure 2 Disability in patients with multiple sclerosis (expanded disability status scale scale score) (n = 25).
The predominant number of relapses was 1 (52%), followed by 0 relapses 40%, the correlation of the number of lesions with relapses and with EDSS was 0.58 (p = 0.02) and 0.678 (p < 0.0001), respectively. The association between lesion count and EDSS score showed statistically significant differences. (Fig. 4)
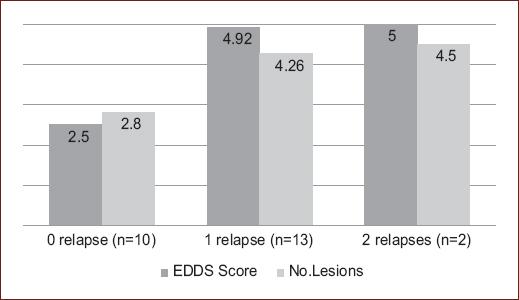
Figure 4 Distribution of number of lesions and disability (expanded disability status scale score) by number of relapses in patients with multiple sclerosis (p < 0.0001).
Cognitive impairment was more prevalent in women with 80% (n = 4) compared to men with 20% (n = 1) (p = 0.6).
The number of lesions and cognitive impairment did not showed a significative correlation, with an asymptotic Pearson Chi-squared value of 0.464 and a likelihood ratio of 0.391.
The association of lesion morphology with the EDSS scale did not show a correlation, with an asymptotic likelihood ratio of 0.112 and a Chi-squared of 0.311.
Discussion
The predominance of the variable sex, age, and type of MS is consistent with previous reports in the Mexican population15.
It is noteworthy that the percentage of cognitive impairment does not agree with previously reported studies, in our study, it was only present in 20%, while in others, it is variable (40-70% and 42-52.5%)19,20.
Cognitive impairment does not correlate with physical disability and can be present in early stages of the disease. The most frequently affected areas are information processing speed, working memory, visual and verbal memory, verbal fluency, learning, word retrieval, and executive functions18,20. Because a neuropsychological evaluation was not conducted to assess a baseline state of cognitive impairment or any previously established alterations in mental functions, these aspects remain unclarified19,21.
The predominance in our study of the MS subtype was relapsing-remitting, having concordance with other previous imaging and histopathology studies22,23.
The average number of lesions is relatively higher in our study (4.01) compared to the population of Harrison et al. (3.38)24. However, both coincide closely in the intrinsic gradual relationship with the presence of high EDSS scores. The greater the number of lesions, the higher the EDSS score.
Pareto et al. describe only the relationship of the presence of juxtacortical lesions in patients with relapsing remitting MS describing that there is cortical thinning and loss of subcortical gray matter25.
This study complements the previous line of research by also describing the location and making correlations with other variables, finding that the most common morphology was juxtacortical lesions and the most common location was the parietal region. These findings cannot be compared because there is no existing literature that reports the morphology and location of lesions by brain lobe, making this the first studies of its kind in Mexico26.
It was observed that the number of lesions was associated with the number of relapses, and in turn, if the patient presented one or more relapses, was associated with intermediate EDSS scores (both p < 0.001). This finding may be due to the small sample size. It is already known from previous literature that these variables are not always directly proportional21,26,27.
Aldrete et al suggest that the number of lesions is associated with greater cognitive impairment; their study was also in Mexican population. In this study, no association was found between the number of lesions and cognitive impairment or between lesion morphology and EDSS scale. Several factors, including biological, medical, and psychosocial factors, may contribute to cognitive impairment in MS. These findings need to be investigated in future studies with larger sample sizes21.
The use of high detail resonators is recommended for the identification of more cortical lesions, for this study, 3-T MRI was used28.
Perhaps multicenter studies are needed to increase the sample size. This would allow us to draw conclusions. There is also a need for further monitoring of this research topic to identify areas for better utilization in both clinical and diagnostic settings.

