











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Returning to work after stroke is a challenging task. Nearly two-thirds of all strokes occur among people < 70 years, and young and middle-aged adults are at higher risk due to the increase of classic risk factors in these groups of age1; globally, in 2019, there were almost 101 million stroke survivors and 143 million disability-adjusted life-years, with the largest proportions in developing countries2. Stroke leads to loss of work production, with a subsequent impact on socioeconomic indicators. Stroke survivors are less likely to be employed and they earn a lower hourly wage than the general population3.
The number of stroke survivors who are capable of returning to work varies across differen\t studies (44-75%)4-7, but the general considerations related to return to work barriers after a stroke are based on previous academic level, socioeconomic status, higher age at stroke, type of work, severity of stroke, recurrent stroke, walking ability, subtype of stroke, depression, and even ethnicity8-12. These factors could be related to changes in working conditions for post-stroke patients, with modifications such as a decrease in the number of working hours, work shift, complexity of the labor, and even unemployment13,14.
Work performance after stroke is determined not only by the probability of being active in daily job activities but also by the ability to recover in different cognitive and motor areas to perform tasks as they previously had. The self-reported impact on the work modifications, level of disability, and work satisfaction in stroke survivors who return to work has been poorly studied, and no specific tools for this evaluation have been developed. Many tools, such as the Barthel Index, the performance assessment of self-care skills, or the Lawton and Brody assessment scale, intend to determine the level of independency after stroke15, but the patient's perception about their performance when returning to work is sometimes underestimated by these and other assessment tools16.
We developed a quality of performance questionnaire for ischemic stroke survivors who had returned to work to evaluate the self-perception of work performance according to the compromise of different skills and cognitive domains as a result of the index stroke.
Materials and methods
Study population
Consecutive patients with first-ever confirmed ischemic stroke treated at the Stroke Clinic and the Rehabilitation Department from the Instituto Nacional de Neurologia y Neurocirugia (a third level referral center in Mexico City) were recruited from January 2014 to December 2016 (collection dates were part of the internal validation of the questionnaire, which is intended to be analyzed in a prospective protocol after this phase and currently at the Rehabilitation Department). Clinical data from these patients related to the index stroke were extracted from the Stroke Clinic's dataset, which is a prospective database collecting data from stroke patients since 1982.
The inclusion criteria consisted of ischemic stroke survivors (confirmed with local protocol imaging studies) who were admitted to the rehabilitation facility and had subsequent follow-up appointments at the outpatient stroke clinic for at least 3 months. Included patients were > 18 years old, were employed at the time of the stroke, were able to return to work after the index stroke, and were actively working at least 3 months by the time; they were recruited to the study.
All patients had a standardized diagnostic follow-up, laboratory, and treatment protocol according to institutional guidelines for stroke care. The dataset included demographics, medical history, risk factors, stroke onset time, arrival time at the hospital, complications, treatment, imaging characteristics of the index stroke, procedures, and ambulatory status at discharge and these were registered for each patient. Risk factors and predisposing conditions for ischemic stroke were also registered.
Clinical outcome was defined using the modified Rankin score (mRs) as follows: Good clinical outcome (mRs = 0-2) and bad clinical outcome (mRs > 2). The Montreal Cognitive Assessment (MOCA)17 was used to evaluate and establish cognitive status (abnormal < 25 points); the Barthel Index (independent = 80-100 points)18 and Lawton and Brody (independent=8 points [female] or > 5 points [male])19 instruments were used to evaluate levels of independency at the time of the questionnaire completion. The Institutional Review Board from the Instituto Nacional de Neurología y Neurocirugía approved the present study, and each participant gave informed consent before being included in the study.
Work-related definitions
The time to return to work was evaluated for each patient and was the time from when the patients started at the outpatient rehabilitation clinic until full integration in their working place. Work-paid jobs are defined as jobs with explicit (written or oral) employment contracts that give the patient basic remuneration20. Type of occupation was classified as white-collar workers (performing professional or administrative work), blue-collar workers (performing non-agricultural manual labor), business workers (commerce activities), and family business or domestic chores (self-paid services at a local business or for agricultural or domestic chores).
Work performance questionnaire (WPQ) development
A 15-item questionnaire (WPQ) evaluated 11 different domains (language, memory, attention, planning, calculating, writing, motor skills, gait, visual, mood, and self-perception) related to basic performance activities at work (Table 1).
Table 1 General characteristics
| Variable | Female n = 51 (%) | Male n = 49 (%) | Total n = 100 | p |
|---|---|---|---|---|
| Age, years* | 42 (34-55) | 49 (37-57) | 42 (34.5-54.5) | 0.23§ |
| Academic background | ||||
| Primary school | 4 (7.8) | 6 (12.2) | 10 (10.0) | 0.93 |
| Secondary school | 17 (33.3) | 17 (34.7) | 34 (34.0) | |
| College | 28 (54.9) | 25 (51.1) | 53 (53.0) | |
| Risk factors | ||||
| Hypertension | 20 (39.2) | 20 (40.8) | 40 (40.0) | 0.87 |
| Diabetes | 13 (25.5) | 12 (24.5) | 25 (25.0) | 0.91 |
| Dyslipidemia | 18 (35.3) | 15 (30.6) | 33 (33.0) | 0.62 |
| Active smoking | 11 (21.6) | 20 (40.8) | 31 (31.0) | 0.03 |
| Stroke features | ||||
| Oxfordshire classification | 29 (56.9) | 24 (49.0) | 53 (53.0) | 0.48 |
| PACI | 1 (2.0) | 2 (4.1) | 3 (3.0) | |
| TACI | 14 (27.5) | 11 (22.4) | 25 (25.0) | |
| POCI | 7 (13.7) | 12 (24.5) | 19 (19.0) | |
| LACI | 21 (41.2) | 28 (57.1) | 49 (49) | |
| Topographic localization | ||||
| Left hemisphere | 14 (27.5) | 12 (24.5) | 26 (26.0) | 0.35 |
| Right hemisphere | 7 (13.7) | 2 (4.1) | 9 (9.0) | |
| Brainstem | 4 (7.8) | 4 (8.2) | 8 (8.0) | |
| Cerebellum | 2 (0-5) | 3 (0-6) | 3 (0-5) | |
| NIHSS median (IQR) | 0.56 | |||
| Cognitive and functional scales (3 months) | ||||
| MOCA abnormal (< 25) | 26 (51.0) | 24 (49.0) | 50 (50.0) | 0.84 |
| Good functional outcome (mRs = 0-2) | 45 (88.2) | 48 (98.0) | 93 (93.0) | 0.06 |
| Independent (Barthel index) | 50 (98.0) | 48 (98.0) | 98 (98.0) | 0.97 |
| Independent (Lawton and Brody) | 45 (88.2) | 45 (91.8) | 90 (90.0) | 0.56 |
| Work features | ||||
| Time to return to work in months* | 4 (3-7) | 4 (2-8) | 4 (2-7) | 0.39§ |
| Work-paid employee | 32 (62.7) | 47 (95.9) | 79 (79.0) | < 0.001 |
| Type of work | ||||
| White-collar worker | 7 (13.7) | 17 (34.7) | 24 (24.0) | 0.001 |
| Business worker | 5 (9.8) | 3 (6.1) | 8 (8.0) | |
| Blue-collar worker | 20 (39.2) | 27 (55.1) | 47 (47.0) | |
| Family business/domestic worker | 19 (37.2) | 2 (4.1) | 21 (21.0) | |
| Part-time job pre-stroke | 1 (2.0) | 0 | 1 (1.0) | 0.32 |
| Part-time job post-stroke | 21 (41.2) | 18 (36.7) | 39 (39.0) | 0.65 |
*Median (interquartile range);
§p by U-MannWhitney test. mRs: modified Rankin score.
Summary scores represent the sum of item-level responses for each domain and higher scores indicated poorer work performance. Item-level responses were categorized on a numerical interval ranging from 1 (no difficulty) to 4 (severe difficulty) (see Supplementary data Appendix 1). Total points were assigned to four categories of work performance: high (1-5 points), good (6-15 points), moderate (16-29 points), and low performance (30-45 points). All interviews were performed by two trained physicians (ES and RU) who were not involved in the evaluation of the functional status of the patients and were blinded to the clinical or radiological information of the included patients.
A neuropsychologist evaluated the psychometric properties of the questionnaire, according to each cognitive domain that was evaluated with the instrument, to determine that each question was consistent with the domain's performance.
The questionnaire was developed and applied in Spanish and subsequent linguistic validation was performed for the English version, with a professional translator who performed forward translation, back translation, and examination of the language quality (see Supplementary data Appendix 2).
Statistical analysis
Categorical variables are expressed as frequencies and percentages, and continuous variables are expressed as the means ± standard deviation or median and interquartile range (IQR) when appropriate, according to a normality distribution test (i.e., the KolmogórovSmirnov test). Association of categorical variables was performed using Pearson's χ2 test. p-values under 0.05 were considered statistically significant.
Reliability analysis was performed using a Cronbach's a coefficient to evaluate internal consistency for each domain. The optimal value for this index was considered > 0.7; test-retest reliability, item-scale correlation, and factor analysis were also conducted. The determination of the scale homogeneity was evaluated with an item-scale correlation coefficient, which was considered acceptable with values > 0.40. The validity of the scale was evaluated through exploratory factor analysis after varimax rotation.
All of these statistical analyses were performed using the statistical package SPSS (Statistical Package for the Social Sciences, version 22.0, IBM Inc., Armonk, NY).
Results
Demographics
A total of 100 ischemic stroke survivors were recruited (51 [51.0%] female patients, median age 42 years [IQR = 34.5-54.5 years]); work activities among the patients are described in table 2. Seventy-seven patients presented with a minor stroke (NIHSS = 0-4) at the index event (no significant associations were seen among NIHSS punctuation and levels of satisfaction according to the questionnaire); MOCA cognitive assessment scores suggested impairment in 50 patients. The mRs at 3 months was good (0-2) in 93% of cases. The median time to return to work was 4 months (IQR = 2-7 months), with 39 patients (39%) decreasing the work schedule to part time and 100% of subjects remaining in the same work place as before the index stroke, but nearly 39% changing the type of work (i.e., work was adapted to functional status).
Table 2 Working performance questionnaire after stroke and the assessed cognitive domains according to each question
| Domain | Question | |
|---|---|---|
| 1 | Language (production) | Do you have verbal difficulties expressing what you think at work? |
| 2 | Language (comprehension) | Do you have troubles understanding what others say at work? |
| 3 | Short-term memory | Do you have any trouble recalling a phone number or a name that was recently told to you (< 5 min)? |
| 4 | Long-term memory | Do you have any trouble recalling specific functions that you did at work previous to the stroke? |
| 5 | Attention | Do you have troubles focusing on specific tasks at work for more than 1 h? |
| 6 | Planning | Do you have troubles following instructions in performing a task that you previously did without difficulty at work? |
| 7 | Calculation | Do you have troubles doing mathematical calculations that you used to do without difficulty at work? |
| 8 | Writing | Are you able to do writing tasks at work? |
| 9 | Fine motor skills | Are you able to use tools with your hands with similar ability as before the stroke? |
| 10 | Gross motor skills | Are you able to lift the same weight with both arms as before the stroke? |
| 11 | Gait | Are you able to walk without difficulty at your workstation? |
| 12 | Vision | Have you noticed troubles in your visual field at work? |
| 13 | Autoperception | Do you feel that you are able to go back to a full work life? |
| 14 | Mood | Have you been sad due to your work performance (for more than 4 weeks)? |
| 15 | Satisfaction | Do you feel satisfied with your current work performance after the stroke? |
Reliability
Chronbach's alpha coefficient was 0.75 for the overall analysis, ranging from 0.718 to 0.765. The Kaiser-Meyer-Olkin measure of sampling adequacy was 0.72 (p < 0.001) (Table 3). The test-retest reliability, as estimated by the intraclass correlation coefficients, was good (> 0.70 for all the factors). Scale homogeneity according to the item-scale correlation coefficient was > 0.40, with an item-total scale correlation ranging from 0.47 to 0.74.
Table 3 Reliability analysis of working performance questionnaire after stroke*
| Domain | Scale's mean when suppressed | Total corrected correlation | Chronbach's α when suppressed |
|---|---|---|---|
| Language (production) | 11.16 | 0.32 | 0.740 |
| Language (comprehension) | 11.17 | 0.45 | 0.729 |
| Short-term memory | 10.94 | 0.44 | 0.729 |
| Long-term memory | 10.93 | 0.38 | 0.734 |
| Attention | 11.11 | 0.31 | 0.741 |
| Planning | 11.29 | 0.40 | 0.734 |
| Calculation | 11.17 | 0.38 | 0.734 |
| Writing | 10.75 | 0.52 | 0.718 |
| Fine motor skills | 10.75 | 0.52 | 0.719 |
| Gross motor skills | 10.80 | 0.43 | 0.729 |
| Gait | 10.96 | 0.21 | 0.753 |
| Vision | 11.19 | 0.04 | 0.765 |
| Autoperception | 10.26 | 0.18 | 0.761 |
| Mood | 11.00 | 0.50 | 0.725 |
| Satisfaction | 11.02 | 0.32 | 0.740 |
*Scale statistics: Mean: 11.75, Variance: 41.7, SD: 6.4.
Validity
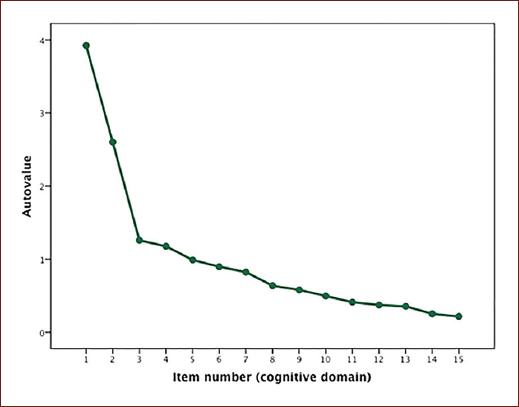
Work performance after stroke was high in 16 (16%) cases, good in 58 (58%) cases, moderate in 24 (24%) cases, and low in 2 (2%) cases. Memory, language, and attention explained 59.7% of the cumulative variation of the questionnaire in the extraction analysis (Table 4), which is visually displayed in the sedimentation graphic (Fig. 1); extraction values ranged from 0.35 to 0.75.
Table 4 Working performance questionnaire after stroke after varimax rotation
| Domain | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|---|
| Language (production) | 0.405 | 0.191 | −0.586 | −0.320 |
| Language (comprehension) | 0.617 | 0.154 | −0.321 | −0.450 |
| Short-term memory | 0.660 | 0.108 | 0.147 | −0.204 |
| Long-term memory | 0.624 | −0.004 | 0.516 | −0.143 |
| Attention | 0.646 | −0.080 | −0.021 | 0.223 |
| Planning | 0.711 | 0.039 | −0.201 | 0.222 |
| Calculation | 0.659 | −0.004 | 0.022 | −0.146 |
| Writing | 0.180 | 0.790 | −0.165 | −0.037 |
| Fine motor skills | 0.170 | 0.779 | 0.116 | −0.064 |
| Gross motor skills | 0.019 | 0.828 | 0.013 | 0.102 |
| Gait | −0.244 | 0.778 | 0.251 | 0.045 |
| Vision | 0.109 | 0.090 | −0.079 | 0.824 |
| Autoperception | 0.052 | 0.303 | 0.655 | −0.152 |
| Mood | 0.688 | 0.174 | −0.114 | 0.103 |
| Satisfaction | 0.591 | 0.006 | −0.005 | 0.004 |
Discussion
In the present study, we developed a post-stroke WPQ to evaluate the self-perception, according to various cognitive domains, of the ability to return to previous activities; this tool is reliable and valid and could be used to define the grade of performance of an individual when returning to work after an index stroke.
Satisfactory internal consistency (Chronbach's alpha coefficient > 0.70), with good test-retest reliability, was achieved with our questionnaire, and nearly 57.9% of the questionnaire could be explained by factors related to memory, attention, and language, which seem to be the most common limitations detected by patients when returning to work and evaluating performance satisfaction.
Job satisfaction is a self-perception that could be determined by many factors, including personality, social and family influence, educative status, and previous professional status21. Adapting after stroke, not only in terms of functional limitations but also in terms of performing work activities with the same quality as they previously had, is a challenging task. Self-perception of work performance in this scenario has been poorly studied22,23, especially because there are certain considerations that the patient and his employer could have: from one side, there are the patient's motivation, socioeconomic status, daily work activities complexity, job demands, and self-efficacy24; and on the other side, from the employer perspective, there are some concerns when stroke patients return to work, related to assessing functional capabilities for their previous work activities, safety assessments, the work environment, requirements and adaptations, and legal responsibilities, and these issues are a result of their disabilities and need to be overcome25. The possibility of maintaining the balance between these two viewpoints is very complex work that should be analyzed at the government and institutional levels, as there are many difficulties to overcome, especially adapting the work space for stroke survivors returning to work.
From the previous studies23,26, it was demonstrated that patients who were able to return to work had a significantly higher level of subjective well-being and life satisfaction, despite the fact that they faced major changes concerning employers, assignments, and working hours. In our sample, 39% of patients had changes in their work hours, shifting from a full-time to a part-time job, which was observed in nearly 95% of the white collar workers, which is another feature that has been reported as a predictor for returning to work24.
Cognitive impairment is a factor that has been reported as one of the most important limitations for returning to work22,23. However, analysis of each domain is important and depends on the characteristics of each type of work and how the specific domain could affect subsequent performance. In our sample, 47% of patients had blue-collar work, and most of them reported good performance when returning to work, independent from the MOCA test results. This could be explained because the complexity of manual labor could be underrated with this cognitive screening tool and because shifting responsibilities in manual labor jobs could be an easier task for employers; on the other hand, this should also be analyzed carefully, and the cognitive domains should be evaluated in a more detailed manner with neuropsychological tests to obtain more reliable information that can be assessed with regard to each task that the patient does as his/her daily working activities27.
What is the benefit of developing a satisfaction questionnaire in stroke survivors who return to work? Even in stroke survivors with minimal or no physical disability, perception of difficulties in adapting again to their work activities has been documented28-30; therefore, knowing the subjective perception on this matter is fundamental when establishing vocational therapy programs, preparing for returning to work, adapting the work place with employers, and even helping a workplace advocate to support stroke survivors to gain confidence when reassuming their work responsibilities28. Another advantage of using this satisfaction questionnaire is as an aid to employers and rehabilitation programs, for those domains whose perception for the employee, should be improved; cognitive, occupational, and multiple-task therapy programs could be paired to the questionnaire findings.
Certain limitations should be acknowledged: first, all patients recruited in our study were from a single center, and no external validation from our instrument was performed to evaluate the questionnaire's performance in other clinical settings. Second, this is the analysis from a retrospectively selected sample, with a standardized questionnaire application and functional assessment at the final follow-up visit, but to increase the internal and external validity of this tool, a prospective analysis in a more consistent and homogenous sample should be performed; also, for the purpose of this questionnaire to become a diagnostic tool to improve quality and work satisfaction, the above mentioned bias in terms of multicenter and sample size limitations should be explored in a prospective protocol. Third, our sample size, despite the fact that for the purpose of the questionnaire development and evaluation was adequate, should be increased to have a higher predictive power. Fourth, our sample of stroke patients included younger and less severe cases (NIHSS < 4), which could also introduce a bias, as older patients could face a more difficult path to work return, which could explain why the majority of patients who have been included in other studies find it difficult to return to work. In addition, despite the fact that these patients were younger, returning to work was achieved in a median time of 4 months, which can be explained by the usual protocols of physical and occupational therapy (1-3 months) that depend on the severity of the index stroke.
Conclusion
The WPQ-INNN is a reliable and valid tool for the assessment of performance quality in stroke survivors who returned to work, with the highest prediction ability based on memory, language, and attention. This instrument should be validated in prospective studies.
Supplementary data
Supplementary data are available at DOI: 10.24875/RMN.23000044. These data are provided by the corresponding author and published online for the benefit of the reader. The contents of supplementary data are the sole responsibility of the authors.

