











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Stroke is one of the diseases with the greatest impact on public health, being the third cause of mortality and leading cause of disability in the western world since most patients suffer sequels, which in 30% of cases disable them to perform daily activities1,2.
The proportion and frequency between the ischemic types and intracerebral hemorrhage (ICH) are variables according to a determined region; while in Spain, the rates of ICH are around to 12%3, in regions of South America such as Ecuador and Chile, the ICH reach rates between 37 and 46%4. In Paraguay, cerebrovascular disease is the fourth cause of death5. However, other data about the baseline characteristics in our population are not widely known.
Among the cardiovascular risk factors related to stroke, hypertension is the most frequent and important risk factor. The prevalence is around 70% in both ischemic and hemorrhagic patients and its optimal control is possibly one of the most important interventions in secondary prevention for both types of stroke3,6. In Paraguay, the prevalence of hypertension is high, with rates of 53% in men and 40% in women between 35 and 45 years, reaching up to 81% in the general population between 65 and 74 years7.
Another known and controversial stroke risk factor is gender and their disparities in baseline and clinical outcomes. Several descriptive studies have shown an association of older age, frequency of hypertension, obesity, and atrial fibrillation in women than in men8,9.
Methods
This is a descriptive, observational study in a single center. Data were collected from a prospective of stroke patients admitted in the Stroke Unit of our center since April 2015-March 2019.
The known modifiable and non-modifiable risk factors have been recorded. In patients with hemorrhagic stroke, the etiology of hypertensive ICH has been determined according to the history of hypertension, the topography of the parenchymal lesion, and the vascular study10. The diagnosis of ischemic stroke was made according to the criteria of the Oxfordshire Community Stroke Project and the Trial of Org 10172 in acute stroke treatment11.
The descriptive statistical analysis was performed for all the parameters, which included measurements of the central tendency and dispersion for the quantitative variables, as well as absolute and relative frequencies for the qualitative variables, with their 95% confidence interval (CI) in both cases. If the data did not meet the assumptions of normality for the analysis, non-parametric statistical methods were used (Student’s t-test or Mann–Whitney U-test, respectively). The Chi-square test was applied for the comparison between the proportions. To determine the weight of each of the risk factors between ischemic and hemorrhagic stroke, multiple logistic regression models were established, with a 95% CI. The statistical tests were performed with a significance level of 5%. The statistical program SPSS v. 23.0 was used to perform the analysis.
Results
From 996 patients with stroke, 744 (74.7%) were ischemic and 252 (25.3%) ICH, 390 (39.1%) were women. The mean age was 62.8 years (standard deviation [SD] ± 15.3). From overall, 75.4% had known antecedent of hypertension, 27% diabetes mellitus (DM), and 6.4% dyslipidemia. The median baseline NIHSS was 8 (interquartile range [IQR]: 4-12). The baseline characteristics in general and of the ischemic and hemorrhagic groups are shown in Table 1.
Table 1 Baseline characteristics of all patients with stroke and subgroups, ischemic and hemorrhagic with their significance in the univariate analysis
| All (n = 996) | Ischemic (n = 744) | ICH (n = 252) | p value | |
|---|---|---|---|---|
| Age, year | 62.8 DS ± 15.3 | 64.3DS ± 15.2 | 58.1 ± 14.8 | < 0.001 |
| Glycemia at admission mgr/dl. (n: 169) | 165.4DS ± 120.3 | 168.6DS ± 97.7 | 155.9DS ± 120.3 | 0.513 |
| Female gender n (%) | 390 (39.1) | 295 (39.6) | 93 (36.9) | 0.585 |
| Hypertension n (%) | 749 (75.2) | 553 (74.3) | 195 (77.3) | 0.102 |
| Diabetes mellitus n (%) | 237 (23.6) | 206 (23.5) | 30 (3.4) | < 0.001 |
| Dyslipidemia n (%) | 56 (5.6) | 47 (5.4) | 9 (1) | 0.144 |
| Atrial fibrillation | 128 (12.7) | 117 (13.6) | 11 (1.3) | < 0.001 |
| Prior antiplatelet treatment | 996 (99.1) | 81 (8.1) | 10 (1.0) | 0.003 |
| Prior stroke | 150 (14.9) | 129 (15.4) | 21 (2.5) | 0.001 |
| Baseline NIHSS median (interquartile range) | 8 (4) | 8 (4) | 9 (4) | 0.796 |
| Systolic blood pressure at admission | 169.8 ± 38.3 | 161.4 ± 32.5 | 189.9 ± 43.2 | < 0.001 |
In ischemic stroke patients, the mean age was 64.3 (SD ± 15.2) years, the median of NIHSS 8 (IQR 4-12), and 39.8% were women. Patients with ischemic stroke were significantly older (mean years 64.3 SD ± 15.2 vs. 58.1 SD ± 14.8), had higher glycemia at admission (mean mgr./dl 168.6 SD ± 97.7 vs. 155.9 SD ± 120.3, p = 0.513), frequency of DM (23.5% vs. 3.4%, p = 0.001), atrial fibrillation (13.6% vs. 1.3%, p = 0.001), prior history of stroke (15.4% vs. 2.5%, p = 0.001), prior antiplatelet treatment (8.1% vs. 1.0%, p = 0.001), and lower systolic blood pressure on arrival than patients with ICH (mean mmHg, 169.8 SD ± 38.3 vs. 189.9 SD ± 43.2).
The most frequent etiology were (422 cases work-up performed) cardioembolic 41.2%, indeterminate in 24.1%, lacunar infarcts in 11.6%, and atherothrombotic in 21.5%. Hypertension was present in 91% of atherothrombotic strokes, 89.6% of lacunar strokes, 80.8% in cardioembolic, and 77.6% of indeterminate strokes, Figure 1.

Figure 1 Graphic bar showing number of cases of ischemic stroke etiology according to prior hypertension status.
ICH patients had a mean age of 58.1 (SD ± 14.8) years, the median of NIHSS was 9 (IQR 5-13), and 36.9% were women. From 142 cases with etiological work-up, 79.5% were due to hypertensive hemorrhage. The factors significantly related to hypertensive hemorrhage (113 cases evaluated) were hypertension (p ≤ 0.001) and the lower age stratified by groups (p = 0.006), Figure 2.
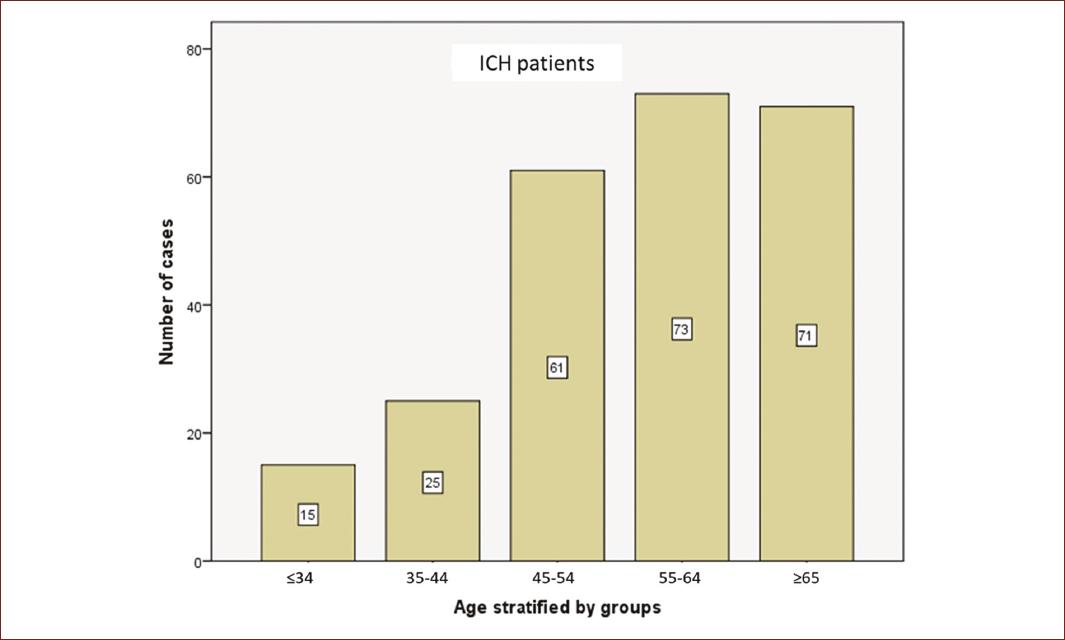
Figure 2 Graphic bar showing number of cases of intracerebral hemorrhage according to stratified age group.
In the multivariate analysis adjusted for sex, hypertension, DM, previous stroke, and atrial fibrillation, age < 60 years old (odds ratio [OR]: 4.893, 95% CI: 1.772-13.509, p = 0.029) and a higher systolic blood pressure at admission (OR: 1.098, 95% CI 1.044-1.155, p = 0.009) were independent factors associated with ICH.
In relation to gender, hypertension was present in 79.3% in men and 83.5% in women. In men, smoking habit was significantly more frequent (23.9% vs. 3.4%, p < 0.001) and they presented more ischemic heart disease (7.9% vs. 2.3%, p = 0.001) than women. Men were younger (61.75 SD ± 13.6 vs. 64.16 SD ± 17.4, p = 0.003), being in the ICH group, even more remarkable the difference (mean years 55.41 [SD ± 14.8] vs. 62.48 [SD ± 15.2], p ≤ 0.001), Figure 3.

Discussion
This is a descriptive study, with data from a prospective cohort over a period of 41 months. In general, there is a higher proportion of men than women with stroke, and the mean age is significantly lower than in developed countries1,3, but similar to the previous studies in Buenos Aires and Brasilia12,13. Hypertension is the most frequent risk factor, slightly higher than other series3,12-14. Another risk factors rate such as DM, previous stroke, and atrial fibrillation was similar to prior studies; however, the frequency of dyslipidemia, known ischemic cardiopathy, and smoking was strikingly lower3,12-14. Possible explanations (in addition to the inherent biases and limitations from the nature of this study) are that our center, although it is located in an urban center, is a reference center that receives patients from the rural area also, and this could affect our results. Another reason would be the lack of knowledge of the risk factors of our population (less than half of men know about their blood cholesterol levels7).
The rate of HIC is significantly higher than that described in developed countries3,12 and is consistent with results from our region in studies conducted in Chile, Ecuador, and Argentina14-16. These results are explained by the high prevalence rate of hypertension in our population, especially manifests at early ages in the adult7.
In relation to ischemic stroke, the etiology by TOAST (in 422 cases) showed a high rate of cardioembolic (41.2%), however, a lower frequency of atheromatous disease (21.5%) and lacunar (11.6%). These results are more similar with those found in Santiago14 than in those shown in Brasilia, Guayaquil, and Buenos Aires13,15,16. It should be noted that in South America, the frequency in relation to the etiology of stroke is very heterogeneous and diverse, mainly due to ethnic, geographical, and sociocultural differences4. Finally, the relative high rate of indeterminate etiology would be related in many cases to an incomplete study and is a clear limitation at the present study.
Interestingly, while hypertension rates are high (79.3%) in ischemic patients, the percentage of lacunar strokes for presumed hypertensive microangiopathy as a cause is lower than expected (11.6%). In contrast, hypertensive hemorrhage represents the cause of up to 79.5% of ICH. The previous studies in relation to this possible common substrate have shown that the cerebral vascular phenotype (ICH vs. lacunar infarcts) due to hypertensive microangiopathy would be related in part to age and cholesterol levels17,18. Therefore, a possible explanation to our findings could be related to age (remarkably younger patients) and the lower frequency of dyslipidemia (5.6%) known in our population. Another possible explanation would be in relation to the less severe clinical deficit associated with lacunar stroke19, which may affect the arrival or referral of these patients. These results are consistent in the region with the previous studies in Santiago de Chile and Bogotá13,20. Unfortunately, the body mass index, which has been shown to be a prognostic factor for the development of ICH or lacunar infarctions in hypertensive microangiopathy18, has not been evaluated in the present study. Future prospective and comparative studies should be taken into account to confirm these findings.
Regarding gender, women presented a stroke less frequently, with greater age (according to literature8,21,22) and significantly less known cardiovascular risk factors than men, which is also consistent with the previous studies. Factors such as hypertension and atrial fibrillation, which in other series showed a significantly higher frequency in women, have not been seen in our study8,9. The age difference in HIC is remarkable among genders, being the higher hypertension prevalence in early age7 and the hypothetical hormonal preventive effect in women20,21 probable reasons of this finding.
As a relevant limitation at the present study, it is a monocentric study, involving patients from urban and rural areas that may not represent a specific geographic area.
In this prospective study in our country, hypertension is a risk factor highly related to stroke with a higher frequency of hypertensive hemorrhages in younger patients than other series, especially in men. The frequency of different stroke subtypes would be related to environmental, sociocultural, and biological factors. Multicenter and comparative studies are warranted to confirm these findings. The intensification of public health programs focused on the control of risk factors, especially hypertension, is necessary to prevent cerebrovascular disease in our environment.

