











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Hepatitis B infection is a global public health problem.1 Around 2 billion people have been exposed worl- wide, and near 350 million have developed a chronic hepatitis B (CHB).2 Hepatitis B virus (HBV) is responsible for 600,000 annual deaths each year.3
Preventive measures by means of widespread use of vaccine, have been associated to decrease the prevalence of CHB in some regions, although absolute number of HBsAg positive persons has increased from 223 million in 1990 to 240 million in 2005.4
The hepatitis B burden is particularly heavy in endemic countries, where liver cirrhosis and hepatocellular carcinoma (HCC) are leading causes of death, but even in developed countries with universal vaccination programs and availability of efficacious treatment, HBV-related dis eases represent an enormous economic and social burden.5
HBV replication measured by serum HBV DNA levels, has been identified as an independent predictor of disease progression. Therefore sustained suppresion of viral replication is essential to prevent fibrosis progression. The European Association for the Study of the Liver (EASL) 2012 guidelines suggest that therapy must reduce HBV DNA to as low a level as possible, ideally below the lower limit of detection by the real-time PCR assay.6
The ultimate goal of CHB treatment is to increase survival by preventing the development of cirrhosis, liver failure, and HCC. Three drugs have been recommended as a first-line therapy for patients with CHB, entecavir, tenofovir and pegylated-interferon (peg-IFN) given as a monotherapy. These recommendations were based on efficacy results and no or minimal risk of HBV drug resistance observed in clinical trials.7 In addition, nucleos(t)ide analogues have shown similar results in real-life studies while interferon has an immune modulator effect with less potent antiviral action.6
The present analysis aimed to estimate the influence of two treatment strategies in the clinical burden of CHB patients, by assesing their effects on disease progression and survival. In addition, the efficiency of the antiviral strategies was assessed, by means of a cost-effectiveness analysis.
MATERIAL AND METHODS
A previously developed Markov model,8 simulating long-term clinical outcomes in CHB patients was used to estimate the survival and the lifetime costs in Euros of a cohort of 1,000 patients with CHB. This cohort which reflected the patients enrolled in the studies GS102 and 103, was adapted to the proportion of HBeAg positive patients identify in the majority of the European countries.9 The study was performed under the perspective of Spanish National Health System.
Interventional therapeutic strategies
Two different strategies of antiviral treatment were explored following the current EASL recommendations for CHB management.6
The first strategy (strategy 1) considered treatment for 71% of patients diagnosed with CHB and candidates to therapy based on the estimation of a survey of CHB patients management practices in the European Union.10 The second strategy (strategy 2) increased the rate of treatment assuming a full treatment coverage (100% of treated patients).
The assessed drugs were those recommended as a first line therapy, peg-IFN alpha-2a (peg-IFN; 180 μg weekly for 48 weeks of treatment) and indefinite oral antiviral with either entecavir (0.5 mg daily) or tenofovir (300 mg daily) at different proportions for each defined cohort trying to simulate the current clinical practice. Oral antivirals (tenofovir-50% and entecavir-50%) was considered in 85% of patients already treated in each scenario for HBeAg- positive cohort, and in 95% of treated patients for HBeAg- negative population.Therefore peg-IFN represented 15% of therapies in HBeAg-positive treated patients, and 5% in HBeAg-negative population.
Analyses were separately performed for both, HBeAg- positive and HBeAg-negative cohorts.9
Transition probabilities
The health states included in the model (CHB, compensated cirrhosis, decompensated liver disease, HCC, transplant and death) were the commonly used to reflect the progression of disease’s natural history.8 , 11
One-year probabilities applied to simulate the evolution through these states were based on the virological response, depending on HBV DNA levels.11 Studies have shown that persistent reduction of serum HBV DNA below the lower limit of detection by real-time PCR assays is associated to biochemical remission, histological improvement and prevention of disease-related complications.12
For this reason, the original model8 was modified, including the potential regression of cirrhosis as have shown in long term studies with tenofovir (74%, at 5-years)13 and entecavir14 (Figure 1).

Failure, resistance and rescue therapies
Patients initially treated with peg-IFN who did not achive inmune control (HBV DNA < 2,000 IU/mL and normal ALT levels) after 48 weeks of treatment were retreated with oral antivirals (50% entecavir and 50% tenofovir). According to the literature, a first year antiHBe seroconversion of 32% was considered in HBeAg-positive patients treated with 48 weeks of peg-IFN.6 This seroconversion was maintained overtime in the 81% of cases15 given a lifetime adjusted seroconversion equal to 25.9%. In HBeAg-negative patients, 19% of them achieved serum HBV DNA levels < 60-80 IU/mL after 48 weeks of therapy,6 being a failure rate of 81%.
The antiHBe seroconversion rates6 , 16 in HBeAg-positive patients treated with tenofovir were 21% at year 1 of therapy,9 26% at year 3,17 and up to a maximum rate of 40% at year 7.18 The same rates were applied for entecavir in absence of long-term data in clinical trials (only results for 3 years of follow-up were identified). As recommended by guidelines, oral therapy was stopped 12 months after antiHBe seroconversion.6 The rate of HBsAg loss considered in HBeAg-positive cohort was 12%.18 No HBsAg loss was applied to HBeAg-negative patients. No resistance to tenofovir was considered based on the results published.19 A resistance rate of 1.2% at 5 years 20 was considered for entecavir. Patients with HBV resistant to entecavir were rescued by adding on tenofovir.
Treatment discontinuations
Treatment discontinuations for efficacy of oral antivirals were allowed for those HBeAg-positive patients achieving HBeAg loss and seroconversion to anti-HBe and also for HBeAg positive or negative who presented HBsAg loss.
No more discontinuations were applied further the 7 years mentioned period. After discontinuation, the patient's progression was equivalent to the natural disease.
Analysis
Expected outcomes were calculated in terms of survival, as well as the accumulated number of HCC cases at each patient cohort.
The cost-effectiveness results were expressed as incremental cost in euros, per survival increase measured as life year gained (LYG) and quality adjusted life years (QALY) gained.
QALY were derived from LYG, appliying different utility figures, obtained for each model health state.8
The model established the incremental cost-effectiveness ratio (ICER) for each one of the defined-antiviral strategies compared to the reference case (natural disease history). Additionally the ICER of strategy 2 compared to strategy 1 was calculated, to assess the influence to increase the treatment coverage from 71% to 100% of population.
Beyond the first year, an annual discount rate of 3% was applied to costs and health benefits to allow for time preference into current values.21
Costs
Only direct health care costs related to pharmaceutical and disease management costs8 were included in the analysis.
Drugs ex-factory prices for pharmaceutical costs calculation were taken from a national database,22 appliying the 7.5% mandatory deduction.23 Pharmaceutical costs calculations did not consider potential discontinuations due to adverse events.
Costs were expressed in euros (€, year 2014 values). Unitary costs were updated and inflated to 2014, when applicable, with Consumer Prices Index (Table 1).
Sensitivity analysis
Sensitivity analysis was performed to test the model’s robustness. Two alternative scenarios were defined: a fast and slow disease progression scenario. In the fast progression scenario, the base case transition probabilities were increased +10%, together with reduction of -10% of the cirrhosis regression rate. In the slow progression, transition probabilities decreased 10%, while cirrhosis regression rate increased its value +10%.
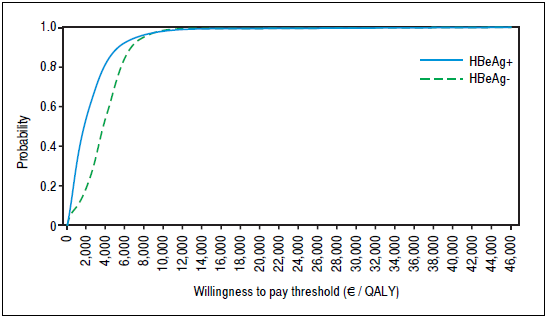
Probabilistic sensitivity analysis (PSA) was also performed through 1,000 iterations of a second order Monte- Carlo simulation. Beta distribution was applied to transition probabilities, and lognormal distribution was used for disease management costs, assuming a standard deviation of 10% from mean values. Results were plotted in a cost-effectiveness plane, and acceptability curves were constructed.
RESULTS
The results of the model showed that both treatment strategies resulted more effective than no therapy for both HBeAg-positive and HBeAg-negative populations.
Strategy 1 (treating 71% of population) increased patient survival, yielding 3.50 LYG and 3.98 additional QALY in HBeAg-positive cohort and 1.51 LYG and 2.16 additional QALY in HBeAg-negative cohort, compared to natural history. Strategy 2 (full treatment coverage) increased survival up to 4.93 LYG and 5.60 additional QALY and 2.13 LYG and 3.05 QALY gained for HBeAg-positive and -negative populations, respectively.
The avoided number of HCC cases also measured health benefits of antiviral therapies. For the study horizon, the model predicted 361 and 276 HCC episodes per 1,000 patients in HBeAg-positive and -negative populations. The strategy 1 (71% of treament coverage) reduced the number of HCC to 233 and 190 cases per 1,000 patients for HBeAg-positive, and HBeAg-negative populations, respectively (Table 2).
Table 2 Accumulated number of HCC per 1,000 patients over time.
Strategy 1: 71% treated patients. Strategy 2: 100% treated patients.
The overall estimated total costs for untreated were €96,555 in HBeAg- positive and €66,527 in HBe Ag-negative cohort.
Total cost increased up to €102,841 and €105,408 for strategy 1 (71% of treatment coverage) and strategy 2 (100% of treatment coverage) in HBeAg-positive population. The estimated ICER was €1,581 per QALY gained vs. the natural history for both scenarios.
In HBeAg-negative population, total costs accounted €85,858 for strategy 1 with 71% of treatment coverage and €93,754 for strategy 2 with 100% of treatment coverage. The ICER resulted €8,942 per QALY gained with any of the treatment strategies assessed compared to the natural history used as reference.
The treatment strategies assessed yielded ICER below the threshold used in most (66%)24 of the economic evaluations performed for Spanish setting (€30,000/QALY), therefore could be considered as cost-effective alternatives compared to no treatment. Detailed values are shown in table 3.
Table 3 Base case cost-effectiveness results.
Strategy 1: 71% treated patients. Strategy 2: 100% treated patients. LYG: life year gained. QALY: quality adjusted life year. ICER: incremental cost-effectiveness ratio.
The estimated ICER decreased, in both HBeAg-positive and -negative cohorts, in the slow disease progression scenario tested, and increased in the fast disease progression analysis up to €1,761 per QALY gained and €8,104 per QALY gained in HBeAg-positive and -negative cohorts, respectively (Table 4).
Table 4 Sensitivity analyses results. Alternative scenarios with fast and slow disease progression.
Strategy 1: 71% treated patients. Strategy 2: 100% treated patients. LYG: life year gained. QALY: quality adjusted life year. ICER: incremental cost-effectiveness ratio.
In PSA including 1,000 Monte Carlo iterations, all the treatment strategies resulted cost-effective compared to reference case in 99.6% and 99.9% of simulations for any threshold higher than€15,000/QALY in HBeAg-positive and -negative cohorts, respectively (Figure 2).
DISCUSSION
The present findings show that with the current treatment rate in clinical practice there a reduction in the numer of HCC and an increase in survival. However, higher treatment coverages on populations were associated to better effectiveness estimates in both HBeAg-positive and - negative populations. Higher benefits in terms of preventing HCC cases were also observed, approximately 180 HCC cases per 1,000 inhabitants could be prevented in HBeAg-positive cohort with a full treatment coverage and up to 121 HCC cases per 1,000 inhabitants in HBeAg-negative cohort.
Efficiency of antiviral strategies compared to the scenario of the disease natural history without treatment was demostrated and are consistent with those reported by other authors which explored the cost-effectiveness of antiviral strategies in HBeAg-positive and HBeAg-negative cohorts in European population.25 The increase of the treatment coverage from 71% up to 100% was associated to better effectiveness estimates (higher survival and less HCC cases over time) at the same cost-effectiveness ratio, for both patients cohorts, HBeAg-positive and - negative.
Apart from the inherent limitations to any modelling study, some of them directly related to heterogenous profile of the CHB, that avoid capturing the full dynamic aspect of the disease, even in a rigoroulsy performed mathematical model, the following limitations are worth mentioning:
The cost of different CHB stages was obtained from published sources8 and could slighty differ from the present patient management, which could include novel treatments as sorafenib and new diagnostic techniques as FibroScan. However, no large variations are expected to occur over results if these values are modified.
In contrast with European guidelines,16 the current Spanish recommendations30 do not consider peg-IFN therapy for HBeAg-negative patients. In the present analysis a 3.5% was applied in order to capture the most reliable scenario across Europe.
One of the main novelties of the present model is that in contrast to the original one,8 it included regression of cirrhosis cases based on the available evidence that have demonstrated its ocurrence in patients achieving sustained virological response after long-term oral antiviral therapy.
The rates applied in the model (74% of cirrhosis regression at 5 years) corresponded to tenofovir,13 because, although a similar phenomenon seems to happen also following entecavir treatment,14 the reduced sample of cirrhotic patients in the studies avoided calculation of a regression rate.
Derived from published series, the HCC accumulated ratios at approximately 5-years of follow-up period, could be established from 6% to 19% for not treated populations, 2%26 to 16%27 in interferon treated patients, and 0.7%28 to 6.6%29 for oral antiviral therapies.
The design of the current model does not allow the distinction between pegylated interferon and oral antiviral, but the projected HCC incidences do not differ much more from the values here above mentioned, and are among the wide intervals showed. The estimated accumulated incidence of HCC at 5-years resulted around 7.6% in HBeAg-positive and 38% in HBeAg-negative populations for no treated patients. Incidences as low as 0.1% and 0% (for HBeAg- positive and HBeAg-negative cohorts, respectively) were observed following any treatment strategy. In line with conclusions from a recent review of the long-term efficacy of antiviral treatment in the prevention of HBV-related HCC30 the results from the present model confirmed the protective effect in lowering the risk of HCC development with the assessed treatment strategies.
Durable HBeAg seroconversion is an important therapeutic endopoint, associated to better outcomes.31 This effect was included in the the model, allowing patients to discontinúate the treatment. Adittionally to the associated reduction in total cost due to the lower drugs consumption over long time, there are other benefits difficult to quantify, in terms of patient quality of life that should be kept in mind.
The results from the sensitivity analyses confirmed robustness of the assumptions and the model.
The external validity of the results, in terms of transferability to other settings, particularly to routine clinical practice derives directly from the potential differences in patient management. These outcomes apply to Spain, should be precautionary interpreted in regard to a potential extrapolation to a different setting.
Cost-effectiveness of CHB antiviral therapies have been examined by differents studies. Comparisons of cost estimates obtained from these studies are often difficult, due to differences on methodology (comparators, time horizon, perspective, year of analysis) and heterogeneity of populations. However, entecavir and tenofovir seem to be cost-effective interventions for the treatment of patients with CHB in many health systems 32
The current analyses aimed to estimate preventable burden of CHB, by means of establishment of available antiviral therapies. Any effort conducted to increase the treatment antiviral coverage in CHB populations, both HBeAg-positive and -negative would be accompanied by the long-term reduction of the CHB complications, as HCC cases mainly.
In conclusion, antiviral therapy must be a generalized option in CHB infected patients. Based on the present results any campaign designed to increase the coverage of treatment in CHB patients, would be efficient and should be encouraged in order to improve health benefits in infected patients, in terms of survival, and by reduction of HCC cases.
ABBREVIATIONS
CHB: |
Chronic Hepatitis B. |
EASL: |
European Association for the Study of the Liver. |
HBV: |
Hepatitis B virus. |
HCC: |
Hepatocellular carcinoma. |
ICER: |
Incremental cost-effectiveness ratio. |
LYG: |
Life year gained. |
Peg-IFN: |
Pegylated interferon. |
PSA: |
Probabilistic sensitivity analysis. |
QALY: |
Quality adjusted life year. |

