











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Early-onset infantile-juvenile scoliosis in children < 10 years of age may be a sign of suspected neuraxial disorder. In 504 patients, the incidence was 18.7%, while Chiari malformation, with or without syringomyelia, accounted for 64.8%. Moreover, in males, the left thoracic and right lumbar curves were significantly associated with neural axis anomalies, a finding detected by magnetic resonance imaging (MRI)1. Therefore, it is justifiable to request this study in patients with apparently idiopathic scoliosis with these characteristics.
Chiari malformations are characterized by different degrees of descending herniation of the cerebellar tonsils, brainstem, and IV ventricle into the spinal canal1. The prevalence of this malformation is 1/1000 live births and, in many cases, it is associated with other anomalies such as myelomeningocele (88%), syringomyelia (45-75%), hydrocephalus (3-10%) and Klippel-Feil syndrome2.
Idiopathic infantile-juvenile scoliosis was associated with intraspinal neural axis anomalies with a prevalence of 11.1-26%, according to a study with a limited sample size3.
Clinical case
We describe the case of a 6-year-old patient who consulted his primary care physician for postural lateralization and left gait. Born prematurely at 31 weeks of gestation, he showed a small cyst located in the right lenticular thalamic sulcus, suggestive of traces of germinal matrix hemorrhage grade I in regression. Although he was under follow-up by the occupational therapy area for attention deficit and motor tics, he showed no other relevant personal or family history.
Physical examination identified a good general condition, with left convergent strabismus, preserved ocular mobilization, reactive and symmetrical pupils of intermediate size, and preserved cranial nerves. The patient had a left-lateralized posture with left shoulder droop (Figure 1), with dextroconvex scoliosis temporarily corrected with assisted positioning, strength 4/5, patellar osteotendinous reflexes 2/4, cutaneous plantar flexor reflexes and the rest of the neurological examination was normal. The initial spinogram detected the presence of scoliosis with a calculated initial angle of 37° (Figure 2).


Figure 2 Pre-surgical spinogram. Pre-surgical scoliotic curvature is marked (orange) with a Cobb angle of 37°.
We requested the evaluation by pediatric neurology and traumatology services. These services found that the patient presented axial lateralization to the left (Figure 2), with a symmetrical tone, volume, muscle mass, and strength, and 2/4 bicipital and patellar reflexes. Painless asymmetry at the level of the shoulder girdle was significant. We decided to request a brain and spine MRI due to suspicion of scoliosis secondary to neuroanatomical alteration. MRI showed a descent of the cerebellar tonsils to C2 (22 mm) (Figure 3), associated with extensive syringomyelia about 14.8 mm of the spinal cord (Figure 4), confirming the diagnosis of Chiari malformation type I. Consequently, a suboccipital craniectomy plus C1 craniectomy with duraplasty was promptly scheduled.

Figure 3 T1 MRI showing 22 mm tonsillar herniation (vertical line in green) from the foramen magnum (horizontal line in green).
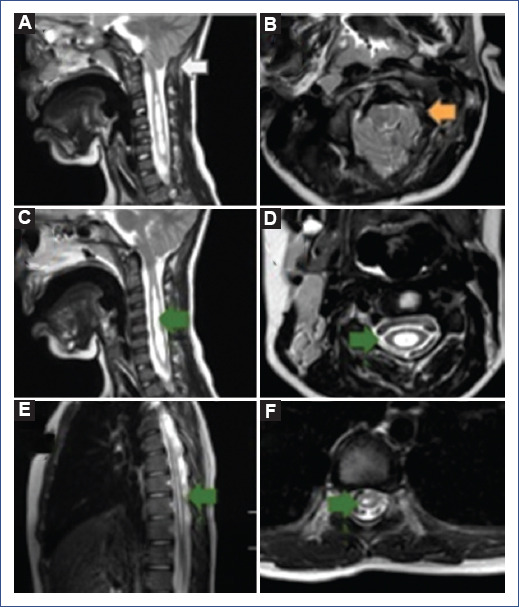
Figure 4 Cervico-dorsal MRI without contrast: sagittal and axial slices are shown. A-B: sagittal and axial slices at the level of the occipital-cervical hinge; a 22 mm tonsillar descent is seen (white arrow), with a decreased content-continent ratio at the level of the foramen magnum (orange arrow). C-D: sagittal and axial view at the cervical level showing syringomyelic cavity (green arrow), extending to dorsal regions. E-F: sagittal and axial sections at the dorsal level.
Fifteen days after the Chiari malformation corrective surgery, the patient developed meningitis and was hospitalized for intravenous treatment, with good evolution and resolution.
The patient evolved with no post-surgical complications and presented a reduction of the syringomyelic cavity (5 mm) one month later. However, scoliotic posture persisted with a final angle of 31° (Figure 5), for which a thoracolumbosacral orthosis (TLSO) was indicated. The clinical, neurology, ophthalmology, and pediatric traumatology teams are currently following up with the patient.

Discussion
As early-onset infantile-juvenile scoliosis in children < 10 years of age may be a suspicious sign of neuroaxis alteration1, it is important to perform a brain and spine MRI in these cases.
Only 15% of the cases of infantile-juvenile scoliosis (3-10 years) are idiopathic, increasing to 80% in adolescence. In males (37% vs. 8% in females), left thoracic1,4 and right lumbar curves are significantly associated with neural axis anomalies on MRI1. In pediatrics, MRI in cases with suspicious signs has led to detecting a higher precentage of neurological alterations (4-26%)3 in cases initially labeled as idiopathic. Syringomyelia and Chiari's malformation are the most frequent findings in patients with little evident clinical manifestations5,6.
Other pathologies associated with scoliosis are myelodysplasia (thoracic level), traumatic paralysis (< 10 years of age) in 100%, Friedreich's ataxia, and cerebral palsy with four limbs involved in 80% of cases5.
In 2016, a study of 188 patients with early-onset scoliosis found that 94 patients (18.7%) had a neural anomaly: Chiari malformation (43 patients), Chiari malformation combined with syringomyelia (18 patients), isolated syringomyelia (13 patients), diastematomyelia (six patients), tethered cord combined with diastematomyelia (six patients), tethered cord (four patients), and other rare intraspinal abnormalities (four patients). Total Chiari malformation with or without syringomyelia accounted for 64.8% (61/94) of these anomalies. In addition, left thoracic7-9 and right lumbar curves in males were significantly associated with neural axis anomalies on MRI3.
Cranioencephalic disproportion with a very small posterior fossa relative to its contents explains why the treatment of choice should be posterior fossa decompressive surgery with or without duraplasty1,10,11.
Chianti malformation is classified into four types (from 0-IV): type I is defined as the descent of the cerebellar tonsils > 3-5 mm below the level of the foramen magnum; consequently, a cranioencephalic disproportion where there is a very small posterior fossa in relation to the contents is observed. Chianti malformation type I is the most prevalent (6/10,000 cases), where the tonsillar herniation is > 3 mm, although the degree of herniation is not related to the severity of the condition. This herniation into the spinal canal causes alterations in cerebrospinal fluid (CSF) circulation, which explains why Chiari malformation is an important cause of syringomyelia4 and is observed in 55-75% of all cases. It has also been documented in 3-10% of cases of the communicating type, in 27% of pediatric age (cervical monosegmental or extended type), and in 57% of cervicodorsal (C8-Dl).
Clinically, the diverse manifestations may be associated with alterations in CSF circulation and compression of nerve structures.
Syringomyelia has a progressive course with worsening symptoms over time. Therefore, early diagnosis is essential to promote a favorable course and prevent the progression of damage to the central nervous system.
Surgery is the only treatment option. Any patient with symptomatic or asymptomatic syringomyelia should be treated by decompressive surgery of the posterior fossa with or without duraplasty10-12.
Surgery with dural opening and plasty, as performed in our patient, is possibly the option that best resolves the symptoms and allows less progression of the scoliotic curve, especially in children < 10 years of age, with improvement in 38%, stabilization in 38%, and worsening in 23%13 with less neurological sequelae.
As a result of the intervention, 80% of patients resolve the syringomyelic cavity, and 20% show marked neurological improvement, while 25-30% remain stable one year after surgery10,13. However, the optimal treatment for this condition is still controversial. In 2008, a study comparing patients who underwent posterior fossa decompression surgery with or without duraplasty, found better clinical and radiological results3,10 and a lower rate of reoperations in those with duraplasty. However, duraplasty presents a higher risk of postoperative complications, such as CSF fistulas or meningitis, as in our patient, due to postoperative inflammatory collections10,11,13,14.
Although surgery is a palliative treatment option, it should be noted that scoliosis as a comorbidity implies a new therapeutic approach, as in the present case, in whom an orthopedic brace was implemented. The use of bracing is less effective in neuromuscular scoliosis than in idiopathic scoliosis, so it can be considered when the skeleton has not yet reached maturity (Risser 0, 1, or 2) and when the Cobb angle is > 20°. However, the purpose of bracing is to halt the progression, not to correct it definitively. The recovery and rehabilitation stage is critical for patients to continue their daily activities and ensure adequate neuromuscular development and harmonious social and family integration.
On this basis, early-onset scoliosis should raise a high index of suspicion of association with neuro-spinal diseases. In this context, syringomyelia associated with Chiari malformation is uncommon, but its timely management may decrease the progression of associated comorbidities.

