











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Pediatric surgery in America began in the early 20th century, when the surgical diseases of newborns forced a group of surgeons to devote themselves exclusively to the care of children. However, neonatal surgery really started when the first neonatal surgical unit was established in Liverpool in 19531-4. Neonatal surgery is the most demanding and specialized field of pediatric surgery due to these patients´ unique physiological, anatomical, and biochemical characteristics5.
Over the years, with advances in neonatal intensive care, we have seen an improvement in the survival of neonates with smaller gestational ages and more challenging and complex clinical conditions6,7. It is well known that pediatric patients are not little adults, and this is especially true for neonates, who require facilities designed specifically for them8.
In 1967, the "Hospital de la Mujer" was inaugurated, which later became the Hospital de Ginecología y Obstetricia (HGyO) of the Instituto Materno Infantil del Estado de México (IMIEM), the first hospital in Toluca to provide specialized care for the mother-child binomial. Since 2011, this hospital has had a pediatric surgery service9, joining the maternity hospitals that provide surgical management within their facilities, being a pioneer in the State of Mexico. It currently has 75 beds, divided into the neonatal intensive care unit (NICU), Infectious Diseases, Metabolic Disorders, Transitional Care, Growth and Development, and the Surgical Unit. In terms of human resources, it has a staff of 27 specialists in neonatology and a pediatric surgeon. It has the peculiarity of not accepting outpatients, so all the newborns that undergo surgery are those born in the same facilities.
Neonatal surgery is divided into surgery for congenital malformations and surgery for acquired conditions secondary to complications of prematurity or prolonged hospitalization10. It is important to know the casuistry of neonatal surgical diseases in one of the oldest perinatal hospitals in the most populated state of Mexico. This study aimed to describe the 10-year experience of surgical management of patients treated at the Neonatal Service of the HGyO of the IMIEM.
Methods
Study design
We conducted a descriptive, observational, cross-sectional, and retrospective study in the Neonatal Service of the HGyO of IMIEM, Toluca, State of Mexico.
Population
Patients who underwent surgery at the HGyO by the Pediatric Surgery Service between August 01, 2012, and July 31, 2022, were included in the study. Patients who underwent surgery outside the hospital facilities were excluded. Patients with incomplete information in their records were eliminated. Procedures such as circumcision, catheter placement, paracentesis, peritoneal or chest tube placement were not included in the study.
Variables
The following variables were analyzed: age and weight at the time of surgery, sex, gestational age in weeks (wg), prenatal diagnosis, surgical diagnosis, procedure performed, anatomic region intervened, type of surgery (emergency or planned, time elapsed from diagnosis to surgery, and NICU stay), type of pathology (congenital or acquired) and mortality.
Emergency surgery was considered as a procedure performed immediately because the neonate´s life or organ function was at risk. Programmed surgery was considered a procedure performed when, despite the nosologic process, the neonate´s hemodynamic, respiratory, and target organ conditions remained stable according to the disease, allowing the optimal moment for surgical intervention to be sought. Data were obtained from the Pediatric Surgery Service database and the patient´s clinical records.
Statistical analysis
Descriptive statistics were reported as frequency, central tendency, or dispersion measures, depending on the variable type. For inferential statistics, comparisons were made using the χ2 test or Fisher´s exact test for qualitative variables and Student´s t-test and ANOVA for quantitative variables. Data were processed using SPSS software version 25 and Excel version 1811. The study was approved by the Bioethics and Teaching and Research Committee of the HGyO of the IMIEM.
Results
Prevalence and patient characteristics
Over a 10-year period, from 2012 to 2022, the mean number of births in the HGyO was 99,946. A total of 551 patients underwent surgery during this period, with a prevalence of 0.5%. The distribution of the number of surgeries per year is shown in figure 1. There is an upward trend of 2.7 cases per year in the number of cases treated during the study period and projected growth of 72 cases per year in 2025, with a model r2 = 0.66 and p = 0.02. Demographic and clinical characteristics of the neonates who underwent surgery are shown in table 1. Overall, the mean gestational age was 36 weeks (range 26-42.3 wg), with only 47.2% term neonates; the mean weight was 2370 g (range 580-4800 g), with the patients divided as follows: 24 neonates (4.4%) < 1000 g, 64 (11.6%) between 1000 and 1500 g, 226 (41%) between 1500 and 2500 g, 203 children (36.8%) between 2500 and 3500 g, and 34 (6.2%) > 3500 g.
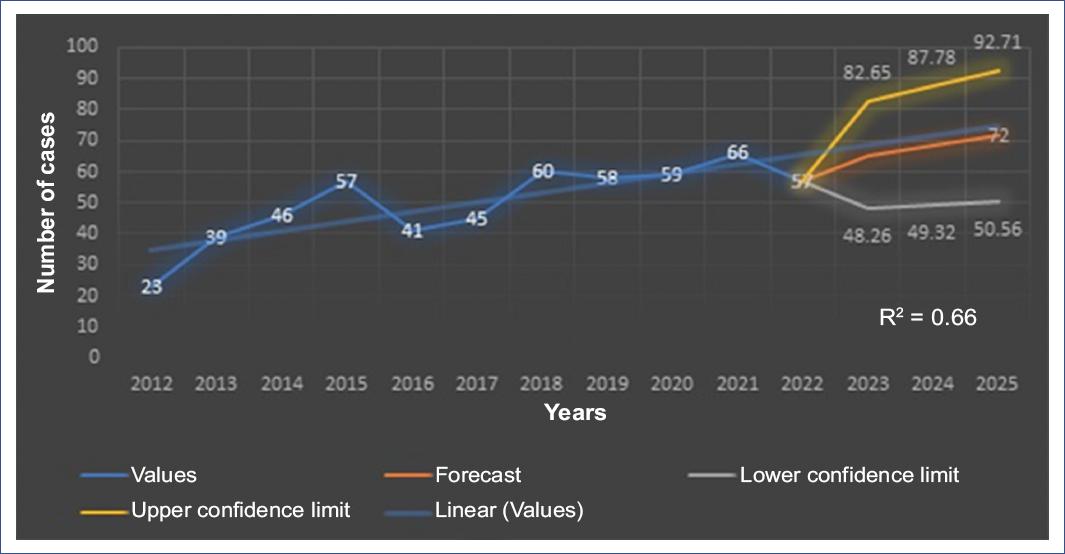
Table 1 Demographic and clinical characteristics of patients according to gestational age
| Variable | Weeks of gestation | Total | p | ||
|---|---|---|---|---|---|
| ≤ 28 | 29-36.6 | ≥ 37 | |||
| Number of cases, n (%) | 20 (3.6) | 271 (49.2) | 260 (47.2) | 551 (100) | < 0.001 |
| Age at the time of surgery (days), mean (SD) | 29 (23.9) | 17 (16) | 13 (14.6) | 15.6 (16) | < 0.001 |
| Weight at the time of surgery (g), mean (SD) | 1672 (721) | 2025 (652) | 2784 (644) | 2370 (761) | < 0.001 |
| Female, n (%) | 9 (45) | 136 (50.2) | 113 (43.5) | 258 (46.8) | 0.304 |
| Prenatal diagnosis, n (%) | 0 (0) | 48 (17.7) | 64 (24.6) | 112 (20.3) | < 0.001 |
| Surgical emergency, n (%) | 6 (30) | 106 (39.1) | 83 (31.9) | 195 (35.4) | 0.200 |
| Congenital pathology, n (%) | 10 (50) | 177 (65.3) | 187 (71.9) | 374 (67.9) | 0.069 |
| Region operated, n (%) | |||||
| Gastrointestinal | 12 (60) | 196 (72.3) | 190 (73.1) | 398 (72.2) | 0.188 |
| Genitourinary | 4 (20) | 42 (15.5) | 24 (9.2) | 70 (12.7) | |
| Thoracic | 3 (15) | 29 (10.7) | 38 (14.6) | 70 (12.7) | |
| Cervical | 1 (5) | 4 (1.5) | 8 (3.1) | 13 (2.4) | |
| Mortality, n (%) | 4 (20) | 40 (14.8) | 13 (5) | 57 (10.3) | 0.001 |
SD: standard deviation.
The mean age of the neonates at the time of surgery was 15.6 days, and 438 (79.5%) of the patients underwent surgery within the first month of life. Adjusting for gestational weeks in preterm infants, 497 (90.1%) patients had surgery in the neonatal period.
Identified diseases and prenatal diagnosis
A total of 48 conditions were identified in patients who underwent surgery, classified as congenital and acquired (Figs. 2 and 3 show the number of cases for each diagnosis, and table 2 shows their prevalence). During the 10-year period covered by the study, there was an increase in the presentation of omphalocele, annular pancreas, esophageal atresia, and necrotizing enterocolitis (NEC), with a marked decrease in the number of cases of intestinal atresia.

Figure 2 Congenital pathologies and prenatal diagnosis. ARM: anorectal malformation. Other: includes 17 pathologies with low presentation: cloacal malformation, adenomatoid cystic disease, diaphragmatic eventration, ovarian cyst, ductus arteriosus, hiatal hernia, lymphatic malformation, biliary tract atresia, pulmonary sequestration, renal cystic disease, phimosis, hepatic hemangioma, hydronephrosis, laryngomalacia, bronchogenic cyst, common bile duct cyst and mesentery cyst.

Table 2 Frequency and prevalence of main pathologies
| Number | ICD-11 | Diagnosis | Frequency (%) | Prevalence |
|---|---|---|---|---|
| 1 | LB17.0 | Anorectal malformation | 58 (10.5) | 5.8 |
| 2 | LB15.1 | Intestinal atresia | 54 (9.8) | 5.4 |
| 3 | LB02 | Gastroschisis | 52 (9.4) | 5.2 |
| 4 | DD51 | Inguinal hernia | 50 (9) | 4.9 |
| 5 | KB88 | Necrotizing enterocolitis | 30 (5.4) | 2.7 |
| 6 | KB80 | Swallowing impairment/GERD | 28 (5.1) | 2.7 |
| 7 | LB12.1 | Esophageal atresia | 27 (5) | 2.7 |
| 9 | DD50 | Diaphragmatic hernia | 21 (3.8) | 2.1 |
| 10 | KB86.Y | Spontaneous intestinal perforation | 13 (2.3) | 1.3 |
| 11 | LB21.0 | Annular pancreas | 12 (2.1) | 1.1 |
| 12 | LB01 | Omphalocele | 12 (2.1) | 1.1 |
| 13 | LB12.3 | Esophageal stricture | 11 (1.9) | 1 |
| 14 | KB2Y | Subglottic stenosis | 10 (1.8) | 1 |
Total births: 99465. Source: SINAC/SINBA. GERD: gastroesophageal reflux disease; ICD: international classification of diseases.
Of the surgical procedures performed, 195 (35.3%) were for acquired pathologies, and 356 (64.6%) were for congenital conditions; of the latter, only 144 (40.5%) had a prenatal diagnosis. Duodenal obstruction was the most common diagnosis in more than 70% of cases, followed by diaphragmatic hernia and abdominal wall defects. Percentages are shown in figure 2.
Surgical care and NICU stay
In congenital pathologies with prenatal diagnosis, the mean time elapsed from birth to the time of surgery was 3 days, and with no prenatal diagnosis, 3.6 days (p = 0.07). In the case of acquired pathologies, the mean time from diagnosis to surgery was 5.1 days. For programmed surgeries, the mean time was 5.4 days.
In terms of length of stay in the NICU, the mean was 18.9 days for all pathologies. When differentiating between planned and emergency surgery, the mean was 18.4 and 19.7 days, respectively (p = 0.376). Regarding the difference between congenital and acquired pathologies, we found a mean NICU stay of 14.9 days for the former and 27.3 days for the latter (p < 0.05). We found no statistically significant differences between NICU stay and gestational age of the patients, with a mean of 21.5 days for those < 28 wg, 18.2 for neonates between 29 and 36.6 wg, and 19.4 for those > 37 wg. However, diagnosis-to-surgery time and NICU stay had highly variable results depending on the pathology involved (Table 3).
Table 3 Evolution and mortality of the main pathologies
| Diagnosis | Diagnosis - surgery time (days) | NICU stay (days) | Mortality n (%) |
|---|---|---|---|
| Anorectal malformation | 2.5 | 14 | 3 (5.1) |
| Intestinal atresia | 2.3 | 18.6 | 8 (14.8) |
| Gastroschisis | 1.7 | 22.6 | 8 (15.4) |
| Inguinal hernia | 6.4 | 0.6 | 0 (0) |
| Necrotizing enterocolitis | 1.8 | 24.2 | 8 (26.7) |
| Swallowing impairment/GERD | 8.9 | 49.8 | 1 (3.6) |
| Esophageal atresia | 5.9 | 24.2 | 8 (29.6) |
| Diaphragmatic hernia | 7.1 | 20.1 | 3 (14.2) |
| SIP | 1.7 | 23.9 | 3 (23.1) |
| Annular pancreas | 2.8 | 16 | 0 (0) |
| Omphalocele | 4.5 | 25.5 | 2 (16.7) |
| Esophageal stricture | 4.3 | 41.1 | 1 (9.1) |
| Subglottic stenosis | 10.1 | 64.9 | 1 (10) |
GERD: gastroesophageal reflux disease; NICU: neonatal intensive care unit; SIP: spontaneous intestinal perforation.
Surgeries performed
Most of the surgeries were performed on the gastrointestinal tract, with 398 cases (72.2%), followed by the genitourinary tract and the thoracic region, with 70 patients each (12.7%), and finally the cervical region with 13 patients (2.4%) (Fig. 4).

Figure 4 Surgical procedures performed. Others: include 36 more procedures, which were grouped due to their low frequency, as follows: esophageal plasty, silo placement, tracheostomy, umbilical plasty, peritoneal dialysis catheter placement, esophageal elongation, ligation of ductus arteriosus, nephrectomy, lobectomy, pneumonectomy, pyloromyotomy, among others.
Survival
In-hospital survival of neonatal surgical patients was 89.7%. Among the 57 patients who died (10.3%), there was a steady decrease in mortality with increasing weight at the time of surgery, with those over 2500 g having the best survival. Seventy-seven percent of deaths occurred in preterm patients (< 37 wg). About 57.9% of mortality occurred in patients with congenital malformations and 72% in neonates requiring emergency surgery. In the bivariate analysis between mortality and associated factors, we found statistical significance for weeks of gestation, weight, type of surgery, time from birth or diagnosis to surgery, and days of stay in the NICU (Table 4).
Table 4 Mortality analysis
| Variable | Mortality n (%) | p |
|---|---|---|
| Weeks of gestation | 0.001 | |
| ≤ 28 | 4 (20) | |
| 29-36.6 | 40 (14.7) | |
| ≥ 37 | 13 (5) | |
| Sex | 0.78 | |
| Female | 28 (12.1) | |
| Male | 29 (9.8) | |
| Weight (g) | < 0.001 | |
| ≤ 1500 | 23 (26.1) | |
| 1500-2500 | 20 (8.8) | |
| ≥ 2500 | 14 (5.9) | |
| Prenatal diagnosis | 0.21 | |
| Yes | 9 (8) | |
| No | 21 (12.8) | |
| Type of surgery | < 0.001 | |
| Urgent | 41 (21) | |
| Scheduled | 16 (4.5) | |
| Type of pathology | 0.062 | |
| Congenital | 33 (8.8) | |
| Acquired | 24 (13.5) |
Concerning mortality and its distribution according to the disease, the pathologies that did not present mortality were diaphragmatic eventration, pulmonary sequestration, bronchogenic cyst, cystic adenomatoid malformation, duodenal atresia, annular pancreas, and intestinal volvulus. Mortality was distributed as follows: NEC, intestinal atresia, esophageal atresia, and gastroschisis with 14% each, spontaneous intestinal perforation with 5.3%, anorectal malformation with 5%, and omphalocele with 3.5%; the remaining 30% was distributed among 13 different diseases.
Patients who died spent an average of 24.3 days in the NICU, compared to 18.2 days for survivors, showing a statistically significant difference (p = 0.007). The total annual mortality is shown in figure 5, with a decreasing trend of 0.7% per year from 2012 to 2022; we can also see the mortality projection for 2025, which will be 5% if the same trends continue, with an r2 of the linear regression model of 0.51 and p = 0.013.

Discussion
Neonatal surgical practice is a specialized area of pediatric surgery due to the complexity of patients during this critical period of life. Care after these high-risk surgeries requires a qualified hospital where the number of procedures and the care team are essential for optimizing outcomes, maintaining the quality of care, and conducting research11,12. Our NICU has a technical infrastructure that has allowed neonatal surgical management for more than 10 years. In our hospital, we have found that six out of 1000 patients require surgical management, similar to the classic reports of Rickham (1:200 neonates) and much higher than the results of Riquel et al. (1:600) in their 10-year study13. Our prevalence of 0.5% of surgical cases is relevant because this is not a referral center, treats only patients born in its facilities, and has only one specialist in pediatric surgery. Even under these conditions, an average of one neonatal surgical case per week has been performed over the past 10 years, in addition to minor procedures such as thoracentesis, pleurostomy, peritoneal drains, paracentesis, circumcisions, and placement of central venous access, among others, which are not included in the study.
In our casuistry, we found that patients with < 37 wg represented 52.8% of the cases and those weighing < 2500 g represented 57%, so our patients had lower weight and gestational age compared to the average of other international reports14-16. This increases the need for pre-operative, intraoperative, and post-operative care and indirectly indicates our units high level of neonatal care.
Surgical interventions in the early stages of life can be due to congenital or acquired pathologies; 32.1% of our cases were acquired pathologies, consistent with other reports17,18 that establish that the main causes of surgical interventions in the neonatal stage are congenital diseases. In Mexico, approximately one in 50 live births have a major malformation that limits functionality and threatens life12. In IMIEMs HGyO, we found four cases of major congenital malformations per 1000 live births, lower than the national reports, which are between 7 and 8.4: 1000 live births19,20. This finding could be influenced by the fact that we are not a referral hospital and that we only report in the casuistry the malformations that are of interest and that have been addressed by the pediatric surgeon.
Diagnosing congenital pathologies before the patients birth is an advantage for postnatal care, so it should be the norm. In the 20-year study by Yagi et al., prenatal diagnosis was reported in 34.9% of cases16; in comparison, we obtained prenatal diagnosis in 40.5% of cases. We still consider this percentage to be low because not having this diagnosis increases the patients risks, making it difficult to plan their care and provide prenatal counseling to the family member. Therefore, in our environment, it is a priority to improve prenatal control, and ideally, as mentioned by Benachi and Sarnacki, there should be an active collaboration between obstetrician-gynecologists and pediatric surgeons21.
The diversity of pathologies found in our study is relevant since, in general, it almost duplicates that found in other national and international reports13,15-18,20,22,23. This diversity allows to maintain an adequate practice in the medical and surgical care of all these diseases, having in this aspect a considerable strength in our hospital. For example, we coincide in six of the first seven most common diagnoses found in the Latin American Collaborative Study of Congenital Malformations (ECLAMC, by its Spanish acronym)24.
Concerning the time elapsed from diagnosis to surgery, there was a wide variation according to the emergency status and surgical diagnosis, as shown in table 3. In general, few procedures require immediate intervention, and in most cases, the first hour of life is used to perform the study protocol and stabilize the patient. This was the case even in congenital pathologies already diagnosed prenatally, where the average intervention time was 3 days. We found an enormous variation according to the pathology; for example, in gastroschisis, the intervention was performed in the first minute of life, and diaphragmatic hernia, where we waited several days for the hemodynamic and ventilatory stabilization of the neonate. The pathologies that were operated on most quickly were intestinal volvulus, gastric perforation, gastroschisis, spontaneous intestinal perforation, and NEC, with an average of 1.5 days. This period, rarely mentioned in studies, has a direct impact on the evolution of the patient, indicating the quality of the pre-operative preparation and the prompt availability of surgical care. In our case, by not receiving transfer patients, we were able to provide timely care to the newborn, and positive impact on the results.
Few reports have analyzed the length of stay in the NICU for surgical patients. Siddharth et al. reported a mean of 13.8 days15 and Saggers et al. 13 days18, durations significantly lower than those in our study (18.9). However, in our hospital, the NICU stay is not only related to the surgical diagnosis and the health status of the patient but also to external causes, such as the availability of places in intermediate therapy. Therefore, the figure we obtained may not be a reliable parameter of the patient´s evolution. There was a significant difference in the length of stay in the NICU between congenital and acquired pathologies, which could be because these diseases occur as a consequence of prematurity and prolonged hospitalization, such as NEC, swallowing, and suckling disorders, esophageal stenosis, chemical peritonitis due to umbilical catheter dysfunction, subglottic stenosis, and renal failure, among others.
One indicator of the quality of care in a NICU is the neonatal surgical mortality rate, which is closely related to a country´s economic development, being seven times higher in low socioeconomic countries than in developed countries25. Our overall mortality rate was 10.3%, which is within the international average but higher than that reported in developed countries such as the United States (4%), Japan (6.6%), and South Korea (6.7%) and lower than countries such as India (35%) and Nigeria (45%)16,26; in terms of previous national studies, our results are lower than the 33% reported by Rodriguez et al.20
The percentage of neonatal deaths attributable to congenital anomalies, many of which are correctable by surgery, is increasing. They also represent a significant financial burden and public health problem27,28. Our mortality rate for surgical congenital anomalies was 0.3/1000 live births, which is lower than the mortality rate reported in Mexico for patients with these anomalies (whether or not they have undergone surgery), which is 2:100029. Similarly, reports from the Instituto Mexicano del Seguro Social and the Instituto Nacional de Perinatología describe congenital anomalies as one of the top five causes of neonatal death30,31.
Mortality in our study varied widely, as shown in table 3, but for most diseases, the proportions were similar to those reported internationally16-18,32,33. In addition, there was a general downward trend over the 10 years of the study. This decrease was mainly observed in NEC, which reached a peak mortality of 28% and decreased from 2018 when we started early surgical intervention protocols for this disease. The only pathologies with a higher mortality in our hospital were esophageal atresia and gastroschisis, which is a call to review our care protocols for these diseases.
Within our bivariate analysis of mortality, we found an inverse relationship between mortality - weeks of gestation and patient weight, consistent with international reports16,28. However, unlike countries with high resources, our mortality in neonates under 30 wg and 1500 g who required surgery was almost 6% higher. Thus, it is essential to maintain multidisciplinary management, constant development, and technological updating of the NICU, to have better viability in the premature patient. Another variable with significant relationship with patient mortality was the emergency surgery, which presented almost five times more deaths than scheduled surgery. Therefore, our priority is to conduct prospective studies to determine whether this is due to the conditions of the critically ill patients or whether there is an extrinsic part that could be improved in the perioperative multidisciplinary care. Concerning the time patients remained in the NICU, we found a progressive increase in mortality as the surgical neonates remained longer in the NICU, with 63.2% of the total mortality in patients who remained longer than 21 days, suggesting that the critical condition of a neonate warranting a stay in the NICU is a determining factor of survival. Conversely, we did not find statistical significance in the difference in mortality between patients with or with no prenatal diagnosis, either in general or specifically by pathology, even though the neonates who had prenatal diagnosis had earlier surgery.
Among the factors that influence the survival of our patients, it is important to emphasize that we only care for patients born in our unit. This avoids transfers that could destabilize the high-risk neonate, reduces the time of care, and limits the pathogenic organisms that could enter our unit, reducing sepsis events. There are studies suggesting that the surgeon´s experience impacts mortality, which is 12% higher when the procedure is performed by a physician with less experience, with a relative risk of 1.534,35. In our study, the fact that all surgical care is provided by a single pediatric surgeon with more than 10 years of experience in neonatal surgical care and that there are no residents may be an advantage. All of the above undoubtedly contribute to improving the outcome of neonatal surgical patients. However, one aspect that could be improved in our hospital would be the availability of a pediatric surgical service on all shifts, which would further reduce the time of surgical care.
It is well known that technological advances in neonatology, surgery, and anesthesia have reduced the mortality rate in neonatal surgery from 72% six decades ago to < 10% today in developed countries22,25,36. During the decade described here, we observed a steady decrease in mortality. One of our goals is to continue this trend, and continue to provide safe care, not only to improve survival but contribute to the quality of life of the surgical neonate and his or her family, remembering that the provision of adequate surgical care to all newborns will allow more children to develop their full potential by preventing death or treating disability37,38.
Among the limitations of this study, we find the reduced number of variables included, which does not allow us a better view of the behavior of surgical diseases in the neonatal stage.
In recent decades, the incidence of neonatal surgical pathology has increased; the care of these patients requires multidisciplinary management and represents a challenge within pediatric surgery. Although we are not a local or national reference center we have many congenital and acquired diseases, with a decreased mortality trend, close to the international average, and lower than national reports.

