











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Noninvasive arterial oxygen saturation (SaO2) is routinely used in neonatal intensive care units and other clinical settings. The measurement of SaO2 is used to make clinical decisions that might change a patient's prognosis, and it has been proposed as the fifth vital sign1-3.
Pulse oximetry determinations are based on spectrophotometry principles4; this technology has contributed to great advances in the management of patients, offering an easy, quick, noninvasive, and reproducible estimation of SaO25. Until now, pulse oximetry has been one of the main tools for noninvasive monitoring of in-hospital patients, especially for those with critical conditions.
The first hour of life is an adaptive period from fetal to extrauterine life, and factors such as altitude above sea level (ASL) might significantly affect SaO2 of the newborn6.
Although the inspired oxygen fraction in the air is constant (21% regardless of altitude), partial oxygen pressure is a function of the barometric pressure. For this reason, SaO2 is expected to be lower at high altitude locations, considering a lower atmospheric pressure7.
The relationship between SaO2 and altitude ASL varies among ages8. Therefore, it is important to have precise reference values in healthy full-term newborns.
This study aimed to analyze SaO2 levels in healthy full-term newborn patients at different altitudes ASL.
Methods
Study design
We conducted a multicenter cross-over study including six hospitals in Mexico located at different altitudes. Three hospitals were located < 250 m ASL, one at 1500 m ASL and two at 2250 m ASL. The study was approved by the research and ethics committees of each institution, and informed consent was obtained from parents or legal tutors before patients were included.
SaO2 measurement
We obtained SaO2 values in healthy full-term newborns, after the first 24 hours of life.
Besides SaO2, the following variables were obtained: age in hours, gender, gestational age determined by Capurro's score, weight and length at birth, type of birth, Apgar's score, and maternal disease if present.
Healthy full-term newborns were defined as those newborns who needed no supplementary oxygen and showed no respiratory distress, cyanosis, cardiac murmur, or any other evident clinical perturbance.
The device used for SaO2 determinations was the Masimo pulse oximeter Radical-7 model (Masimo, Irvine, CA, USA) with neonatal sensors (factory code 2514).
Before the study, the participating physicians were trained for the proper use of the oximeter to standardize the technique.
All measurements were performed when the newborn was awake with no agitation or irritability. The sensor was placed in the newborn's right hand, with a stabilization period of at least 1 min or until the plethysmographic curve was steady.
Statistical analysis
All data were collected in Excel format (Microsoft Office 2016) and exported to STATA 17.0 (Stata Corp LLC 4905 Lakeway Drive College Station, Texas. USA).
General patterns of healthy full-term newborns are expressed as frequencies or proportions considering qualitative variables, while quantitative variables were expressed as mean and standard deviations.
Analysis of variance (ANOVA) and χ2 were used to identify significant differences between the three groups, the first test for quantitative variables and the second for qualitative variables. For both tests, a p-value < 0.05 was considered significant.
Simple linear regression and multiple linear regression analysis were used to evaluate altitude ASL and SaO2, and other related variables. Regression analysis results are shown as correlation coefficients with 95% confidence intervals.
Results
A total of 4015 healthy Mexican full-term newborns from six centers were included (Table 1). Mean weight and height were 3252 g and 49.6 cm, respectively. Eutocic delivery was present in 66.5% of cases, and only 1.6% of newborns were born from multiple pregnancy.
Table 1 Study population
| Center | Location | Altitude in meters above the sea level | Number of newborns |
|---|---|---|---|
| Group 1 | Mérida, Yucatán Tampico, Tamaulipas Hermosillo, Sonora | 8-210 | 2437 |
| Group 2 | Zapopan, Jalisco | 1571 | 1300 |
| Group 3 | Mexico City | 2240-2265 | 278 |
| Total | 4015 |
The mean gestational age was 39 weeks, and the Apgar's score at the first minute of life was 8.2 and at 5 minutes, 8.9 (Table 2). The mean SaO2 of all healthy Mexican full-term newborns was 97.6 ± 1.8%. For group 1, the mean SaO2 was 98.2 ± 1.4%, for group 2, 96.7 ± 1.9% and for group 3, 96.0 ± 2.1%.
Table 2 General features of healthy Mexican full-term newborns
| Characteristics | Number/mean | Percentage/SD* |
|---|---|---|
| Male | 2020 | 50.3% |
| Female | 1995 | 49.7% |
| Weight (g) | 3253 | ± 435 |
| Length (cm) | 49.6 | ± 2.4 |
| Gestational age (weeks) | 39 | ± 1.2 |
| APGAR'S score | ||
| At the 1st min | 8.2 | ± 0.6 ± 0.3 |
| At 5 min | 8.9 | |
| Type of birth | ||
| Regular delivery | 2671 | 66.5% |
| Cesarean section | 1344 | 33.5% |
| Multiple pregnancy | 64 | 1.6% |
| Maternal disease | 193 | 5.2% |
| Groups considering altitude | ||
| Group 1 | 2437 | 60.7% |
| Group 2 | 1300 | 32.4% |
| Group 3 | 278 | 6.9% |
SD: standard deviation.
A significant difference was observed among the three groups (p < 0.001), and higher between groups 1 and 2 (1.5%, p < 0.001) as compared with groups 2 and 3 (0.7%, p < 0.001) (Table 3).
Table 3 Group analysis
| Characteristics | Group 1 (< 250 m ASL) | Group 2 (1 500 m ASL) | Group 3 (2 250 m ASL) | p-value |
|---|---|---|---|---|
| SaO2 (mean ± SD) | 98.2 ± 1.4 | 96.7 ± 1.9 | 96.0 ± 2.1 | < 0.001 |
| Males (%) | 50.2 | 50.1 | 52.1 | 0.819 |
| Weight in kilograms (mean ± SD) | 3.3 ± 0.4 | 3.2 ± 0.4 | 3.1 ± 0.3 | < 0.001 |
| Gestation weeks (mean ± SD) | 39.1 ± 1.3 | 38.9 ± 1.1 | 38.9 ± 1.2 | < 0.001 |
| Cesarian section (%) | 28.7 | 34 | 72.6 | < 0.001 |
| Maternal disease (%) | 6.4 | 2.7 | 7.9 | < 0.001 |
| Age in hours at the time of measurement (mean ± SD) | 39.3 ± 15 | 47.1 ± 8.9 | 36.6 ± 11 | < 0.001 |
ASL: above sea level; SD: standard deviation; SaO2: arterial oxygen saturation.
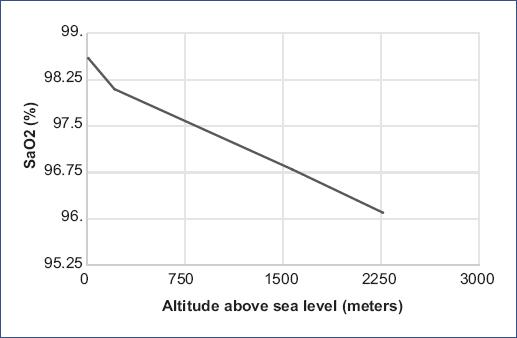
Other variables, such as weight, age (postpartum hours), cesarean section, maternal disease, and gestational age, showed a significant difference among the three groups (Table 4). The analysis showed a negative correlation between SaO2 and altitude ASL (coefficient = −0.00101), meaning that for every 1000 m ASL, SaO2 reduces by 1.01% (Figure. 1).
Table 4 Linear regressions between SaO2 and other variables
| Variables | Simple linear regression | Multiple linear regression | ||
|---|---|---|---|---|
| SaO2 (raw) | SaO2 (adjusted) | |||
| Coefficient (CI 95%) | p-value | Coefficient (CI 95%) | p-value | |
| Altitude ASL (1000 m) | −1.01 (−1.08/−0.94) | < 0.001 | −1.01 (−1.08/−0.94) | < 0.001* |
| Weight (Kg) | −0.04 (−0.17/0.08) | 0.525 | - | |
| Gestation weeks | −0.0014 (−0.0441/46.9) | 0.952 | - | |
| Cesarian section | −0.35 (−0.47/−0.23) | < 0.001 | −0.07 (−0.18/−0.03) | 0.188** |
| Maternal disease | −0.01 (−0.28/0.26) | 0.923 | - | |
| Age in hours (10^3) | −10 (−14/−6) | < 0.001 | −0.3 (−3.5/4.2) | 0.848** |
*Adjusted for weight, age by hours and cesarian section.
**Adjusted for ASL. ASL: above sea level; CI: confidence interval; S
aO2: arterial oxygen saturation.
Discussion
SaO2 values at different altitudes ASL have not been clearly established, which is why a "normal range", rather than a specific number has been used.
Rojas-Camayo et al.8 reported SaO2 decrease as altitude increases in all age groups, which is evident above 2500 m ASL.
Other authors suggest that SaO2 in newborns only decreases in altitudes > 1500 m ASL9; however, Samuel et al.7 described a small but statistically significant difference between SaO2 values in healthy full-term newborns close to sea level (25 m ASL) compared with locations with a moderate high altitude (780 m ASL) (98.9 vs. 98.5%, p = 0.03).
Our findings are consistent with other studies (Poets et al.4, Levesque et al.10, Guo et al.11, and O´Brien et al.12) reporting SaO2 values in healthy full-term newborns between 97% and 98.3% at an altitude close to sea level.
In our study, SaO2 fluctuates between 96 and 96.7% at altitudes > 1500 m ASL, similar to those reported by Guo et al.11 (96.4-95.5%) and Bakr and Habib13 (95.4%) but different from those reported by Thilo et al.6 (92.7%) and Morgan et al.14 (93%). This difference could be attributed to the type of oximeter sensor used in our study (similar to the one used by Guo et al. and Bakr and Habib)11,13 which uses signal extraction technology to provide precise lectures with slightly higher values.
As predicted, we demonstrated a statistically significant decrease of SaO2 as altitude ASL increases (< 250 m = 98.2 ± 1.4%, 1500 m = 96.7 ± 1.9%, and 2250 m = 96.0 ± 2.1%). Our results are supported by other studies reporting SaO2 values 0.4% lower than those observed at sea level in newborns at moderatehigh altitudes (780 m ASL).
Guo et al.11 reported a mean SaO2 of 97.9% close to sea level (0-500 m ASL), with 1.5% of decrease for higher altitudes (500-1500 m ASL) and 2.4% at moderatehigh altitudes (1500-2500 m ASL). That study concluded that SaO2 decreased by 1.54% for every 1000 m ASL, while our results showed a 1.01% decrease for every 1000 m ASL. This difference might be attributable to the altitude of the centers located at the extremes of the samples: in Guo's report, the center with the lowest altitude was located at 267 m ASL. Conversely, half of the centers in our study were located < 250 m ASL and in these places the mean SaO2 was 98.5%.
Here, we report an association between altitude and other variables such as weight, gestational age, type of birth, and preexistent maternal comorbidity (Table 3). The linear regression analysis showed that only two variables (besides altitude) were inversely related to SaO2: age in hours and type of birth. Multiple regression analysis was adjusted for altitude to exclude the possibility of confounding variables. Age in hours and type of birth had a stronger relationship with the health center than SaO2 (Table 4). As more specialized centers are expected to have more cesarean sections, a lower gestational age and weight or other related variables might be conditioned. To manage a possible effect of these factors on SaO2, we used multiple regression analysis showing a persistent reduction of 1.01% for every 1000 m ASL, meaning that the variation of SaO2 is mainly due to altitude instead of other factors.
In the present study, we demonstrated a statistically significant reduction in SaO2 level at higher altitudes ASL (1.01% for every 1000 m ASL).
This observation can be particularly relevant for clinical decision-making based on pulse oximetry as critical congenital heart disease screening in countries such as Mexico where more than half of the population lives above 1500 m ASL.
One limitation of this study was that the SaO2 values described were obtained only from the right hand and not the average of the right hand and foot.

