











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Worldwide, evidence shows a considerable increase in the prevalence of childhood obesity in the first stages of life1,2, mainly during the first 1000 days, a period from the fetal/neonatal stage to the first 2 years of life3,4. In countries such as the United States, a prevalence of overweight and obesity of 8.1% has been reported5; in Mexico, a prevalence of 6.5% is reported in children from 0 to 24 months6, which is considered high for this age group.
Obesity in the first years of life has been shown to be a strong predictor of obesity in school age and adulthood7; it is also considered a risk factor for the development of diabetes mellitus, arterial hypertension, sleep apnea, and a greater risk of social and psychological problems and premature death1. As childhood obesity is a preventable disease, prevention efforts during the first 1000 days of life should be a public health priority8-11.
Childhood obesity is defined as the excessive and abnormal accumulation of body fat detrimental to health caused by an imbalance in energy expenditure1. Its etiology is multifactorial resulting from a complex relationship between risk factors of different types, such as genetic, family, environmental, and community factors, among others12. These risk factors have been systematized in some theoretical models with a socioecological perspective to explain and study how they can influence and interact with the development of obesity13,14.
A widely recommended model in childhood obesity research is the Six-Cs Ecological Model of Obesity by Harrison et al.14, which states that to understand and explain the problem of childhood obesity, it is necessary to know not only the immediate context in which the child is developing but also the environmental factors beyond its proximal sphere and over time. The model is represented by six spheres and their interactions with each other: cell, child, clan, community, country or state, and culture. Within these spheres, it groups risk factors into five specific zones: Zone 1: nutrition-related opportunities and resources; Zone 2: activity-related opportunities and resources; Zone 3: nutrition-related practices; Zone 4: activity-related practices; and Zone 5: personal and relational attributes. The spheres and zones proposed by Harrison et al. have been studied and found to be predictors of childhood overweight and obesity, and are essential for future research and the development of prevention and health promotion interventions for this age group13,14.
Some published systematic reviews have documented ecological determinants of childhood obesity11,15-18. However, the results indicate that most studies have focused on preschool and school-age children from high-income countries; most have addressed only one sphere, and only some have assessed the combined impact of several spheres according to the Six-Cs model. Mexico has the highest prevalence of childhood obesity in the world19. However, no reviews of published studies that identify risk factors for obesity in children under 2 years of age in the Mexican population and the indicators of overweight and obesity in this age group have been found.
Analyzing the available evidence on childhood obesity factors from a holistic perspective is a good starting point to understand its nature, scope and, above all, to address it effectively. This study aimed to describe published evidence on obesity risk factors by sphere and zone in Mexico, considering the structure of the Six-Cs model, and to determine which of them have been associated with anthropometric indicators of overweight and obesity in children under 2 years of age.
Methods
A scoping review was conducted based on the PRIMSA-ScR extension20. The protocol is registered and published in the Open Science Framework (https://doi.org/10.17605/OSF.IO/UWX8V). This methodology allows to map of a large amount of literature on a topic, to assess its extent, scope, and the nature of different study designs, which improves the results without compromising their reliability, and to identify research gaps.
The following research questions were formulated: What risk factors for obesity have been studied in children under 2 years of age in Mexico, by sphere and area, and which of the factors studied are related to indicators of childhood obesity?
Eligibility criteria
The main inclusion criteria were studies conducted in Mexican children aged 0-2 years, and original articles of observational and experimental design in English, Spanish, and Portuguese that included an anthropometric indicator of overweight or obesity as an outcome variable. Review articles, gray literature, and preprints were excluded, as well as articles that were not accessible for retrieval.
Resources
The PubMed, Scopus, and EBSCOhost databases were searched for scientific articles. Medical subject headings (MeSH) terms were used, and the language and operationalization systems of each database, along with the use of Boolean operators: AND, OR, or NOT. The search period was from November to December 2022.
Search strategy
For the review, the identification of the Health Sciences Descriptors in Spanish (Descriptores en Ciencias de la Salud, DeCS) and its English analog, MeSH with the topic of study was performed. The main strategy was: in English: ("pediatric obesity" OR "child obesity" OR "infant overweight" OR "infantile obesity" OR "childhood obesity" OR "infant nutrition disorders" OR "Child Overnutrition") AND (Mexico OR Mexicans) AND (infant OR "1-23 months") AND ("Risk factors" OR "Social determinant of health"); in Spanish: ("Obesidad pediatrica" OR "obesidad infantil" OR "sobrepeso infantil" OR "trastornos de la nutricion del lactante" OR "sobrealimentacion infantil") AND (Mexico OR Mexicanos) AND (lactante OR "1-23 meses") AND ("Factor de riesgo" OR "Determinantes"), adapted for each database (Table 1). No time or language restriction filters were used in the databases.
Table 1 Health sciences descriptors (Descriptores en ciencias de la salud, DeCS) and MeSH for advanced search strategy
| Descriptors in Spanish | Descriptors in English | Descriptors in Portuguese | Synonyms in Spanish | MeSH |
|---|---|---|---|---|
| Lactante | Infant | Lactante | 1-23 meses Lactante Infante | Infant |
| Obesidad pediátrica | Pediatric obesity | Obesidade Pediátrica | Obesidad infantil Sobrepeso infantil Obesidad en la infancia Obesidad |
Pediatric Obesity |
| Trastornos de la nutrición del niño | Child nutrition disorders | Transtornos da Nutrição Infantil | Trastornos de la nutrición Estado nutricio del infante Nutrición infantil |
Child nutrition disorders |
| México | Mexico | México | Mexicanos Mexicans |
Mexico |
| Factor de riesgo | Risk factors | Fatores de risco | Factor de riesgo Población en riesgo |
Risk factors |
| Determinantes sociales de la salud | Social determinants of health | Determinantes sociais da saúde | Determinante de salud Determinantes estructurales de la salud | Social determinants of health |
MeSH: Medical Subject Headings.
Evidence selection
A spreadsheet database was created to organize and retrieve metadata and information from the selected articles. The first filter was performed to exclude those articles that did not meet the inclusion criteria based on the title and abstract. To explore the evidence, the reviewers were provided with the eligibility criteria and access to the systematic review software (Rayyan) to screen the articles and ensure the review process.
The researchers extracted data such as year of publication, title, region/place of study, study design, sample size, child age, and main findings. For the analysis of risk factors, the structure of the Six-Cs obesity model14 was considered and classified into the following spheres:
Cell included factors related to children's body composition and the influence of genetic and biological characteristics
Child included factors related to dietary self-regulation, self-control, environmental exposure, and sleep
Clan was related to family dynamics, adaptation to society, and parental characteristics (health and education, among others)
Community included factors such as the influence of the community on children and access to recreational areas/sports facilities
Country indicated the economic context and public policies
Culture included factors related to cultural and social norms, such as beauty standards and myths related to body composition.
Within these spheres, the risk factors were classified into five specific zones: Zones 1 and 2: opportunities and resources related to nutrition and physical activity, respectively; Zones 3 and 4: practices related to nutrition and activity, respectively; and Zone 5: personal and relational characteristics. In addition, the location to determine the geographical zones to be studied in Mexico was classified according to the criteria (Table 2).
Table 2 Classification by geographical area
| Region | State |
|---|---|
| North | Baja California, Sonora, Chihuahua, Coahuila, Nuevo León, and Tamaulipas |
| North-West | Baja California Sur, Sinaloa, Nayarit, Durango, and Zacatecas |
| Center-North | Jalisco, Aguascalientes, Colima, Michoacán, and San Luis Potosí |
| Center | Guanajuato, Querétaro, Hidalgo, State of Mexico, Mexico City, Morelos, Tlaxcala, and Puebla |
| South | Guerrero, Oaxaca, Chiapas, Veracruz, Tabasco, Campeche, Yucatán, and Quintana Roo |
| National | All |
Critical appraisal of evidence
Although scoping reviews do not necessarily require an assessment of the quality of evidence, we strengthen the reporting of observational studies in an epidemiology checklist21. Furthermore, the CDC's transparent reporting of evaluations with non-randomized designs statement22 for non-pharmacological experimental studies without randomization (quasi-experimental) was applied as an additional criterion to guarantee the quality of the data to be evaluated.
Results
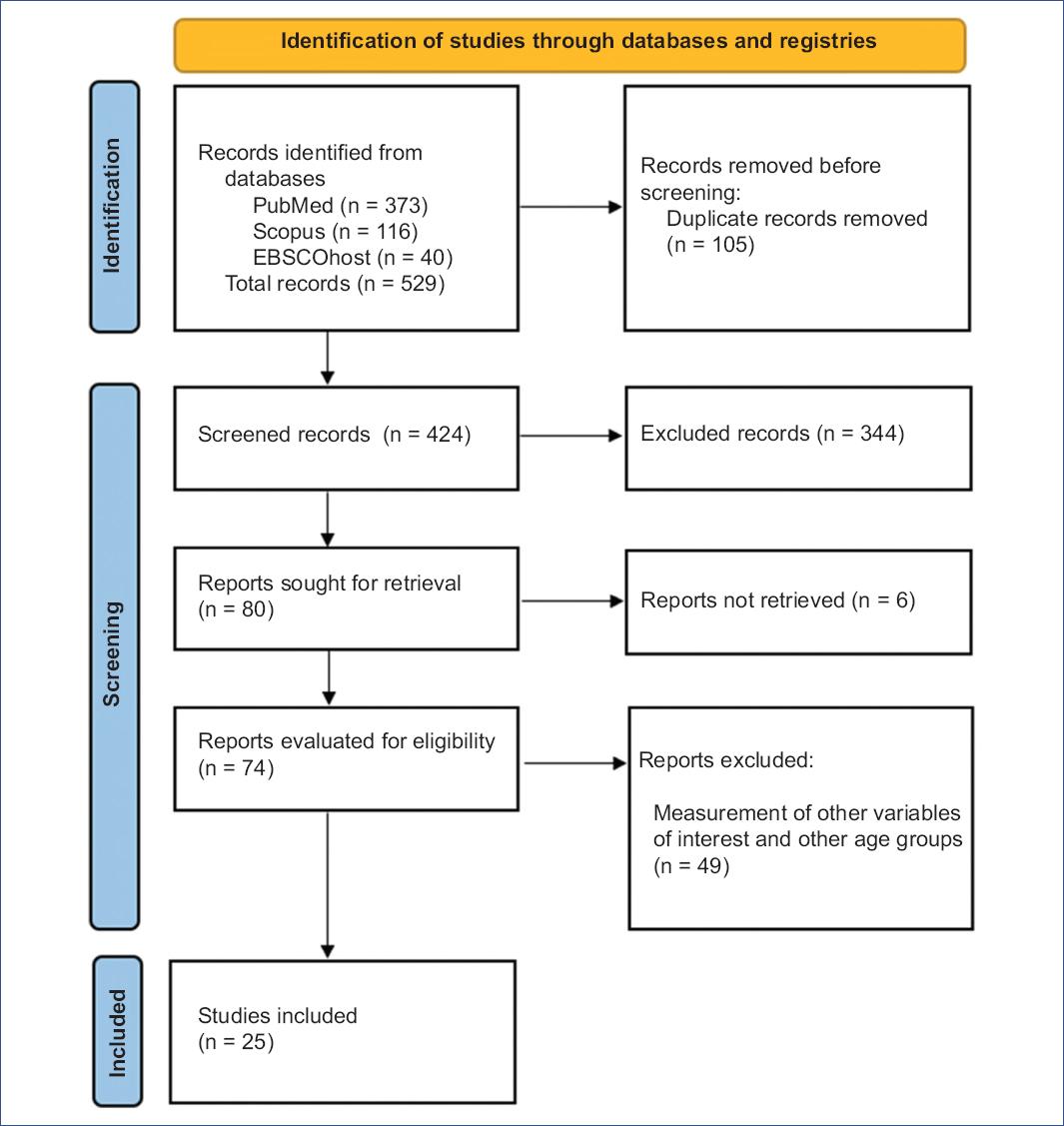
A total of 529 articles were retrieved from the databases previously mentioned. After eliminating duplicate articles (n = 424) and those that did not meet the inclusion criteria (n = 344), a total of 80 articles remained to be retrieved and assessed for eligibility for full-text review. Of these 80 articles, six were excluded due to lack of full-text availability, and 49 did not assess the variables or age group of interest. A total of 25 studies were considered eligible for this review (Figure 1).
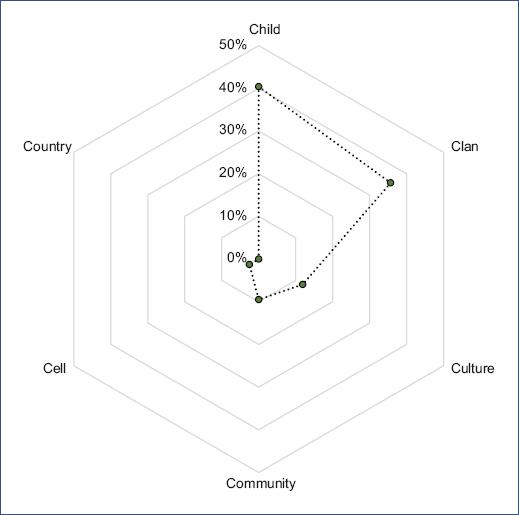
When classifying the 25 articles by spheres and zones (Table 3), we identified that the highest percentage (40.4%) studied the child sphere, followed by clan (35.7%), culture (11.9%), community (9.5%), and cell spheres (2.5%)23-47. Some articles studied two or more spheres together: child-clan sphere (n = 7, 2%), family-culture (n = 2, 8.0%), and child-clan-culture (n = 1, 4.0%), child-clan-community (n = 1, 4.0%), and clan-community-culture (n = 1, 4.0%). No article reported the study of the country sphere, thus denoting a relevant disproportionate gap of studies in the country, cell, community, and culture spheres (Figure 2).
Table 3 Spheres and zones explored in the studies classified according to Harrison's model
| Study | Sphere | Zones | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cell | Child | Clan | Community | Country | Culture | 1 | 2 | 3 | 4 | 5 | |
| Alarcón-Domínguez et al. (2020)23 | - | ✓ | ✓ | - | - | - | - | - | ✓ | - | ✓ |
| Álvarez-Villaseñor and George-Flores (2014)24 | - | ✓ | ✓ | - | - | - | - | - | - | - | ✓ |
| Bacardí-Gascón et al. (2012)25 | - | ✓ | - | - | - | - | - | - | - | - | ✓ |
| Campos et al. (2021)26 | - | ✓ | ✓ | ✓ | - | - | - | - | ✓ | - | ✓ |
| Cárdenas-Villarreal et al. (2018)27 | - | ✓ | ✓ | - | - | ✓ | - | - | ✓ | - | ✓ |
| Cuevas-Nasu et al. (2018)28 | - | - | - | - | - | ✓ | - | - | - | - | ✓ |
| Fernald et al. (2006)29 | - | ✓ | - | - | - | - | - | - | - | - | ✓ |
| Flores et al. (2021)30 | - | ✓ | ✓ | - | - | - | ✓ | - | ✓ | - | ✓ |
| Galindo-Gómez et al. (2015)31 | - | - | ✓ | - | - | - | - | - | - | ✓ | |
| Jimenez-Cruz et al. (2010)32 | - | - | ✓ | - | - | ✓ | - | - | ✓ | ✓ | ✓ |
| Jimenez-Cruz et al. (2010)33 | - | ✓ | ✓ | - | - | - | - | - | ✓ | - | ✓ |
| Kim-Herrera et al. (2021)34 | - | ✓ | ✓ | - | - | - | - | - | ✓ | - | - |
| Murata et al. (2020)35 | ✓ | ✓ | ✓ | - | - | - | - | - | - | - | ✓ |
| Okronipa et al. (2020)36 | - | ✓ | - | - | - | - | - | - | ✓ | - | - |
| Orozco-Núñez et al. (2022)37 | - | - | ✓ | ✓ | - | ✓ | - | - | ✓ | - | ✓ |
| Ortiz-Félix et al. (2021)38 | - | ✓ | ✓ | - | - | - | - | - | ✓ | - | ✓ |
| Ramirez-Silva et al. (2015)39 | - | ✓ | - | - | - | - | - | - | ✓ | - | - |
| Salinas-Martínez et al. (2012)40 | - | - | - | ✓ | - | - | ✓ | - | - | - | ✓ |
| Shamah-Levy et al. (2017)41 | - | - | ✓ | - | - | - | ✓ | - | - | - | ✓ |
| Téllez-Rojo et al. (2019)42 | - | ✓ | - | - | - | - | - | - | ✓ | - | - |
| Veile and Kramer (2016)43 | - | ✓ | ✓ | - | - | - | - | - | - | - | ✓ |
| Woo et al. (2012)44 | - | ✓ | - | - | - | - | - | - | ✓ | - | - |
| Yang et al. (2018)45 | - | - | - | ✓ | - | - | - | - | - | - | ✓ |
| Zaragoza-Cortes (2019)46 | - | - | ✓ | - | - | ✓ | - | - | ✓ | - | ✓ |
| Zavala et al. (2019)47 | - | ✓ | - | - | - | - | - | - | - | - | ✓ |
| Number of cases | 1 | 17 | 15 | 4 | 0 | 5 | 3 | 0 | 14 | 1 | 20 |
In the analysis by zones, we identified the following percentages: Zone 5: personal and relational attributes (52.6%); Zone 3: nutrition-related practices (36.8%); Zone 1: nutrition-related opportunities and resources (7.8%); and Zone 4: activity-related practices (4.0%). No studies were reported for Zone 2: physical activity-related opportunities and resources. The maximum number of zones studied was three, but minimally (8%).
Table 4 shows the characteristics of the risk factors for overweight and obesity that were studied in each article and the main findings23-47. The most common research design was observational: 14 cross-sectional studies (56%), six cohort studies (24%), a case-control study (4%), a qualitative study (4%), and only three quasi-experimental studies (12%). The sample size of the studies ranged from 17 to 25,075 children. The most studied geographic region in Mexico was the Central region (40%), followed by the North-West (16%), the North region (8%), simultaneously studied North and South regions (12%), and at the National level (24%).
Table 4 Factors that have been studied in Mexico regarding childhood obesity
| Author | n, infant age | Risk factors studied | Sphere | Zone | Study design | Region | Significant findings |
|---|---|---|---|---|---|---|---|
| Alarcón-Domínguez et al. (2020)23 | n = 90, 12-24 months | Perinatal factors (birth weight, age, sex) and feeding practices (breastfeeding and introduction of complementary foods). | Child, Clan | Z3, Z5 | Cases and Controls | North-West | Increased exclusive or mixed breastfeeding prevents excessive weight gain in infants. |
| Álvarez-Villaseñor and George-Flores (2014)24 | n = 368, 2-47 months | Age, sex of child, type of family. | Child, Clan | Z5 | Cross-sectional | North-West | Belonging to single-parent families is associated with OB. |
| Bacardí-Gascón et al. (2012)25 | n = 90, 0-4 years | Daily variations of weight-for-height and length-for-weight for age and gender. | Child | Z5 | Cohort | North-West | Children living in orphanages have reduced weight and height-for-age, reduced linear growth velocity and increased risk of OW. |
| Campos et al. (2021)26 | n = 2089, 6-35 months | Breastfeeding; Age, sex, birth weight, type of delivery; Complementary feeding; Home environment; Parental socioeconomic factors and place of residence. | Child, Clan, Community | Z3, Z5 | Secondary analysis of a cross-sectional study | National | High infant birth weight and maternal OB is related to infant OW/OB. |
| Cárdenas-Villarreal et al. (2018)27 | n = 267, 2-12 months | Child's age, sex, birth weight and energy intake; Maternal self-efficacy and maternal feeding attitude, Perception of child's hunger/satiety cues and mother's sleep; Maternal perception of child's weight. | Child, Clan, Culture | Z3, Z5 | Cross-sectional | North | Mothers who underestimate their child's weight, sleep fewer hours per day, and provide higher daily caloric intake to the child are associated with child OW/OB. |
| Cuevas-Nasu et al. (2018)28 | n = 1993, 0-59 months | Magnitude, weight distribution according to urban and rural localities of the country. | Culture | Z5 | Cross-sectional | National | Children living in urban areas and in the southern and northern regions of the country presented more OW and OB than those in rural areas, Mexico City, and Central regions. |
| Fernald et al. (2006)29 | n = 896, 12.5-23.5 months | Cognitive function (MDI) in low-income areas. | Child | Z5 | Cross-sectional | National | Child's mental development negatively associated with child's weight. |
| Flores et al. (2021)30 | n = 1112, 1-4 years | Age and sex of the child, ethnicity, educational level, socioeconomic status, dietary patterns of parents. | Child, Clan | Z1, Z3, Z5 | Cross-sectional | Center | Dietary patterns of the child (lower consumption of fruits and vegetables and traditional diet) were associated with greater OW and OB. |
| Galindo-Gómez et al. (2015)31 | n = 40, 28-56 days | Maternal weight and adiponectin levels present in breast milk. | Clan | Z5 | Cross-sectional | North and South | Adiponectin level in breast milk is associated with infant weight gain. |
| Jimenez-Cruz et al. (2010)32 | n = 813, 5-24 months | Beliefs about food and physical activity; perceptions of child's weight. | Clan, Culture | Z3, Z4, Z5 | Cross-sectional | North and South | Mothers who underestimate their child's weight are associated with more OW and OB in children. |
| Jimenez-Cruz et al. (2010)33 | n = 810 dyads, 5-24 months | Frequency and consumption of food; feeding practices; mother's weight. | Child, Clan | Z3-Z5 | Cross-sectional | North and South | Introduction of energy-dense foods, high consumption of snacks and sugary drinks, less breastfeeding, higher maternal BMI is related to child OW and OB. |
| Kim-Herrera et al. (2021)34 | n = 263 dyads, 6 y 9 months | Feeding styles; complementary feeding practices. | Child, Clan | Z3 | Cohort | Center | Stressful parental feeding style is associated with growth markers in 6-month-old infants. |
| Murata et al. (2020)35 | n = 57, < 4 months | Analysis of newborn stool samples, Type of delivery (vaginal and cesarean) and mother's weight. | Cell, Child, Clan | Z5 | Cross-sectional | Center | Birth by cesarean section is associated with an alteration in the intestinal microbiota of infants, and both are associated with child OB. |
| Okronipa et al. (2020)36 | n = 59, 7-24 months | Effect of milk supplementation; sweetened and unsweetened supplementation. | Child | Z3 | Quasiexperimental | Center | No significant difference was found between type of milk supplementation and child OW and OB |
| Orozco-Núñez et al. (2022)37 | n = 17 women with children under 2 years of age | Economic, cultural and family factors in the availability of consumed food. | Clan, Community, Culture | Z3, Z5 | Qualitative | Center | Family income, gender roles, and beliefs about children's preference for ultra-processed products lead to greater availability of high-calorie beverages and foods and predispose children to OB. |
| Ortiz-Félix et al. (2021)38 | Intervention group: n = 30 mother-child dyads; Control: n = 30 mother-child dyads. | Prenatal educational intervention (feeding practices, hunger-satiety cues and maternal perception of infant weight. | Child, Clan | Z3, Z5 | Quasiexperimental | North-West | Educating mothers about feeding practices and improving the perception of the child's weight promotes the child's proper nutritional status. |
| Ramirez-Silva et al. (2015)39 | n = 727, 0-4 years | Breastfeeding practice, serum total cholesterol and low-density lipoprotein (LDL) cholesterol, triglycerides, and insulin. | Child | Z3 | Cohort | Center | Exclusive and predominant BF at 3 months is associated with less adiposity in children at 4 years of age. |
| Salinas-Martínez et al. (2012)40 | n = 903, 1-5 years | Age, sex African American, Mexican American. | Community | Z5 | Cross-sectional | Center | Mexican children had differences in waist circumference of 1 cm more than African-American children; and up to 4 cm less than Mexican-American children. Males showed more OB than females. |
| Shamah-Levy et al. (2017)41 | n = 5087 dyads, 0-4 years | Household food insecurity; maternal obesity. | Clan | Z1, Z5 | Cross-sectional | National | Household food insecurity is related to maternal OB and risk of child stunting. |
| Téllez-Rojo et al. (2019)42 | n = 935, 0-5 years | Growth trajectories and children's caloric intake; postpartum maternal BMI. | Child, Clan | Z3, Z5 | Cohort | North | Childhood OB is associated with mothers with OW/OB and who provide their children with more calories than recommended. |
| Veile and Kramer (2016)43 | n = 3576, 0-5 years | Birth by cesarean section; BMI of mother. | Child, Clan | Z5 | Cross-sectional | National | Cesarean births are associated with OB, but only in children whose mothers had a high BMI. |
| Woo et al. (2012)44 | n = 192, 1-2 years | Serum APN exposure in breast milk. | Child | Z3 | Cohort | Center | Infants exposed to high levels of APN in breast milk are associated with higher weight-for-age Z-scores. |
| Yang et al. (2018)45 | n = 249, 1-14 years | Maternal urinary concentrations of bisphenol A (BPA) exposure and phthalate metabolites in the third trimester of pregnancy; infant weight and length. | Community | Z5 | Cohort | Center | Exposure to the phthalate metabolite mono (2-ethyl-5-carboxypentyl) is positively related to the child's BMI. |
| Zaragoza-Cortes (2019)46 | n = 19 dyads, < 24 months | Complementary feeding educational intervention and maternal perception of infant weight. | Clan, Culture | Z3. Z5 | Quasi experimental | Center | Knowing how to introduce food and maintaining an appropriate maternal perception of infant weight has a positive impact on infant growth. |
| Zavala et al. (2019)47 | n = 25075, 1-5 years | Intestinal parasite infection; BMI. | Child | Z5 | Cross-sectional | National | Children infected by intestinal parasites (lumbricoides or intestinal protozoan infection) are more likely to have a higher BMI Z-score in the same year, 6 and 12 years later in life. |
APN: adiponectin; BF: breastfeeding; BMI: body mass index; MDI: Mental Development Index; OB:: obesity; OW: overweight; WC: waist circumference.
The limited number of risk factors studied by sphere was noticeable. By describing them and their relationship with some indicators of overweight and obesity, our findings showed the following: in the child sphere, most of the risk factors corresponded to characteristics of the child and practices related to nutrition. Those related to some indicators of child overweight and obesity were birth by cesarean section43 and high birth weight26; as for nutritional practices, those related to child overweight and obesity were adiponectin levels in breast milk31, higher daily caloric intake27, lower consumption of fruits and vegetables, and traditional diet30. Conflicting data were found on the protective effect of breastfeeding23,26,33,39. In addition, children with better mental development29 had a lower prevalence of overweight or obesity.
In the family sphere, the main risk factors for overweight and obesity were mothers with a high body mass index33, less sleep than recommended27, a high-calorie diet42, and those who underestimated their child's weight27. It was also found that children living in single-parent families24, with a stressful parenting style34, and with food insecurity at home41 tended to gain more weight.
In the community and culture sphere, the following factors were identified as being related to overweight and obesity: living in urban areas and the northern and southern areas of the country28, family income, gender roles, and beliefs about children's preference for ultra-processed products led to greater availability of caloric beverages and foods37.
Discussion
This scoping review on risk factors for obesity in infants in Mexico showed that this topic is emerging but in progressive development. In fact, a significant number of articles highlighted the importance of considering the first 1000 days of life as a key period for obesity prevention48,49.
In the study of risk factors for obesity in infants, we found that the majority of articles reviewed used observational research designs with a limited number of factors per sphere and zones. Also, an incipient use of quasi-experimental design given that only two phase II (feasibility) studies were identified, despite the importance of promoting a multifactorial study of obesity at this level14,50.
The results identified in this study reveal a great disproportion of studies per sphere. The child and family spheres were the most addressed individually and as a whole, while the community and culture spheres were the least studied. Furthermore, no studies were found to address all spheres. To date, the political sphere has not been studied during the first 2 years of life. These findings are similar to previous systematic reviews, which reported that the most studied spheres to identify risk factors for overweight and obesity are the child and family spheres18,51.
The main risk factors related to the weight status in children under 2 years of age in Mexico were in the child sphere and zones related to personal characteristics and nutritional opportunities. The most important factors were as follows: birth by cesarean section, high birth weight, inadequate feeding practices such as daily caloric intake higher than recommended, and lower consumption of fruits and vegetables in the diet; the practice of breastfeeding showed contradictory evidence. In the family sphere, the most important factors were mothers with obesity and underestimating their children's weight, stressful parenting style, and food insecurity at home. In the community and culture sphere, the factors identified were living in urban areas, family income, and mothers' beliefs about children's preference for ultra-processed products. All these factors are consistent with previous literature on risk factors for obesity in the first 1000 days of life17. Some gaps are apparent in the Community, Culture, and Country domains and in Zones 2 and 4, involving components related to practices, opportunities, and resources related to infant physical activity, sleep, knowledge related to active lifestyles, and parental encouragement of infant activity, practices related to physical activity, such as excessive use of screen devices, and sedentary behavior.
The limited number of studies identified in this review may be due to policy strategies focused on obesity prevention in the first 1000 days of life have recently been published in Mexico52,53. These strategies have been formulated considering evidence on the main identified modifiable risk factors for obesity. These strategies are directed at two stages: The first focuses on antenatal care to optimize maternal health and lifestyle in preparation for pregnancy, achieve recommended weight gain during pregnancy, and prepare mothers for exclusive breastfeeding; the second strategy focuses on the postnatal period. The main focus is on the application of cognitive-behavioral interventions, individually and in family, in clinical settings, at home, or in combinations, using digital technology to promote appropriate feeding practices (breastfeeding, complementary, and perceptual feeding), lifestyle training mainly related to nutrition, physical activity, and sleep quality. Therefore, the number of studies in Mexico should increase and help to identify risk factors that determine the problem of overweight and obesity in the first 1000 days and, in turn, pursue intervention studies.
The limited number of publications selected in this article suggests that this topic is challenging. Time and cost are barriers to designing projects that include more determinants per sphere, which should be mitigated in future studies. Developing strategies and using culturally appropriate tools to measure risk factors are urgent for the pursuit of holistic health, especially for young children. High-income countries are conducting an increasing number of trials to prevent obesity in the first 1000 days, with promising results for preventing childhood obesity54-56. These studies consider areas and opportunities for research, based on evidence of factors associated with obesity in the first 1000 days, and generate recommendations for health professionals caring for this age group57,58. Therefore, it would be important to consider these strategies in future research studies on the Mexican population.
To the best of our knowledge, this is the first study to systematically review evidence for obesity prevention in children under 2 years of age using the Six-Cs as an ecological framework for childhood obesity. Our analysis provides a clear description of where research efforts for obesity prevention in the first 1000 days are currently focused and provides a broader understanding of the existing literature and its gaps, which is useful in delineating future research.
This review does not summarize the evidence on the magnitude of associations between determinants in the different Six-Cs spheres and children's weight, which could be considered a limitation. However, this review aimed to quantify and describe the studies according to the Six-Cs spheres and zones, not to identify new risk factors for childhood obesity or to compare the results of the studies. Therefore, studies were included regardless of the study designs, statistical analyses, and definitions of childhood overweight and obesity used.
The determinants of overweight and obesity at the individual and family level in children under 2 years of age are the most studied. However, it is important to recognize that these alone cannot explain children's weight. As aspects of different natures determine childhood obesity, studies should be based on a more holistic perspective, that is, simultaneously addressing aspects of different spheres and zones (socioecological models). The weight status of populations should be followed in longitudinal cohorts to develop informed, evidence-based interventions in the future and try to reduce obesity from an early age for better health in adulthood. This will require new analytical, qualitative methods, and more appropriate quantitative analyses, such as multilevel modeling techniques, to include all relevant determinants of childhood obesity in future research. Despite the research conducted in Mexico, more efforts are needed to conduct studies that integrate socioecological models to reduce the research gap on obesity in the first 1000 days of life and, thus, reduce the risks later in life. In addition, it is important to have policies focused exclusively on this period of life and to implement them throughout the country.

