











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Obstructive anomalies of the aortic arch (OAA) include a group of anatomical malformations that are differentiated by the lack of anatomical continuity of the aortic arch (interruption of the aortic arch). OAA can present with anatomical continuity of the aorta in which there is a fibrous segment causing a total obstruction (aortic atresia), or there is only a reduction of the vessel lumen, causing a circumscribed partial obstruction (coarctation of the aorta). The clinical behavior of these anomalies is similar. We previously reported our experience in OAA in a study of autopsy cases from the Hospital Infantil del Estado de Sonora and found that coarctation of the aorta was the most frequent finding, followed by interruption of the aortic arch; no case of aortic arch atresia was found1. Reports on this anomaly in the medical literature are scarce and are generally isolated clinical cases. As this is the first clinical case of atresia of the distal segment (isthmus) of the aortic arch diagnosed in our institution, we decided to report it.
Clinical case
We describe the case of a male neonate born at term vaginally, the product of the third gestation, with a birth weight of 2.5 kg. The mother was aged 24 years with apparent good health, and the father was 34 years with positive addiction to crystal meth and marijuana. The patient was referred from a secondary level care hospital where he arrived for presenting food refusal, irritability, and crying without tears in the first 48 hours of life. At the hospital, the patient showed acrocyanosis, generalized pallor, dry oral mucosa, respiratory distress, and hypothermia signs. During the hospital stay, the patient was diagnosed with congenital heart disease, interruption of the aortic arch type A with ventricular septal defect and patent ductus arteriosus, right ventricular systolic dysfunction, and moderate secondary tricuspid and mitral regurgitation. Prostaglandin was indicated at a dose of 0.01 μg/kg/min. The patient was transferred to the Hospital Infantil del Estado de Sonora in Hermosillo, Sonora, where he received supplemental oxygen through nasal cannulas at 2 L/min with an oxygen saturation of 92% and was admitted to the Neonatal Intensive Care Unit. Physical examination revealed marmoreal skin, systolic murmur in the aortic area, and a third murmur in the mitral area; upper extremity pulses were brisk, and lower extremity pulses were diminished in intensity. A central venous catheter was placed through the right subclavian puncture. The patient was evaluated by a pediatric cardiologist, who found a normal phenotype on physical examination, with hemodynamic instability, earthy tinge, and tachypnea. Auscultation showed a low left parasternal third sound and no precordial murmur. The heart rate was 155 bpm, according to the monitor. The hepatic border was palpated 4-5 cm below the right costal border. Bulging pulses were detected in the upper limbs that were not found in the lower limbs. The sphygmomanometer on the right upper limb recorded a pressure of 128/87mmHg, the left upper limb 107/81mmHg, and the lower limb 86/57mmHg.
Chest X-ray showed grade IV cardiomegaly with a dilated right atrium and capillary congestion in the lung fields. The echocardiogram study indicated situs solitus with dilatation of cardiac cavities. In the atrial septum, color Doppler demonstrated a unidirectional left-to-right shunt through a 2.5 mm diameter foramen ovale. At the tricuspid valve, continuous and color Doppler showed regurgitant flow with a velocity of 4.19 m/s and a gradient of 70.2 mmHg. Therefore, concordant atrioventricular and ventricular-arterial connections were found. In addition, a membranous ventricular septal defect of 3.5 mm in diameter was observed, and color Doppler demonstrated a bidirectional shunt at this level. The pulmonary artery trunk was found with confluent branches, and no ductus arteriosus shunt was observed at this level. The left ventricular outflow tract was free, and the aortic valve showed no alterations. The aortic arch was visible on the left and was incomplete due to a lack of continuity with the descending aorta in its distal segment. The presence of three supra-aortic vessels was visualized, and the interruption of the aortic arch was observed after the origin of the left subclavian artery (Figure 1A and 1B).
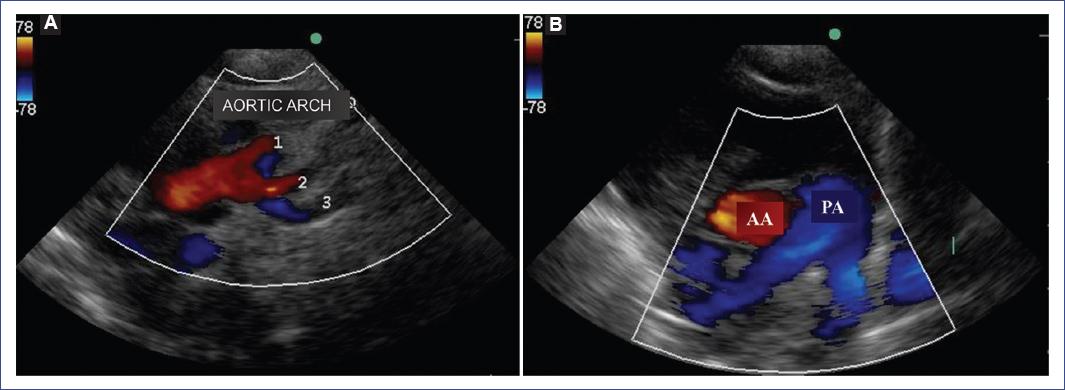
Figure 1 Echocardiogram. A: the aortic arch and three supra-aortic vessels with no continuity with the descending aorta are observed. B: pulmonary artery (PA), ascending aorta (AA), and confluent branches are shown. Absence of ductus arteriosus.
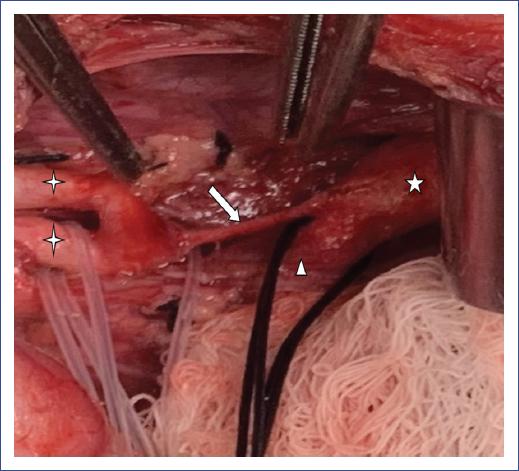
Due to the findings, a CT angiography study with image reconstruction was indicated, in which the interrupted segment following the left subclavian artery and the absence of communication between the pulmonary artery and the descending aorta through the ductus arteriosus were visualized (Figure 2A and 2B). The interrupted space between the aortic arch and descending aorta measured 12.3 mm. The descending aorta showed good size, receiving blood flow through two small-caliber intercostal arteries in its upper segment (Figure 3). The interrupted aortic arch type A diagnosis was proposed against the differential diagnosis of aortic arch atresia, and urgent surgical intervention was indicated. The patient presented a sudden respiratory deterioration with a decrease in oxygen saturation reaching 60% and bradycardia of 70 bpm with poor respiratory effort, for which it was decided to maintain the airway with assisted mechanical ventilation. Due to hypoxemia, the patient presented a state of mixed acidosis. The patient underwent surgery through a left postero-lateral thoracotomy. Vascular structures were dissected and identified, allowing visualization of the continuity of the aortic arch with the descending aorta through an obliterated fibrous tissue. In addition, the ductus arteriosus was obliterated, and proximal and distal clamping was performed for section and ligation of the ductus arteriosus (Figure 4). Aortic advancement was performed to anastomose the aortic arch and descending aorta, and the subclavian artery was used for a wide junction. Clamping was released, and hemostasis was checked; however, the patient presented gradual and progressive hemodynamic deterioration. Support was given with direct cardiac massage maneuvers for 5 minutes with an adequate response. Regardless, after 10 minutes, the patient deteriorated again into asystole but with no response to management.

Figure 2 CT angiography. A: three supra-aortic vessels and
interruption of the aortic arch behind the left subclavian artery are
observed. B: pulmonary artery and confluent branches are shown.
Connection of two small intercostal arteries ( ) in the upper part of
the descending aorta.
) in the upper part of
the descending aorta.





Discussion
Of the OAAs, atresia of the aortic arch’s distal segment (isthmus) is extremely rare. In our previous report on obstructive anomalies of the aortic arch, aortic atresia was not included1. The present report is the first clinical case of a patient with aortic atresia diagnosed in a term male newborn with a normal phenotype. OAAs have been associated with genetic syndromes such as 22q·11 deletion, DiGeorge syndrome, and Down syndrome1,2. The presentation of this clinical picture in the first 48 hours of life may be related to hemodynamic adjustments that occur in vascular resistance, mainly at the pulmonary level. Newborns and infants present severe heart failure with a tendency to develop shock, which results in death within a few days of birth if untreated3. In cases of OAA, the ductus arteriosus is usually the structure that allows systemic blood flow along with high pulmonary vascular resistances at birth; subsequently, the ductus arteriosus may begin to close, and with it begin the signs and symptoms of hemodynamic imbalance. The use of prostaglandin E1 is indicated when the specific diagnosis of this ductus-dependent congenital heart disease is established to prevent the closure of the ductus arteriosus. The dose of prostaglandin to be administered by infusion is 0.01 μg/kg/min, which may vary according to the clinical condition; in case of circulatory collapse due to closure of the ductus arteriosus, a dose of 0.1 μg/kg/min is used.
The presence of cardiomegaly and capillary congestion in the radiological study of the thorax reflects the clinical hemodynamic state in which the patient was received. Some patients may survive infancy without the need for surgical treatment, as they usually have a ductus arteriosus and well-developed collateral arteries that carry blood flow to the descending aorta; in the absence of ductus arteriosus, early development of collateral arteries of adequate caliber may replace the function of the ductus arteriosus4. In other cases, when the ductus arteriosus is obliterated and collateral arterial vessels are not well developed, a pressure difference can occur in the segments of the obstructed aortic arch and the descending aorta, triggering heart failure, as in this case2. The association of patent ductus arteriosus in this anomaly has been described in 98%, and ventricular septal defect in 90%5. These two anomalies were present in this case, but the ductus arteriosus presented early closure, as observed in the echocardiographic and CT angiographic studies. Other associated anomalies reported are aortic and sub-aortic valvular stenosis.
Although the distinction between interruption and atresia of the aortic arch is complex, the hemodynamic consequence of these two anatomical lesions is similar. The surgeon identifies them at the time of surgery, as occurred in this case and in others reported previously6,7. Echocardiography remains the preferred method for evaluating patients with suspected congenital heart disease. Furthermore, in the case of OAA, it is possible to define the site of obstruction. Echocardiography can be performed from the prenatal stage, allowing early detection of cardiac malformations and referring the patient to a medical center for optimal care, improving the patient’s prognosis. CT angiography studies, especially with multi-slice technology and magnetic resonance imaging (MRI), have gained relevance in studying vascular anomalies, mainly in neonates and infants. In this case, the CT angiography confirmed the echocardiographic findings and provided information on the collateral circulatory state that carried flow to the descending aorta through small intercostal vessels (Figure 3)8,9. Cardiac catheterization in the critical clinical condition of the neonate is not an option as it was previously. Immediate medical care and timely diagnosis contribute to a stable clinical condition, maintaining the ductus arteriosus with prostaglandin supply and allowing better hemodynamic stability before surgery. This clinical condition, however, was not present in our patient due to hemodynamic deterioration with pulmonary compromise and hypoxemia that caused a state of mixed acidosis during the critical evolution of this case. Echocardiographic evaluation of this patient found pulmonary arterial hypertension as part of an unstable hemodynamic situation. The patient underwent surgery to connect the aortic arch with the descending aorta through an aortic advancement and using the subclavian artery to create a wide anastomosis10. However, the patient deteriorated and presented irreversible cardiac failure at the end of the surgical procedure.
The prognosis of patients with OAA who undergo surgery in medical centers is good. A survival rate of 100% has been described in an average follow-up of 9 years after corrective surgery for this malformation11. We consider relevant the state of hypoxemia and mixed acidosis that this group of patients usually present since, for this reason, any pharmacological or surgical intervention may be unsuccessful. We should consider the diagnostic possibility of aortic atresia in the presence of interruption of the aortic arch.

