











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The neonatal period is considered the most critical and essential in growth and development1 because newborns experience unstable conditions in the first hours and days after birth, challenging them to adapt to extrauterine life. Moreover, preterm infants show a reduced ability to adapt to the surrounding world1,2. Consequently, many preterm infants may be admitted to neonatal intensive care units due to respiratory problems, instability in temperature, blood pressure, heart rate, respiratory and cardiac distress, and neurological diseases in the first days of life3. Epidemiological studies reveal that 9.6 to 12.9 million premature infants are born annually, accounting for 5-15% of live births worldwide4. In this regard, 1.6 million births occur in Iran each year, of which 160,000 newborns are preterm (8-12%) and require specialized care in neonatal intensive care units3,4.
Mothers of preterm babies are faced with a newborn who needs special equipment and is being cared for to survive. After a complicated delivery process, they experience severe emotional shock. As a consequence of this shock, mothers do not have sufficient capacity and strength to care for the baby5 since facing a premature baby, or a patient admitted to the Neonatal Intensive Care Unit (NICU) is one of the most sensitive and stressful stages in the life of parents, especially mothers. This confrontation is considered a major emotional crisis and can have adverse and long-term effects on the lives of mothers6. The negative impact of preterm birth on mothers consists of feelings of inability and intolerance, incompatibility, sadness, anxiety, fear, worry, guilt, anorexia, failure to breastfeed, depression, and sleep disorders7,8. These mothers also experience significant changes in family relationships, work, social activities, family responsibilities, and parenting roles9.
Seeing a premature infant inside an incubator or warmer under a ventilator or oxygen therapy, with multiple intravenous lines connected, cause these mothers to doubt their ability to care for their babies. As a result, many have not been able to adapt to the baby’s condition and needs and have subsequently expressed intolerance to caring for their baby8. This is why resilience is an essential concept of positive psychology and refers to the dynamic process of positive adaptation to bitter and unpleasant experiences10. Resilience is also defined as measuring a person’s ability to cope with stressors and factors that threaten a person’s mental health11. Therefore, improving resilience and increasing mothers’ threshold of tolerance to stressful conditions can moderate their helplessness under stressful situations and boost their mood, mental and physical health, and involvement in caring for their baby10,11.
Mothers with low resilience are less active in the pediatric section and are not sufficiently involved in caring for their babies and performing their role as mother12. In addition, one of the fundamental functions of mother-infant attachment is breastfeeding13. Consequently, developing a sense of self-efficacy in breastfeeding mothers of preterm infants improves their ability to care for their infants to achieve a stable condition. In other words, breastfeeding self-efficacy means believing in one’s ability to breastfeed and care for the baby14.
Breastfeeding self-efficacy is influenced by four essential factors, including past breastfeeding experiences, surrogate experiences (observing mothers who have been successful at breastfeeding), verbal encouragement from influential people in the mother’s life (spouse, friends, family, and treatment team, especially nurses), and physical and mental illness (postpartum depression, anxiety, and fear)14,15. Medical staff, particularly nurses in the NICU, can promote mother-infant interaction and attachment and reinforce resilience and self-efficacy in breastfeeding. In addition, they can encourage and support them to stay in bed with their baby and engage in care procedures16,17. By counseling and assisting the mothers of these infants, nurses can promote a sense of self-efficacy in breastfeeding. Mothers may experience a sense of empowerment, self-efficacy, and reassurance18.
As mentioned in previous studies, kangaroo mother care (KMC) is one of the most influential participatory care in promoting infant health and improving mothers’ sense of empowerment. Kangaroo care involves skin-to-skin contact between mother and infant and addresses infant health, mother-infant relationship, and maternal satisfaction and empowerment17. Recent studies examining the effect of KMC on preterm infants and their mothers have been conducted. In particular, research has shown that kangaroo care improves physical health indicators in preterm infants13,19. However, as this care is a bidirectional interaction pattern between mother and baby, it may also affect the physical and mental health indicators of the mothers12,13,19.
KMC stimulates oxytocin secretion and decreases cortisol. As a result of these biochemical changes, the mother’s sense of calm, vitality, and pain tolerance is increased, and stress, anxiety, and worry are reduced20. However, only a few studies have examined the effects of kangaroo care on mothers, especially on mothers of preterm infants admitted to the NICU7,18,21. In this regard, de Macedo et al. (2007), Bigelow et al. (2012), and Faramarzi et al. (2014) have shown that KMC relaxes mothers and helps them feel better, empowers them, and helps them to be more tolerant, reinforcing these feelings8,17,22. In addition, Widström et al. (2019), Yilmaz et al. (2020), and Zhang et al. (2020) have reported that kangaroo care increases mothers’ confidence in caring for their infants13,23,24. These studies also found that mothers needed less help with breastfeeding and demonstrated more self-efficacy in breastfeeding13. Most of these investigations evaluated the impact of KMC on resilience and breastfeeding self-efficacy with educational booklets and videos and reported its benefits. Heidarzadeh et al. (2013) and Mohammadi et al. (2021) also found that KMC is a safe, effective, and feasible method of care for low-birth-weight infants that increases maternal engagement in NICU care and leads to successful exclusive breastfeeding, and can be a good substitute for CMC (conventional methods of care) in NICU in Iran25,26. However, Namnabati et al. (2016) argued that several challenges are faced for KMC in NICUs in Iran, such as maternal-related and organizational barriers and the need for a physician’s order to perform KMC. These cross-cultural differences between Iran and other developed countries, such as the United States, limit KMC in NICUs in Iran27.
Examining the influence of KMC through role-playing before an actual performance may be practical and valuable for maternal physical and mental health. Since this effect is unknown, we decided to study the influence of KMC on the resilience and self-efficacy for breastfeeding in mothers of preterm infants admitted to the NICU with the role-play method. We hypothesized that KMC through role-playing is more effective than the routine method in increasing the resilience and improving breastfeeding self-efficacy in mothers of neonates admitted to the NICU.
This study aimed to evaluate the effect of kangaroo care through role-playing on resilience and self-efficacy in breastfeeding in mothers of infants admitted to the NICU.
Methods
Study design
From November 2020 to March 2021, we conducted a single-blind randomized controlled trial with an intervention and a control group in a hospital with two NICUs affiliated with the University of Medical Sciences in western Iran.
Ethical considerations
The Ethics Committee approved the study of the Hamadan University of Medical Sciences (Umsha.rec.1399.1042) and prospectively registered in Clinical Trials (number IRCT20190703044082N4). At the beginning of the study, the researcher introduced herself and explained the study’s objectives. After providing participants with sufficient information about the study, those who agreed to participate signed an informed consent form. Participants were assured that all information would remain confidential. The researcher offered participants the possibility of withdrawing from the study at any time and assured them that their non-participation or withdrawal would not have any consequences.
Study population and sample size
Mothers of preterm infants admitted to two neonatal intensive care units participated in this study. Inclusion criteria included preterm infants ≤ 1,800 g, an Apgar score ≥ 7 at 5 minutes after birth and ≥ 30 weeks of gestation. It had to be a delivery of a single, healthy neonate without severe physical disorders and not having undergone surgery. It should be noted that these babies were not undergoing phototherapy. According to the opinion of a medical specialist, the neonate should also be in a condition to leave the incubator and the warmer and had to be able to breastfeed. Mothers’ absence of psychiatric problems (depression, bipolar disorder, among others) and the non-consumption of psychiatric drugs and tobacco were also considered. Mothers should be ≥ 18 years of age and able to read and write. Finally, the mothers had to be willing to participate in the study.
Exclusion criteria included the occurrence of unexpected physical problems in the infants during the study, mothers’ unwillingness to continue the investigation, death, transfer of the infant to another hospital, and mothers’ absence for one day of the intervention (because if the mother did not show up one day, kangaroo care was not performed).
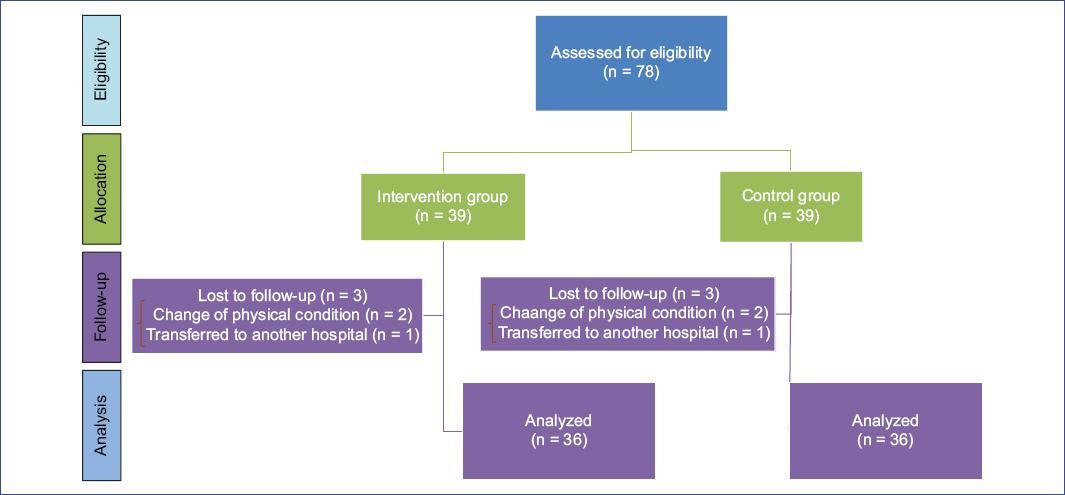
The sample size in this study was calculated according to Yilmaz et al. (with β = 80% and α = 0.05)13. A total of 78 mothers were randomly assigned to the experimental or control group. The sample size was estimated at 39 individuals with a 10% loss in each group. Three infants in each group were excluded from the study due to changes in physical status or transfer to another hospital (Figure 1).
Recruitment and allocation
After determining the sample size, a total of 78 patients were screened for eligibility; they were then randomly assigned to one of two groups by block randomization with a volume of 2 and an allocation ratio of 1:1 using a computer-generated randomization program stratified by parity (two strata: first and second). This study was conducted in a single-blind manner, so the questionnaires were collected by a researcher unaware of the assignment of individuals to groups.
Intervention
In the experimental group, each mother attended two 30-minute individual sessions in the hospital conference room. These mothers were taught how to hold a baby dummy in their arms. To do this, the researcher first talked to the mothers in this group and answered their questions about how to care for, hold, look at, and cuddle the baby. The researcher then helped them wear a particular blouse designed according to the KMC standard and protocol. These blouses mainly were loose-fitting, with short sleeves and buttons on the front of the garment that could be easily opened and closed. The mother would then sit in a chair in whatever position she felt comfortable for the next steps. The researcher placed the model baby with only a cap and diaper upright position between the mother’s breasts to teach her kangaroo care. After this step, the researcher closed the bottom buttons of the mother’s blouse. The model dummy was entirely placed between the mother’s breast and the cloth, reducing the possibility of falling and hypothermia. The researcher then stood next to the mother and asked her to try to make eye contact with the model while smiling, looking, caressing, and talking to the model baby. After training in embrace care by role-playing method, mothers in the intervention group performed this training three times a day (once per shift) for 30 minutes for 7 days with full supervision and accompaniment by the researcher. Mothers in the control group received a booklet training routine. All mothers completed the questionnaires several times: before the intervention, one day after, and one week after discharge. These questionnaires were applied by a researcher unaware of the allocation of individuals into the intervention and control groups.
Connor and Davidson Resilience Scale
We used the scale designed by Connor et al. (2003) in the United States to measure resilience28. This scale has 25 questions on five areas: individual and general competence (eight questions), tolerance to adverse effects and strength against stress (seven questions), positive acceptance of the change (five questions), self-control (four questions), and spiritual impact (five questions). The questions of this scale are scored from zero (completely incorrect) to four (always correct) according to Likert scores. The maximum score for this questionnaire is 100, and the minimum score is zero. Higher scores indicate more resilience. The face validity, content, and reliability of this questionnaire have been estimated by Ahangarzadeh et al. (2015). This study mentioned that the reliability of this instrument had been reported through Cronbach’s alpha method with a value of approximately 0.8229.
Breastfeeding self-efficacy questionnaire
One of the most important instruments to measure breastfeeding self-efficacy in this study was the Breastfeeding Self-Efficacy Scale designed in 1999 by Dennis. This instrument can measure the confidence and ability of breastfeeding mothers based on 5-point Likert-type items through 33 questions: 1 strongly disagree to 5 strongly agree. All questions in this questionnaire are positive, and the score range is 33 to 165. A higher score indicates higher self-efficacy for breastfeeding in mothers. Dennis performed face validity, content, and reliability of this questionnaire, and its reliability was estimated at 0.96 by Cronbach’s alpha method30. In Iran, Farhadieh et al. evaluated this questionnaire’s face validity, content, and reliability and considered it a suitable instrument for research31.
Data analysis
Data were analyzed with SPSS version 22 software. Descriptive statistics (frequency, percentage, mean, and standard deviation) were used for this purpose. After confirming the normal data distribution by the Kolmogorov–Smirnov test, the paired t-test was used to compare the mean of resilience and breastfeeding self-efficacy between the two groups on three measures. Finally, repeated measures analysis of variance was used to compare the mean of resilience and breastfeeding self-efficacy in each group three times of measurement. The statistical significance value was considered as 0.05.
Results
Most of the mothers in this study were graduates and self-employed. The mean age of the mothers was 37.31 ± 1.57 years in the intervention group and 37.42 ± 1.41 in the control group; the mean monthly income of the participants was $120 in both groups.
Most of the neonates in both groups were male. Their mean weight of the infants was 1721.42 ± 1.92 g in the intervention group and 1756.21 ± 1.74 g in the control group, and their mean gestational age was 31.42 ± 1.52 weeks in the intervention group, and 31.61 ± 1.06 weeks in the control group. No statistically significant differences were observed in the distribution of demographic characteristics between the two groups (p > 0.05) (Table 1).
Table 1 Demographic information of the participants
| Variable | Intervention group, n (%) | Control group, n (%) | p-value |
|---|---|---|---|
| Mother’s age (years) | |||
| 24-33 | 11 (28.20) | 12 (30.77) | 0.87* |
| 34-44 | 16 (41.03) | 16 (41.03) | |
| 45-55 | 12 (30.77) | 11 (28.20) | |
| Mother’s education | |||
| Illiterate | 2 (5.12) | 3 (7.69) | 0.79** |
| Primary | 11 (28.21) | 12 (30.78) | |
| Diploma | 18 (46.15) | 17 (43.58) | |
| Bachelor | 7 (17.95) | 6 (15.38) | |
| Master’s degree and higher | 1 (2.57) | 1 (2.57) | |
| Father’s education | |||
| Illiterate | 3 (7.69) | 3 (7.69) | 0.77** |
| Primary | 10 (25.64) | 12 (30.78) | |
| Diploma | 18 (46.16) | 18 (46.15) | |
| Bachelor | 5 (12.82) | 4 (10.26) | |
| Master’s degree and higher | 3 (7.69) | 2 (5.12) | |
| Mother’s job | |||
| Self-employed | 11 (28.21) | 13 (33.34) | 0.71* |
| Employee | 10 (25.64) | 9 (20.51) | |
| Housewife | 18 (46.15) | 18 (46.15) | |
| Father’s job | |||
| Self-employed | 19 (48/71) | 18 (46.15) | 0.77* |
| Employee | 7 (17.95) | 7 (17.95) | |
| Livestock and farmer | 13 (33.34) | 14 (35.90) | |
| Number of children | |||
| 2 | 19 (48/71) | 19 (48/71) | 0.89* |
| 3 | 13 (33.34) | 14 (35.90) | |
| ≥ 4 | 6 (15.38) | 5 (12.82) | |
| Sex of neonates | |||
| Male | 20 (51.29) | 21 (53.85) | 0.98* |
| Female | 19 (48/71) | 18 (46.15) | |
| Gestational age (weeks) | |||
| 30-33 | 21 (53.85) | 20 (51.29) | 0.98* |
| 34-36 | 18 (46.15) | 19 (48/71) |
*x2 test;
**Fisher exact test.
Resilience in mothers of premature neonates
Before the intervention, the resilience score in both groups was not statistically significant (p = 0.71). However, repeated measures analysis of variance demonstrated a statistically significant difference in the resilience score in each group one day and one week after performing the intervention (p < 0.001). Cohen’s d for resilience in the intervention and control groups showed the high impact of the intervention. Moreover, the independent t-test revealed a statistically significant difference between both groups in the resilience score one day and one week after the intervention (p ≤ 0.01). Therefore, the role-playing method was more effective than the routine method (booklet training) (Table 2).
Table 2 Comparison of resilience scores between both groups
| Study days Study groups | Before intervention Mean (SD) | One day after intervention Mean (SD) | One week after intervention Mean (SD) | F, mean difference, p-value for time* group |
|---|---|---|---|---|
| Control group | 43.74 ± 3.46 | 54.65 ± 3.22 | 66.43 ± 3.42 | 10.75, 0.67, 0.001** |
| Intervention group | 43.84 ± 3.96 | 87.87 ± 3.22 | 92.74 ± 3.11 | 29.54, 0.82, 0.001** |
| t, mean difference, | 0.01, 1.02, | 33.22, 2.76, | 26.31, 3.98, | |
| p-value | 0.71* | < 0.01* | < 0.01* |
SD, standard deviation.
*Student’s t-test;
**Repeated measure test.
Breastfeeding self-efficacy in mothers of premature neonates
At the beginning of the study, mothers in both groups showed a poor performance in breastfeeding self-efficacy, with no statistically significant difference between their breastfeeding self-efficacy scores (p = 0.83). However, after KMC training, mothers in both groups made significant progress in their breastfeeding self-efficacy scores. Intragroup comparison of the breastfeeding self-efficacy scores was statistically significant in each group (p = 0.001), demonstrating that KMC education by both methods (role-playing and routine) was effective. In addition, Cohen’s d for breastfeeding self-efficacy in the showed the high impact of the intervention. Furthermore, a statistically significant difference was observed between both groups one day and one week after performing the intervention (p = 0.01). Hence, the role-playing method proved more effective than the routine method (booklet training) (Table 3).
Table 3 Comparison of breastfeeding self-efficacy scores between both groups
| Study days Study groups | Before intervention Mean (SD) | One day after intervention Mean (SD) | One week after intervention Mean (SD) | F, mean difference, p-value for time* group |
|---|---|---|---|---|
| Control group | 23.14 ± 2.76 | 62.95 ± 2.12 | 73.65 ± 2.76 | 10.32, 0.69, 0.001** |
| Intervention al group | 23.32 ± 2.96 | 91.17 ± 2.41 | 112.04 ± 2.31 | 24.51, 0.81, 0.001** |
| t, mean difference, value* | 0.26, 1.42, 0.83* | 28.22, 3.64, | 38.39, 4.14, | |
| < 0.01* | < 0.01* |
SD, standard deviation.
*Student’s t-test;
**Repeated measure test.
Discussion
The results of the present study revealed that role-playing and routine methods effectively promote resilience and breastfeeding self-efficacy. However, the two groups showed statistically significant differences in improving resilience and breastfeeding self-efficacy. The role-play method seems more effective than the routine method in promoting resilience and breastfeeding self-efficacy in mothers of premature infants in the NICU.
In the literature, we found no data on the effect of KMC training by role-play method on resilience and breastfeeding self-efficacy in mothers of premature neonates. Therefore, the impact of KMC on resilience and breastfeeding self-efficacy is discussed broadly as follows.
Consistent with our findings, Ghazi et al. (2021) stated that a home visiting program based on the continuation of KMC positively affected maternal resilience in mothers of premature infants. These authors found a statistically significant difference in mothers’ mean resilience score one month after discharge between the intervention and control groups32. Although the results of this study show the efficacy of KMC in improving maternal resilience, the researchers taught KMC to mothers only with the routine method (booklet training), and the experimental group continued the KMC after discharge at home. Murty et al. (2018) found that KMC improves the resilience of families with low-birth-weight infants. Home-based KMC motivates families to manage problems effectively, ultimately saving the newborn from neonatal death10. This finding indicates that KMC is an effective method for improving the tolerance and resilience of families, especially mothers with preterm and low-birth-weight infants, consistent with our results. However, in the same study by Murty et al., mothers were also trained in KMC only with the routine method (booklet training)10. It seems that if education is conducted with more objective and effective methods, such as role-playing, it can help families manage the preterm birth crisis and increase tolerance and resilience more effectively.
Furthermore, in line with the present study, Rossman et al. (2017) remarked that the mother’s training and ability to care for her infant in the NICU positively affect maternal resilience and adaptability to conditions11. Herizchi et al. (2018) also showed that KMC improved maternal adaptability and tolerance. Thus, the authors suggest that KMC be taught continuously and with more efficient training methods to mothers of premature infants to promote maternal adaptation and improve the newborn’s condition33.
This study showed that breastfeeding self-efficacy of mothers of preterm infants admitted to the NICU improved in both the role-playing and routine education groups. However, the best results in promoting breastfeeding self-efficacy were observed in the role-play group. Although many studies have examined breastfeeding self-efficacy in mothers of term infants, few studies have examined the effect of KMC on breastfeeding self-efficacy in mothers of preterm infants admitted to the NICU. In this regard, Zhang et al. demonstrated that mothers in the intervention group (KMC) reported higher frequency and quality of breastfeeding than the control group. Therefore, it can be said that KMC significantly improved the number and quality of breastfeeding in mothers of preterm infants24, consistent with our observations. However, in the present study, the mean score of breastfeeding self-efficacy was higher in both groups. A possible explanation could be a difference in how KMC is taught.
Also consistent with the present study, Yilmaz et al. reported that KMC effectively promotes breastfeeding self-efficacy and creates a sense of empowerment in mothers, which consequently helps them to achieve better infant development13. Our results are consistent with published evidence reporting that frequent skin-to-skin contact between mother and infant is crucial for the successful transition to direct breastfeeding in preterm infants6,24,30,34 and the initiation of exclusive breastfeeding in healthy full-term infants13,24.
One of the notable limitations of the present study was the small sample size of the participants. Therefore, similar studies in different communities and with larger samples are recommended in future years. Moreover, in this study, mothers were followed up for one week after the intervention; we suggest following the effect of KMC on breastfeeding self-efficacy in mothers of preterm infants for more weeks.
This study showed that teaching KMC through role-playing and routine methods effectively promotes resilience and breastfeeding self-efficacy. However, the role-play method is more effective than standard methods in promoting resilience and breastfeeding self-efficacy. We recommend role-playing and routine methods as therapeutic care methods in clinical settings at the beginning of infants’ admission to the NICU to improve maternal resilience and breastfeeding self-efficacy.

