










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkBoletín médico del Hospital Infantil de México
versión impresa ISSN 1665-1146
Bol. Med. Hosp. Infant. Mex. vol.71 no.3 México may./jun. 2014
Artículo de investigación
Child Development Evaluation Test analysis by field improves detection of developmental problems in children
Antonio Rizzoli-Córdobaa,*, Lourdes Schnaas-Y-Arrietab, Fernando Ortega-Riosvelascoa, Evelyne Rodríguez-Ortegac, Miguel Ángel Villasís-Keeverd, Daniel Aceves-Villagráne, Gabriel O''Shea-Cuevasf y Onofre Muñoz-Hernándezg
a Neurodevelopmental Research Unit, Hospital Infantil de México Federico Gómez, Mexico City, Mexico.
b Subdepartment of Public Health Investigation, Instituto Nacional de Perinatología Dr. Isidro Espinosa de los Reyes, Mexico City, Mexico.
c Department of Public Policy, Hospital Infantil de México Federico Gómez, Mexico City, Mexico.
d Clinical Epidemiology Investigation Unit, Unidad Médica de Atención Especializada Hospital de Pediatría, Centro Médico Nacional S. XXI, IMSS, Mexico City, Mexico.
e Opportunities Program General Management, National Commission of Social Health Protection, Mexico City, Mexico.
f National Commission of Social Health Protection, Mexico City, Mexico.
g Research Division, Hospital Infantil de México Federico Gómez, Mexico City, Mexico.
* Corresponding author:
A. Rizzoli-Córdoba.
E-mail: antoniorizzoli@gmail.com
Received 4 May 2014;
accepted 19 M ay 2014.
Abstract
Background: The Child Development Evaluation (CDE) Test is a screening instrument for developmental problems. In the validation study, a sensitivity of 81% and a specificity of 61% were reported, considering a cut-off value for both a total development quotient (TDQ) of 90. Given that the TDQ is obtained by calculation of the five evaluated fields in the Battelle Development Inventory, 2nd edition (BDI-2), it may occur that a child is classified as a false positive (TDQ ≥90) and may have a developmental delay in at least one of the fields (true positive). The objective of this work was to evaluate if the properties of the CDE Test are different when analyzing each field for the probability of a developmental delay.
Methods: The information obtained for the study from the validation (Rizzoli-Córdoba, 2013) was analyzed. In the CDE Test, a true positive was considered when the result was yellow or red. A developmental delay was considered per domain with a scale score <80 in the BDI-2. The results were analyzed based on the correlation of what was evaluated between the CDE Test and the BDI-2.
Results: For 438 children of 1- to 60-months of age, sensitivity (S) and specificity (Sp) per field were as follows: a) Motor: S=84.3% and Sp=87%; b) Communication: S=79.5% and Sp=79.4%; c) Personal-Social: S=86.9% and Sp=85%; d) Adaptive: S=91.7% and Sp=85.1%; and e) Cognitive: S=83.6% and Sp=88.8%.
Conclusions: When analyzing each field separately, better scores for the CDE are observed compared with those reported for the TDQ in both sensitivity and specificity.
Key words: The Child Development Evaluation Test (prueba EDI); Child Development; Screening; Battelle.
1. Background
"The birth of a human being is comparable to a person at a train station that boards a steam for the first time (its body) that will accompany him/her for the rest of his life journey, to be able to reach his/her destiny. During the first five years of age there are no deviations or intersections on the road (which is determined by parents, family and caretakers), this because the boy or girl can focus on getting to know the train engine and learn, amongst other things: where to put the wood and have energy for the ride (feeding and adapting to the environment); how to run it and decide what direction to take (motor aspects), how to understand the present signs along the way and what other driver of other trains might say (communication), to remember each process and to learn what he/she sees, hears, imagines and thinks (cognitive aspects), to learn to relate to other train drivers (pair interaction), to follow the rules and respect limits (adult interaction) and to learn what his/her role is in the world (social role), as well as the ability to take care of him/herself (self care) with personal responsibility. All this happens during the first five years, so that starting from six years old, with all the obtained abilities, this will allow him/her to make the correct decisions when there are intersections along the rail, to drive without affecting others by respecting the rules and to be able to enjoy the landscape and pay attention to details to learn, grow and make their dreams come true"
(Rizzoli, unpublished).
Because of the above, the first 5 years of age are a critical period during which children learn to understand and interact with the world around them, establishing the basics that will allow them to abstract in the future all the concepts to be independent, to solve problems, to plan and reach their goals, to be able to have effective communication, to establish and maintain adequate interpersonal relationships, all these to have the necessary tools to reach their maximal potential.
Evaluation of childhood development is a process destined to learn and quantify the level of maturity that a child reaches compared to a group of children the same age. This process requires the administration of standardized tests that evaluate the different domains of child development. During February 2012, "Validation of diagnostic instruments of child development in Mexico" was co-organized by the National Commission for Social Health Protection (Mexico) and the expert panel of the World Bank. After analysis of the different diagnostic tests, it was established that the Battelle Developmental Inventory, 2nd edition (BDI-2)1 is the most appropriate diagnostic instrument for developmental delay in Mexico because of the following: a) it is available and validated in a Spanish version; b) it was standardized in Spanish with a high percentage of the Mexican population; c) it can evaluate children from newborn to 7 years, 11 months and the manipulatives can be replaced by others more familiar to the children being evaluated.2
Diagnostic test application (BDI-2) lasts from 1 to 3 h and includes the evaluation of five domains and 13 subdomains: 1) Motor (gross, fine and perceptual), 2) Communication (expressive and receptive), 3) Personal-social (interaction with adults, interaction with pairs, self-concept and social role), 4) Adaptive (personal responsibility and personal care) and 5) Cognitive (perception and concepts, reasoning and academic skills and attention and memory).1
Child development screening tests are tools designed to identify problems within the different domains and consist of general questions to caretakers and the direct observation of behaviour or activities that children perform. Like all screening tests, they have to be easily and quickly applied and also should have a sensitivity (capacity to detect individuals with developmental problems) and specificity (capacity to rule out individuals with developmental problems) >70% when compared to gold standards.3 During analysis of the psychometric properties already published for screening tests in the U.S. (found in a review from 1980 to 2012), we observed a great heterogeneity in the quality of the tests because they had gold standard selection problems, sample size, age ranges, and a great variety of sensitivity and specificity values.4
The Child Development Evaluation (CDE) Test is a screening tool designed and validated5 in Mexico for the early detection of developmental problems in children from 1 month of age to 1 day before their 5th birthday. This evaluation takes place through the evaluation of five axes6 described in Table 1. For each item, the corresponding mode of application is specified: a) direct observation of the child, or b) targeted questions for the caregiver.7 In Table 2 the components of the developmental domains evaluated in the BDI-2 (diagnostic test) are described as well as the relationship of each with the questions among the developmental areas of the CDE Test (screening tool).
Possible tests results of the CDE Test are a) Normal development (green): the child has reached the corresponding milestones for his/her age group and has no sign of disturbance during the neurological physical exam; b) Developmental delay (yellow): the child has not reached the corresponding milestones for his/her age group but he/she does complete the milestones of the previous age and has no signs of disturbance during the neurological physical exam; and c) Retardation risk (red): the child has not reached the corresponding milestones for his/her age group or the immediate previous age group or else presents disturbances during the neurological physical exam. For both yellow and red results, the child is considered to have developmental problems.8
As part of the process to determine confidentiality of the CDE Test, a concurrent validation was designed in which we used the Battelle Developmental Inventory, 2nd Edition in Spanish or BDI-2 as a gold standard. We used in the diagnostic test as a limit for normal development a value for Total Development Quotient (TDQ) ≥90, determining a sensitivity of 81% (95% CI: 75-86%) and specificity of 61% (95% CI: 54-67%) for all domains (in all age groups).5
It was mentioned in an editorial9 that the specificity for the CDE Test is low compared to other tests in Latin America. It may be possible that this low specificity is due to the identification of "false positive" results, given that the CDE Test catalogues them as normal even though they may have delay in at least one domain or that in fact it does have a low specificity with a high incidence of true false positives. In order to answer this question, the goal of the present study is to evaluate the capacity of the CDE Test (especially specificity) according to each domain in order to be able to identify patients with the probability of having a developmental delay.
2. Methods
The present study presents part of the analysis of the information obtained during the validation study. The design characteristics and inclusion and exclusion criteria as well as the information recollected and global results have been previously described.5 Briefly, it was a cross-sectional study that included 438 children aged from 1 month to 1 day before their 5th birthday and who lived in an urban, suburban or rural environment in three Mexican states: Chihuahua, Yucatán and Distrito Federal. The spectrum of the population included those with biological risk factors as well as environmental risk factors and no risk factor for developmental delay. Patients with evident neurological disturbances were excluded. As gold standard, the Battelle Developmental Inventory, 2nd edition in Spanish1 (BDI-2) was used. The CDE and the BDI-2 Tests were applied to each participant on the same day or with a time frame no longer than 1 week. The person who applied the BDI-2 did not know the result of the screening test. The results of the tests and the information acquisition were performed centrally. The CDE Tests considered a yellow or red result as positive.
For this study, retardation was defined according to scale domains with a result of <80 in the BDI-2. The result was analyzed based on the relationship of what was being evaluated in the CDE Test and each of the domains for the BDI-2. To perform the calculation of sensitivity, the number of participants in the study who had a developmental quotient was used as a denominator, also named scale result, in each domain of <80 and for each of the subdomains a Z-score of less than -1.33 SD, which is equivalent to a developmental quotient of <80. In the numerator of each patient subgroup we considered those who had the above conditions and who had a yellow or red result according to the CDE Test.
To perform the calculation for specificity, the denominator was the total of participants in the study who had a TDQ >80 and for each of the subdomains a Z score of -1.33 SD or higher. The numerator was the patients who accomplished the above and had a normal result (green) in the corresponding screening test.
For each of the estimates, a 95% (CI) was calculated using the following formula:
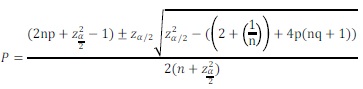
For statistical analysis we used the IBM SPSS version 19 software.
The study was approved by the Investigation, Ethics and Biosafety Commissions of the Hospital Infantil de México Federico Gómez. Parents participating in the study signed an informed consent form.
3. Results
Considering 438 children evaluated, 235 (53.6%) were between 1 and 15 months and 203 (46.3%) were from 16 to 60 months, global sensitivity (the capacity to identify children with developmental problems) for the total CDE score was 81% (95% CI, 75-86%); however, there were important differences for each age group. Sensitivity for the younger age group was 74% (95% CI 65-82%), lower than that reached by the older age group (89%; 95%CI, 82-95%). For specificity (capacity to identify children without developmental problems), this was not seen, given that the global specificity was 61% (95% CI, 54-67%) and for 1- to 15-month-old children it was 60% (95% CI, 51-68%), similar to the results from the 16- to 60-month-old age group (62%; 95% CI, 53-71%).5
As can be appreciated in Tables 3 and 4, when analyzed according to each of the domains, a difference in the global results was determined. In regard to sensitivity (Table 3), the percentages were similar or slightly lower for each domain. For specificity (Table 4) these results show an increase.
Sensitivity in the group of children from 1 to 15 months of age is lower than the older age group, in particular for communication and cognitive domains. On the other hand, for the adaptive domain the sensitivity was higher. In children 16- to 60-months-of-age, a substantial improvement was observed in the following domains: motor and adaptive but lower sensitivity for cognitive (specifically attention and memory). Regarding specificity, even though percentages improved substantially for each domain, reasoning and cognitive domain abilities had the lower values of the domains.
The cognitive domain (BDI-2) is evaluated in all ages using the CDE Test through items distributed in different axes: alert or alarm signs, or in the developmental areas: fine motor, language or knowledge. The knowledge area of the CDE Test is only evaluated in children from 36 to 59 months of age and is focused on evaluating specific aspects of this domain that have a direct association with the bases of preschool (attention and memory; perception and concepts). Sensitivity of the test for this domain was 83.6% (95% CI: 76.4-88.4%), being much better for children from 16 to 59 months (86.2%; 95% CI: 76.7-91.5%) compared to children of 1 to 15 months old (79.7%; 95% CI: 66.8-87.3%). In the analysis for the subdomains, we can see that the lowest result (60%) and the highest result (85.7%) fall within the same subdomain (perception and concepts). The lowest is for the age group from 1 to 15 months where children still do not possess the vocabulary to express concepts, and the highest one is associated with the presence of specific items from the knowledge area (age group 36 to 59 months) where it is greatly focused on concepts and academic abilities. The specificity analysis could only be performed in the subgroups of 36-59 months, and it reports a value of 88.8% for the domain (95% CI: 80.4-93.3%), the highest value for attention and memory (90.4%; 95% CI: 82.1-94.5%), and the lowest for reasoning and academic abilities (59.6%; 5% CI I5%: 44.3%-71.4%).
4. Discussion
Diagnosing developmental problems presents multiple challenges that involve different domains and there is no perfect gold standard. A frequent thought is that neuroimaging or electroencephalographic studies are needed to confirm the diagnosis.10 Electroencephalogram is only useful for epilepsy and there can be developmental delay without graphic confirmation, which is why these studies are not necessary for diagnosis (except for diseases with specific clinical findings). Within this process, the administration of tests constitutes a central element that can measure the level of the abilities by establishing a developmental quotient.2 These diagnostic tests have different characteristics and properties per se, and their properties change depending on the limits used for each. Therefore, children with an illness who have not been identified by the gold standard (false negative in the tests) can be identified by screening tests and it would appear that they are false positives, which reduces specificity. As described in the original validation article,5 only 1.3% of children who had no results on a scale below -1 standard deviation (SD) had a TDQ of <90 that corresponds to a "false negative" of the CDE, whereas 84% and 23.9% of the children who had a scale of less than -1 SD in one or two areas, respectively, had a TDQ ≥90, which is a "false positive." This highlights the importance of the analysis by domains.
For calculation of the sensitivity by domain, we decided to consider the total result and not by axis or area from the CDE Test, given that there are different axes within the test (developmental areas, alert, alarm and physical exam) that evaluate the aspects of a same developmental domain (BDI-2). For example, for the age group of 31-36 months, the corresponding abilities for the communication domain (both receptive and expressive) are evaluated in the areas of development (language) as well as7 a) alert signs axis: 12.2: Is it difficult for the child to understand simple instructions such as: go to mom? and 12.3: Does he make eye contact when you talk to him/her? and b) alarm signs axis: 12.1: Does he drool constantly or talk in a noncomprehensive manner? and 12.2: Does he communicate with isolated words or does he make sentences such as: mom I want milk, or does he only say milk? This was performed so that problems could be evaluated or asked in different axes and to provide a greater opportunity for problems to be detected. This analysis shows higher values of sensitivity for children in the 16- to 60-month-old age group, consistent with the results when taking as a limit the TCQ. For each of the domains we find similar values from those reported in a general manner, being highest for the adaptive domain (91.7%) and lower for communication domain (79.5%), especially for the receptive communication subdomain (74.4%). For the cognitive domain, sensitivity in the age subgroup of 1 to 15 months was 79.7%, being the lowest of all tests for the perception and concept subdomain (60%). This is due, in a great part, to the fact that children of that age normally have a limited vocabulary, making this evaluation more difficult.
Given that the specificity is the percentage of persons who are identified as normal in the CDE Test (green or normal), and there are areas within the CDE Test that correlate directly with each domain, this is why we selected only the result for each developmental area (gross and fine motor skills within the motor domain; language within the communications domain; social within the personal-social domain and adaptive domain; knowledge within the cognitive domain) to insert the numerator to calculate the specificity of the test for each domain.
On the alarm signal axis we included selected items associated directly with the developmental domain (for example, ALA 9.2: Does he/she walk alone?, ALA 13.1: can he/she copy a circle on a piece of paper? and ALA 14.1: Can he/she pronounce correctly his/her name and surname?) or those suggestive of neurological diseases (from a regressive syndrome: Does the mother report that her child has experienced a loss of important and constant abilities that he/she once possessed?; from autism: Does he/ she show repetitive or stereotypical conducts, for example, balance him/herself on a chair nonstop or hits his/her head with his/her hands?). For these reasons everything should be analyzed separately. The fact that it may be present (red result) does not imply that there is a specific delay in a certain domain. This is the reason why we excluded this category for the specificity analysis for each domain.
One of the exclusion criteria for the study was the presence of evident abnormalities during a neurological physical exam, given that the questions from the CDE Test for this axis can be identified easily (significant increase or decrease on cephalic perimeter, extremity, face or eye movement asymmetries). We did not include any patients who had any of the previous alterations on the axis, which is why we do not present any information related to the neurological physical exam. If a child with a risk of developmental delay from any of the above-mentioned for the axis, a complementary neurological evaluation9 should be performed and the appropriate treatment that allows as far as possible to prevent or diminish the development of certain disabilities should be applied.2
While performing the calculation for specificity using exclusively the results from the normal areas of development with which domains relate to, we observed an important increase in specificity of all age groups >61% as a global value to values of 79.4% (communication domain) to 88.8% (cognitive domain). This relates to the fact that the gold standard stipulates the results of the different domains and subdomains for a total quotient, which is why a normal quotient does not necessarily implicate absolute normality in all domains. For example, in children 16 to 60 months, 89.3% with a delay in the motor domain have an abnormal result on the CDE Test, whereas 87% with a normal value in this same domain have a green result in the gross motor developmental area on the CDE Test.
While analyzing each domain separately, we observe better values for the CDE Test compared to that reported on the validation study, for both sensitivity and specificity. As such, quotients for each domain (QEC) stipulate the results for the subdomains that are being evaluated, which is why a child may have a QEC ≥80 and have a delay in some of the subdomains. On field application, if a subdomain is identified with a low score, we have to consider that there is a delay in such subdomain and establish an improvement plan.
The lowest values obtained were for the communication domain, which is why it is fundamental to perform auditory screening at the recommended stages11 as a complementary evaluation of child development (ECD).
Given that the original objective of this study was to evaluate the psychometric properties of the CDE Test, we searched for accurate representation for each type of delay risk and not for a population <5 years of age or that represents the general population of the country or each of the states. In some cases the population sample was very small, resulting in wide CIs. It is important to consider not only the punctual values but the CI to interpret results for each domain.
From a clinical point of view, it is useful to plan feedback and counselling regarding the results in each of the areas of the CDE Test. Results on a population base (or a representative sample of such population) are necessary in order to be able to obtain predictive results.
In conclusion, the CDE Test is a validated instrument in Mexico with studied psychometric properties and with adequate values, which makes it the recommended instrument for the evaluation of development in children <5 years of age in Mexico.12 The global result of the CDE Test for detection of children with developmental problems is very useful, given that there may be affected areas or domains. In children 1- to 15-months of age, the values are lower and it is fundamental to perform a clinical evaluation to rule out other problems. It is fundamental to complement the evaluation with the auditory screening test. In children >16 months of age, higher values are obtained, and it is important to establish individualized profiles for each of the subdomains while applying the diagnostic test (BDI-2) to be able to perform adequate preventive or therapeutic actions.3 It is recommended to provide individualized counselling by considering the result from each of the axes and areas of the CDE Test.
Funding
The study was carried out with funding from the CPSS/ ART.1°/128/2011 agreement between the Hospital Infantil de México Federico Gómez and the National Commission for Social Health Protection (CNPSS).
Conflicts of interest
The author declares no conflicts of interest of any nature.
Acknowledgments
a) Hospital Infantil de México Federico Gómez: General Direction (José Alberto García Aranda, Judith Torres Mujica, Claudia Esmeralda Martínez González, Irene Solana Barbosa and Laura Elena García Ojeda), Research Division (María del Carmen Martínez García, Elías Hernández Ramírez, Ana Alicia Jiménez Burgos y Ana Lilia González Camacho), Neurodevelopment Research Unit (Mariel Pizarro Castellanos, Guillermo Buenrostro Márquez, Beatriz Romo Pardo, Silvia Liendo Vallejos, Marta Lia Pirola and Rocío del Carmen Córdoba García); b) Opportunities Program, National Commission for Social Health Protection (Fátima Adriana Antillón Ocampo, Joaquín Carrasco Mendoza, Julieta Medina Santos, María Esther Valadez Correa and Jorge Carreón García); c) National Center for Adolescent and Childhood Health (Ariana Bernal Zamora, María Magdalena Solares Llamas and Amanda Mendoza Martínez), d) Víctor Hugo López Aranda and Iván Rivas Rodríguez, e) Interamerican Development Bank (Caridad Araujo, Ricardo Pérez Cuevas), f) State Coordination for Opportunities Program (in alphabetical order) of Chihuahua (Olga Susana Lira Guerra, Edgar Flores Pérez) and Yucatán (Heidi de Lourdes Río Hoyos, Roberto Robles Anaya, Amalia Reyes Peón).
References
1. Newborg J. Battelle Developmental Inventory (Spanish version). Ithaca, IL: Riverside Publishing; 2005. [ Links ]
2. Comisión Nacional de Protección Social en Salud. Manual para la evaluación de menores de cinco años con riesgo de retraso en el desarrollo. México D.F.: Secretaría de Salud; 2013. p. 88. [ Links ]
3. Rydz D, Srour M, Oskoui M, Marget N, Shiller M, Birnbaum R, et al. Screening for developmental delay in the setting of a community pediatric clinic: a prospective assessment of parent-report questionnaires. Pediatrics. 2006;118:e1178-e1186. [ Links ]
4. Romo-Pardo B, Liendo-Vallejos S, Vargas-López G, Rizzoli-Córdoba A, Buenrostro-Márquez G. Pruebas de tamizaje de neurodesarrollo global para niños menores de cinco años de edad validadas en Estados Unidos y Latinoamérica: revisión sistemática y análisis comparativo. Bol Med Hosp Infant Mex. 2012;69:450-62. [ Links ]
5. Rizzoli-Córdoba A, Schnaas-Arrieta L, Liendo-Vallejos S, Buenrostro-Márquez G, Romo-Pardo B, Carreón-García J, et al. Validación de un instrumento para la detección oportuna de problemas de desarrollo en menores de 5 años en México. Bol Med Hosp Infant Mex. 2013;70:195-208. [ Links ]
6. Comisión Nacional de Protección Social en Salud. Manual complementario para la aplicación de la prueba Evaluación del Desarrollo Infantil "EDI". México D.F.: Secretaría de Salud; 2013. p. 168. [ Links ]
7. Comisión Nacional de Protección Social en Salud. Manual para la aplicación de la prueba Evaluación del Desarrollo Infantil "EDI". México D.F.: Secretaría de Salud; 2013. p. 168. [ Links ]
8. Dirección General del Programa Oportunidades. Guía operativa de la Estrategia de Desarrollo Infantil. México D.F.: Comisión Nacional de Protección Social en Salud; 2014. [ Links ]
9. Comisión Nacional de Protección en Social en Salud. Manual de exploración neurológica para niños menores de cinco años en el primer y segundo nivel de atención. México D.F.: Secretaría de Salud; 2013. p. 64. [ Links ]
10. Flores-Huerta S. La importancia de las pruebas para evaluar el neurodesarrollo de los niños. Bol Med Hosp Infant Mex. 2013; 70:175-7. [ Links ]
11. Secretaría de Salud. Proyecto de Norma Oficial Mexicana PROY-NOM-034-SSA2-2010, Para la prevención y control de los defectos al nacimiento. México D.F.: Diario Oficial de la Federación (DOF); 2010. [ Links ]
12. Centro Nacional para la Salud de la Infancia y la Adolescencia. Desarrollo Infantil Temprano: Lineamientos Técnicos. México D.F.: Secretaría de Salud; 2014. [ Links ]

