











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkFloating right heart thrombus is rare, occurring in 3.8% of patients with pulmonary embolism (PE)1. A right to left shunt can let the thrombus pass to systemic circulation, causing a paradoxical embolism. Patent foramen ovale (PFO) is the most associated congenital heart defect. If the thrombus is larger than the foramen, an even rarer condition can arise, an impending paradoxical embolism (IPE)2. With a high mortality rate, the management requires emergency intervention to prevent systemic embolization3. Here, we describe the case of a patient with an IPE in which anticoagulation solely was effective.
An 80-years-old male patient presented to emergency with tachycardia. Seven days before, he suffered pleuritic chest pain and hemoptysis; 2 days before admission, sudden dyspnea at rest. The chest X-ray showed bilateral radiopacity and effacement of both costophrenic angles, atrial fibrillation was featured in EKG and an emergent CT pulmonary angiography revealed PE. The transthoracic echocardiography (TTE) at subcostal view and transesophageal echocardiography (TEE) showed a serpentine image that appeared to be a thrombus through PFO (Fig. 1A-C). It was proximal to the tricuspid valve and attached to the septal wall of the left atrium.
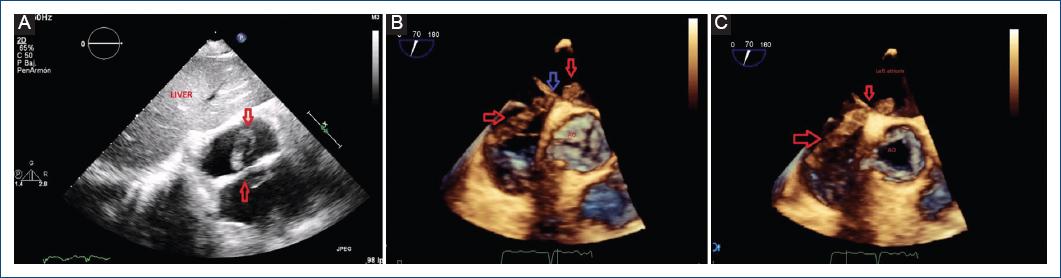
Figure 1 A: transthoracic echocardiography, subcostal view. The red arrows show a serpentine thrombus through the patent foramen ovale. In the right atrium, it is proximal to the tricuspid valve. B: transesophageal echocardiography. The red arrows show a serpentine thrombus through the patent foramen ovale. The blue arrow shows the patent foramen ovale. In the middle of the image, the aortic valve is seen closed. C: transesophageal echocardiography. The red arrows show a serpentine thrombus through the patent foramen ovale. In the middle of the image, the aortic valve is seen opened. AO: aorta.
The patient was diagnosed with IPE of which the etiology was the thrombus in transit, that developed into an acute decompensated heart failure. He was scheduled for surgery and remained on anticoagulation therapy. Clinical condition improved over the following days. In a pre-operative TTE (Fig. 2), complete resolution of the thrombi was evident.
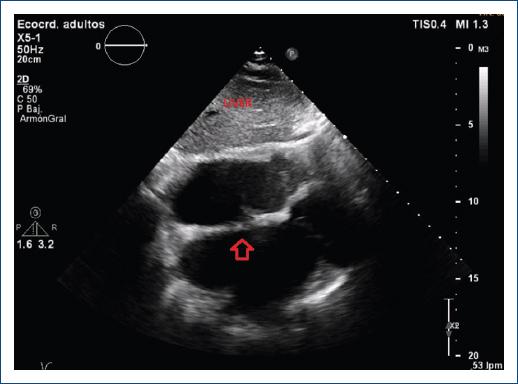
Figure 2 Transthoracic echocardiography, subcostal view. Image taken after finishing the treatment of the patient. The serpentine thrombus had disappeared and the foramen ovale was occluded.
This case contains many striking aspects. An IPE is an extremely rare finding in clinical practice, this being one of the few described in the literature. Due to the fact that it is a life-threatening condition because of the risk of systemic embolization, an early diagnosis must be made. Echocardiography, specially TEE, has an important role in making a correct and timely diagnosis. Finally, optimal management of IPE remains unclear due to the lack of guidelines or randomized and controlled trials addressing the issue. The success in this case encourages us to consider anticoagulation therapy as an effective option, particularly if surgery is not available. However, the decision must be individualized.

