











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Abdominal aortic aneurysm (AAA) is a pathology that primarily affects people over the age of 651. A greater number of patients will require AAA intervention due to the ongoing population aging in developed countries, which is predicted to triple the number of older patients by the year 20402,3. Accordingly, between the years 1994-1999 and 2010-2014, the number of AAA repairs in Sweden tripled, from 13 to 36/10,000 people, with endovascular aneurysm repair (EVAR) being the most popular treatment2. EVAR has replaced surgery as the preferred therapy for treating older patients due to its less invasive nature and lower morbidity and mortality rates3-6. Actually, 80% of older patients with AAA are successfully treated with endovascular therapy7. Data on EVAR in octogenarian patients are contradictory, and although the success rate of the procedure is high, post-procedural and long-term complications are often higher when compared to younger patients1,8-15.
Our goal is to compare the EVAR outcomes between patients under and over the age of 80 in terms of the procedure's safety as well as immediate and long-term outcomes.
Material and methods
Population and study design
In a retrospective cohort study, we included patients who had been diagnosed with an uncomplicated infrarenal AAA and were suitable candidates for endovascular repair. Patients who underwent EVAR between 2011 and 2017 at a tertiary referral hospital in Buenos Aires were included in the study.
Trauma related and inflammatory AAA etiology, complicated AAA and anatomy deemed unsuitable for traditional infrarenal stent grafting (such as short or absent necks, angulated necks, conical necks, or large necks exceeding the size availability for current stent grafts) were exclusion criteria.
The electronic health records were used to carry out the follow-up. Patients who did not follow-up at our facility were called by phone. The physician's preference determined the endovascular repair method as well as the prosthesis selection and application technique. At the time of the EVAR implant, patients were divided into two groups: Those who were 80 or older (octogenarians) and those who were younger than 80.
The Glasgow aneurysm score, which takes into account factors like age, shock at the time of presentation, and prior medical history of coronary, cerebral, and renal disease, was used to assess surgical risk. The score was determined using the formula: total score = (age [years]) + 7 (if coronary artery disease) + 10 (if cerebrovascular disease) + 14 (if renal disease) + 17 (if shock at admission was present). Coronary artery disease was defined as having previously experienced an acute or chronic coronary syndrome, cerebrovascular disease as having previously experienced a stroke or transient ischemic attack, and renal disease as having previously experienced an acute or chronic renal failure in the past. Finally, shock was defined as the presence of hypotension during admission (systolic arterial pressure < 90 mmHg), with tachycardia (> 90 beats per min), or any clinical signs of hypoperfusion16.
Study outcomes
Primary outcomes included hospital mortality, length of stay, post-procedure incidence of acute renal failure, and need for reinterventions. Post EVAR follow-up (regarding imaging and clinical follow-up) was done according to the preference of the physician.
Secondary outcomes included aneurysm-related mortality at follow-up, incidence of acute myocardial infarction, stroke, acute limb ischemia, and need for prolonged mechanical ventilation in the immediate post-operative period.
Definition of outcomes
Hospital mortality was defined as all-cause death during the index hospitalization or within 30-day post-procedure.
Acute kidney failure was defined as a rise in serum creatinine of at least 0.3 mg/dL or an increase of at least 50% from pre-procedure levels17. Reinterventions were defined as any surgical or endovascular treatment related to the primary EVAR. Acute myocardial infarction was defined according to the fourth universal definition18. A stroke was defined as cerebral ischemia due to a thrombotic, embolic, or systemic hypoperfusion event, or hemorrhagic due to intracerebral or subarachnoid bleeding19. Acute limb ischemia was defined as having limb hypoperfusion symptoms and signs within 2 weeks of EVAR20. The need for invasive ventilatory support for more than 72 h after a procedure was referred to as prolonged mechanical ventilation. Endoleaks were defined as an imaging evidence of perfusion to the aneurysm sac after procedure, and classified according to international guidelines21.
Statistical analysis
Continuous variables were analyzed using the t-test or the Mann-Whitney U test, depending on their distribution and were expressed as mean and standard deviation, median, and interquartile range. Categorical variables were analyzed using Chi-square or Fisher exact test and expressed as count and percentage. Freedom from re-intervention analysis was performed with the Kaplan–Meier curve, and analyzed using the log rank test. The relationship between the need for reinterventions and important clinical variables was assessed using a cox proportional regression analysis. The Cox multivariate analysis included the variables that showed up with p = 0.1 and were thought to be potentially confounding variables. The results were shown as hazard ratios along with their corresponding 95% confidence intervals. p < 0.05 was considered statistically significant. All analyses were performed using stata 14.0 (Stata Corp, Texas, USA).
Results
There were 123 patients in total, 77 (62.6%) of whom were under the age of 80, and 46 (37.4%) were octogenarians. The median follow-up was 34 months (18-49 months), and only two (1.6%), both in the under 80 age group, were lost in the follow-up.
Table 1 describes the demographic characteristics of the population. The average age of those under the age of 80 was 71.6 ± 5.1 years, and that of those over 80 was 85 ± 3.5 years. Male sex prevailed in both groups (92.2% vs. 82.6%, p = 0.11). There were no differences in the diameter of the AAA between groups (5.4 cm [4.9-6.2 cm] in younger patients vs. 5.4 [5-6 cm] in octogenarians, p = 0.53). The younger group had a higher prevalence of tobacco consumption (72.7% vs. 41.7%, p < 0.01), while older patients had a higher Glasgow Aneurysm Score (88 [83-96] vs. 77 [72-81], p < 0.01).
Table 1 Demographic characteristics
| Characteristics | Total (n = 123) | Non octogenarians n = 77 (62.6%) | Octogenarians n = 46 (37.4%) | p-value |
|---|---|---|---|---|
| Age, mean (± SD) | 76.7 (7.9) | 71.6 (5.1) | 85.0 (3.5) | < 0.01 |
| Male sex (%) | 109 (88.6) | 71 (92.2) | 38 (82.6) | 0.11 |
| AAA diameter (IQR) | 5.4 (5.0-6.0) | 5.4 (4.9-6.2) | 5.4 (5.0-6.0) | 0.53 |
| Hypertension (%) | 104 (84.6) | 64 (83.1) | 40 (87.0) | 0.57 |
| Dyslipidemia (%) | 72 (58.5) | 52 (67.5) | 20 (43.5) | < 0.01 |
| Diabetes mellitus (%) | 21 (17.1) | 12 (15.6) | 9 (20.0) | 0.57 |
| Tobacco consumption (%) | 77 (62.3) | 56 (72.7) | 21 (41.7) | < 0.01 |
| Chronic obstructive pulmonary disease (%) | 17 (13.8) | 10 (13.0) | 7 (15.2) | 0.73 |
| Chronic renal failure (%) | 22 (17.9) | 10 (13.0) | 12 (26.1) | 0.07 |
| Coronary artery disease (%) | 39 (31.7) | 29 (37.7) | 10 (21.7) | 0.07 |
| Peripheral vascular disease (%) | 10 (8.1) | 7 (9.1) | 3 (6.5) | 0.61 |
| Stroke (%) | 4 (3.3) | 3 (3.9) | 1 (2.2) | 0.60 |
| Abdominal surgery (%) | 31 (25.2) | 20 (26.0) | 11 (23.9) | 0.80 |
| Previous aortic surgery (%) | 3 (2.4) | 3 (3.9) | 0 (0) | 0.18 |
| Glasgow Aneurysm score, median (IQR) | 81 (75-88) | 77 (72-81) | 88 (83-96) | < 0.01 |
AAA: abdominal aortic aneurysm; IQR: interquartile range.
Regarding the primary outcome, neither group experienced intra-hospital mortality. The most common complication in both groups, acute kidney injury, was present in 14.3% of younger patients and 23.9% of octogenarians; however, there were no differences between the groups (p = 0.18). In addition, only one octogenarian patient required dialysis during long-term follow-up, while this complication was not observed in any younger individual (p = 0.20). The intra-hospital complications are described in table 2. In comparison to the younger group, the octogenarians' length of stay was longer (3 days [2-4 days] vs. 2 days [2-3 days], p = 0.04; Fig. 1). Although not statistically significant, the number of reinterventions was numerically higher in the octogenarians (7 [15.2%] vs. 4 [5.3%], p = 0.11; Fig. 2). Endoleaks were the most common cause for additional treatment (nine out of 11 re-interventions: 81.8%), with a prevalence of 34% across the entire cohort. Table 3 summarizes the distribution of the types of endoleaks found. Other types of reinterventions included one conversion to surgery due to technical difficulties in a younger patient and one conversion to surgery due to the occlusion of an endoprotesis in an octogenarian patient.
Table 2 Primary and secondary outcomes
| Outcomes | Total (n = 123) | Non octogenarians n = 77 (62.6%) | Octogenarians n = 46 (37.4%) | p-value |
|---|---|---|---|---|
| Primary outcomes | ||||
| Intrahospital mortality (%) | 0 (0) | 0 (0) | 0 (0) | NA |
| Length of stay, days, median (IQR) | 2 (2-3) | 3 (2-4) | 0.04 | |
| Acute kidney injury (%) | 22 (17.9) | 11 (14.3) | 11 (23.9) | 0.18 |
| Reinterventions (%) | 11/121 (9.1) | 4/75 (5.3) | 7/46 (15.2) | 0.11 |
| Secondary outcomes | ||||
| Aneurysm related death during long-term follow-up (%) | 1/121 (0.8) | 0/75 (0) | 1/46 (2.2) | 0.20 |
| Prolonged mechanical ventilation (%) | 1 (0.8) | 0 (0) | 1 (2.2) | 0.19 |
| Acute myocardial infarction (%) | 2 (1.6) | 1 (1.3) | 1 (2.2) | 0.71 |
| Stroke (%) | 1 (0.8) | 0 (0) | 1 (2.2) | 0.19 |
| Acute limb ischemia (%) | 5 (4.1) | 2 (2.6) | 3 (6.5) | 0.29 |
IQR: interquartile range.
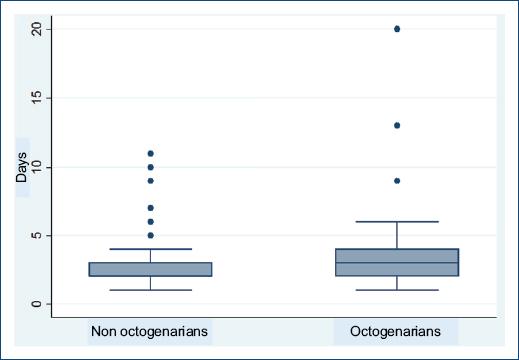
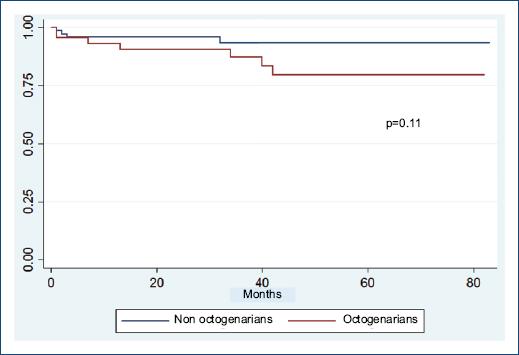
Table 3 Endoleak type at follow-up
| Endoleak type | Total (n = 106)* | Non octogenarians n = 68 (64.2%) | Octogenarians n = 38 (35.8%) | p-value |
|---|---|---|---|---|
| Type I (%) | 5 (4.7) | 2 (2.9) | 3 (7.9) | 0.25 |
| Type II (%) | 25 (23.6) | 17 (25.0) | 8 (21.1) | 0.65 |
| Type III (%) | 2 (1.9) | 0 (0) | 2 (5.3) | 0.06 |
| Type IV (%) | 4 (3.8) | 1 (1.5) | 3 (7.9) | 0.10 |
| Total endoleaks (%) | 36 (34.0) | 20 (29.4) | 16 (42.1) | 0.19 |
| Endoleaks that required intervention (%) | 9 (8.5) | 3 (4.4) | 6 (15.8) | 0.04 |
*Data for endoleaks were present in 106 out of 123 patients.
Regarding secondary outcomes, there was a unique aneurysm related death during follow-up, in an octogenarian patient. There were no differences in the other outcomes, such as myocardial infarction (2.2% vs. 1.3%, p = 0.71), stroke (2.2% vs. 0%, p = 0.19), acute limb ischemia (6.5% vs. 2.6%, p = 0.29), and prolonged ventilatory support (2.2% vs. 0%, p = 0.19).
In the multivariable Cox regression model, the AAA diameter was independently associated with the requirement of reinterventions, after adjusting for age, female sex, tabacco consumption, and Glasgow Aneurysm score (HR: 1.96, 95% CI: 1.24-3.10, p < 0.01; Table 4).
Table 4 Cox multivariable regression model for risk of reinterventions at follow-up
| Variable | HR | Standard error | z-value | p-value | 95% Confidence Interval |
|---|---|---|---|---|---|
| Age | 1.10 | 0.08 | 1.43 | 0.15 | 0.96-1.27 |
| Female sex | 1.32 | 1.09 | 0.33 | 0.74 | 0.26-6.64 |
| AAA diameter | 1.96 | 0.46 | 2.88 | < 0.01 | 1.24-3.10 |
| Tobacco consumption | 0.36 | 0.25 | −1.48 | 0.14 | 0.09-1.39 |
| Glasgow Aneurysm score | 0.97 | 0.05 | −0.69 | 0.49 | 0.88-1.06 |
AAA: abdominal aortic aneurysm.
Discussion
The main findings of our study are that EVAR represents a safe procedure as no intrahospital mortality was found among the cohort. Second, the length of stay was longer in octogenarian patients when compared to a younger group. Third, immediate postoperative complications such as acute kidney injury, acute myocardial infarction, stroke, acute limb ischemia, and prolonged mechanical ventilation did not show any statistically significant differences between the groups. Fourth, although not statistically significant, the number of re-interventions was numerically higher in octogenarian patients, but there were no differences in the rate of aneurysm related death during long-term follow-up between the two groups.
Due to the rising prevalence of a high-morbidity population, such as the older patients, AAA repair represents a challenging scenario1. Even though EVAR has demonstrated advantages over surgery due to its less invasive nature, research on the variations in outcomes for a more morbid population, such as the octogenarian patients, is still required3-6.
Our study, which compares differences between octogenarians and a younger population with its distinct ethnic characteristics, is the first of its kind in Latin America.
As was previously mentioned, differences in pre-procedural baseline characteristics between groups should be taken into account. One such example is the younger group's higher prevalence of tobacco use. This supports a prior meta-analysis by Han and colleagues that focused on the contribution of tobacco to the development of AAA in younger patients1. Consequently, the main risk factor for the development of AAA is tobacco use22,23. On the other hand, as defined by the Glasgow aneurysm score, octogenarians represent a more morbid population, highlighting the importance of the distinctive risk profile of the population that will be treated with EVAR.
In terms of the post-procedure outcomes, we did not describe any statistically significant variations between the groups in terms of important complications like acute kidney injury. However, it is important to note that this complication was more frequent in the group of octogenarian patients, and a statistically significant difference was probably not observed due to the small number of the sample. In addition, no significant impact on dialysis requirement was demonstrated during long-term follow-up in the entire cohort of patients.
Likewise, the length of stay was significantly longer in octogenarians compared to younger patients. In addition, although we did not examine the AAA's anatomical features, prior research indicates that older patients have an anatomy that is more unfavorable for EVAR (more angulated and conical necks, larger calcium volumes in the aorta)1,4,10. These variations could be the cause why EVAR procedures take longer, result in more procedural complications such as acute kidney injury, and extend hospital stays for older patients.
The previous research has shown conflicting outcomes regarding differences in intrahospital mortality in older patients1,10,14,15,24. This is supported by the fact that we did not describe statistical differences in mortality or mortality related to aneurysms; as a result, EVAR should be taken into consideration for octogenarian patients, if life expectancy and functional status are appropriate.
Regarding long-term follow-up findings, we observed a numerically higher rate of reinterventions in older patients without reaching statistical significance. The most common cause for reinterventions in octogenarians was the existence of endoleaks, which could be due to the increased complexity in the anatomy of the AAA described in the previous research1,4,10.
As the decision for treatment is greatly influenced by factors such as quality of life, procedural risks, the anatomical complexity of AAA, and life expectancy, a team that includes cardiologists, vascular surgeons, interventional radiologists, anesthesiologists, and geriatricians should be formed.
Due to our study's retrospective and non-randomized design, it has some limitations, such as selection bias, which could select "healthier" older patients or a more morbid younger group, explaining the differences found. Second, the external validity of the findings may be impacted by the fact that our data are derived from a single, highly complex center. Third, our small sample size may reduce the study's ability to detect subtle differences. Finally, neither the impact on patients' quality of life nor the anatomical complexity of the AAA were taken into consideration.
Conclusion
EVAR represents a safe and effective procedure for octogenarian patients. Although there was no intra-hospital mortality in our study, older patients had a numerically higher requirement of reinterventions, but this difference was not statistically significant. This is supported by the fact that there was no disparity in the rate of aneurysm related death during long-term follow-up between the two age groups.

