











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
To diagnose aortic root and ascending aorta (AA) dilatation in clinical practice, it is essential to have clearly defined normal values of aortic diameters. However, it is still unclear which the normal range is, as the most appropriate methodology to define them is a matter of open debate. Normal values first established by Roman et al. were based on data derived from 135 adult subjects1. Most subsequent studies aimed at defining normal values of the aorta have limitations such as small sample size, non-standardized echocardiographic measurements, heterogeneous inclusion criteria, or lack of inclusion of non-Caucasian or overweight populations2-4. Aortic dimensions are influenced by age and body size1,2. Much of the data underlying current indexing recommendations are based on studies in patients whose body mass index (BMI) was < 30 kg/m2 which may not reflect accurately a large percentage of the population1-4. Moreover, indications for prophylactic surgical intervention of thoracic aortic (TA) aneurysms (TAAs) in international guidelines are still based on absolute aortic diameter5,6. This approach ignores the patient's body size, which is a significant determinant of aortic dimensions.
In an attempt to adjust for body size, the use of Z-scores or aortic diameters indexed by body surface area (BSA) haves been proposed. However, Z-score calculations are complex and are unclear whether they are universal to different populations. In addition, the BSA is subject to variability in individual subjects because of changes in body weight and this should be considered due to the high prevalence of overweight and obesity worldwide (almost 60% in countries across Latin America)7. Considering that height shows relative stability in adulthood, it has been proposed the use of the aortic height index (AHI)8,9. Furthermore, because height is a simple, reliably obtained, non-derived variable that relates linearly to cardiac dimensions independent of age and weight, we aimed to investigate the impact of overweight and obesity on different proposed methods of aortic dimensions indexation.
The MATEAR study (in Spanish: Medición de Aorta Toracica por Ecocardiografia en Argentina; Aortic Thoracic Dimensions Measurement by Echocardiography in Argentina) was a national prospective registry of echocardiographic aortic dimensions in apparently healthy subjects, aimed at defining upper normal limits (UNLs) of thoracic aorta in the Argentinian population10. An important initial finding of this study was that in patients with increased BMI, BSA lost predictive value of aortic dimensions in the Valsalva sinuses, while height was not affected by BMI (adjusted R2 of the model with BSA in total patients: 0.07 vs. adjusted R2 of the model with BSA in patients with BMI < 25 kg/m2: 0.27)10. As a result, the "BSA-indexed normal values" for the overall population lead to an underestimation of aortic dilatation in obese subjects.
Therefore, we aim to further investigate the impact of overweight and obesity on different proposed methods of aortic dimensions indexation and to determine the best definition of dilatation for the population with BMI ≥ 25 kg/m2. Specifically, the objective of this analysis is to compare the indexation of aortic dimensions by AHI and BSA in a subpopulation of the MATEAR registry with and without overweight adjusting for other significant covariates such as age and gender. Our hypothesis is that indexing aortic dimensions to patient's height would be more appropriate than indexing to BSA for determining UNL of aortic diameters in population with BMI ≥ 25 kg/m2.
Methods
Population
The MATEAR study was a prospective, observational, and multicenter study involving 53 accredited echocardiography laboratories of the Argentine Society of Cardiology (SAC). Between February 2018 and June 2019, 1000 consecutive healthy adult individuals were enrolled. Individuals with hypertension, a history of major cardiovascular risk factors, TAA, any degree of aortic stenosis or regurgitation, previous cardiac surgery, pregnancy, family history of genetic aortopathies and/or bicuspid aortic valve, competitive sport participants, and smokers were excluded (Table S1 for complete exclusion criteria).
Assessment of covariates of interest
Relevant related clinical variables were collected for each patient, including demographic and anthropometric data, blood pressure, and cardiovascular history (personal and of first-degree family members). Overweight was defined as subjects with a BMI ≥ 25 kg/m2. BSA was calculated by the Dubois formula11.
Assessment of aortic diameters
Each patient underwent a comprehensive transthoracic echocardiogram (TTE) to rule out unknown cardiovascular diseases, following standard protocols based on ASE/EACVI Guidelines12. TA diameters were measured at the aortic annulus, sinuses of Valsalva, sinotubular junction (STJ), and proximal tubular AA (at 1 cm above STJ)2. Annulus was measured at mid-systole (inner to inner edge method) and the other aortic diameters at end diastole (leading to leading edge) (Fig. S1)12. We included subjects with complete aortic measurements (from annulus to proximal tubular AA). Operators were trained through an explanatory video to unify image acquisitions following the ASE/EACVI recommendations. The definitions of race and ethnicity were adapted from previous local studies representative of the ethnic composition of Argentine population (native Americans, European, and middle eastern)13,14.
Echocardiographic images were recorded in native DICOM format and coded after anonymization for analysis. Aortic measurements were performed onsite and confirmed offline by two experienced readers. The measurements obtained offline were included in the analysis. Interobserver variability of the aortic diameters was tested by two blinded observers in 100 subjects. In these subjects, two replicate measurements of aortic diameters were taken by each observer. All measurements were performed at a single examination. The readers were kept unaware of each other's results. To assess interobserver agreement, the onsite and offline means measurements' value of each observer was plotted and analyzed with correlation test.
Study sample
The population was randomized and stratified by age and sex to obtain a balance sample. We included all overweight subjects from MATEAR (n = 528: 294 males and 234 females) and 351 subjects with BMI < 25. The final population for the analysis was 879 and it was split into four groups according to gender and BMI (men with BMI < 25, men with BMI ≥ 25, women with BMI < 25, and women with BMI ≥ 25).
Ethical considerations
The registry was approved by the bioethics committee of the Argentinian Society of Cardiology (SAC). The study protocol obtained approval from every local ethic committee and an informed consent was obtained from each participant. The study was carried out following the recommendations for medical research suggested by the Declaration of Helsinki, the Good Clinical Practice Guides, and current ethical regulations.
Statistical analysis
Normality of distribution of continuous variables was assessed with the Kolmogorov-Smirnov test. The values included in the 2.5th-97.5th percentile were considered as reference values and the upper reference values as the UNL. Discrete variables were expressed as proportions. Continuous variables with normal distribution were expressed as mean and standard deviation, while those with non-normal distribution were expressed as median and interquartile range. Student's t-test was used to compare continuous variables with parametric distribution and Mann-Whitney U-test for those with non-parametric distribution. A correlation analysis was performed between aortic diameters at each level and anthropometric variables such as age, BSA, height, and BMI using either Pearson or Spearman test, as appropriate. Interobserver and intraobserver correlation was evaluated with intraclass correlation coefficient (ICC). The analysis was repeated stratifying the population according to gender and BMI category. Univariable linear regression analysis was applied to test the association between demographic and anthropometric variables and aortic dimensions. Stepwise forward multivariable linear regression was performed, including in the analysis all the variables with p ≤ 0.1 in univariable analysis. Control for collinearity was warranted in the multiple linear regression analysis. R software was used for statistical analysis considering a two-tailed p < 0.05 as significant.
Results
Demographic data
The present analysis included 879 healthy adult individuals (mean age: 39.7 ± 11.4 years, 399 men). Most individuals were of European or Amerindian ethnicity (55.9% and 39.6%, respectively). Baseline characteristics are presented in table 1. Age, height, and weight distributions are shown in supplementary figures S2-S4. Absolute aortic diameters were significantly higher in men. Similarly, men showed significantly greater anthropometric dimensions, left ventricular dimensions, and wall thickness values. Moreover, men had higher systolic, diastolic, and mean blood pressure values, although they were within the normal range. The observed differences between genders are shown in table 2. A larger proportion of men than women was in the overweight category (294 [73%] and 234 [48.7%], respectively, p < 0.0001).
Table 1 Characteristics of the population according to BMI
| Variables | Total (n = 879) | BMI < 25 (n = 351) | BMI ≥ 25 (n = 528) | p-value |
|---|---|---|---|---|
| Age (years) | 39.7 ± 11.4 | 39.1 ± 11.5 | 40.1 ± 11.3 | 0.15 |
| Male, n (%) | 399 (45.3%) | 105 (29.9%) | 294 (55.6%) | 0.0001 |
| Height (cm) | 167 ± 9 | 166 ± 8 | 168 ± 9 | < 0.0001 |
| Weight (kg) | 75.2 ± 16.3 | 61.5 ± 8.9 | 84.4 ± 13.4 | < 0.0001 |
| BSA (m2) | 1.8 ± 0.2 | 1.7 ± 0.2 | 1.9 ± 0.2 | < 0.0001 |
| BMI | 26.6 ± 4.9 | 22.2 ± 1.8 | 29.6 ± 4.1 | < 0.0001 |
| European, n (%) | 491 (55.9%) | 230 (65.5%) | 261 (49.4%) | < 0.0001 |
| Amerindian, n (%) | 348 (39.6%) | 99 (28.4%) | 247 (46.7%) | 0.0001 |
| Middle eastern, n (%) | 35 (3.9%) | 19 (5.4%) | 16 (3.0%) | 0.08 |
| Other, n (%) | 5 (0.6%) | 3 (0.8%) | 2 (0.3%) | 0.39 |
| Echocardiographic parameters | ||||
| LVEF (%) | 64.8 ± 4.8 | 64.7 ± 4.9 | 64.9 ± 4.8 | 0.2 |
| LVMi (g/m2) | 70.9 ± 13.5 | 68.3 ± 13.9 | 72.7 ± 12.9 | < 0.0001 |
| RWT | 0.36 ± 0.06 | 0.35 ± 0.06 | 0.37 ± 0.04 | 0.0001 |
| LA volume index (ml/m2) | 23.7 ± 6.8 | 24.5 ± 6.8 | 23.2 ± 6.9 | 0.004 |
| E/A | 1.47 ± 0.4 | 1.47 ± 0.4 | 1.47 ± 0.5 | 0.5 |
| Aortic annulus (cm) | 2.03 ± 0.21 | 1.95 ± 0.20 | 2.08 ± 0.20 | < 0.0001 |
| Valsalva sinus (cm) | 2.94 ± 0.40 | 2.90 ± 0.38 | 2.96 ± 0.42 | 0.02 |
| Sinotubular junction (cm) | 2.59 ± 0.37 | 2.54 ± 0.35 | 2.63 ± 0.38 | 0.0004 |
| Proximal ascending aorta (cm) | 2.77 ± 0.37 | 2.70 ± 0.33 | 2.81 ± 0.37 | < 0.0001 |
BMI: body mass index; BSA: body surface area; E/A: E and A wave of mitral inflow; LA: left atrium; LVEF: left ventricular ejection fraction; LVM: left ventricle mass indexed by BSA; RWT: relative wall thickness. Results are expressed as mean ± SD.
Table 2 Anthropometric and echocardiographic characteristics according to gender
| Variables | Women (n = 480) | Men (n = 399) | p value |
|---|---|---|---|
| Age (years) | 40.7 ± 11.5 | 38.5 ± 11.1 | 0.003 |
| Weight (kg) | 68.1 ± 14.6 | 83.8 ± 13.9 | < 0.0001 |
| Height (cm) | 161.9 ± 6.0 | 174.6 ± 7.6 | < 0.0001 |
| BSA - Dubois (m2) | 1.74 ± 0.19 | 2.01 ± 0.19 | < 0.0001 |
| BMI (kg/m2) | 26.0 ± 5.5 | 27.5 ± 4.1 | < 0.0001 |
| SBP (mmHg) | 110.5 ± 9.0 | 114.3 ± 7.6 | < 0.0001 |
| DBP (mmHg) | 70.1 ± 8.1 | 73.6 ± 7.2 | < 0.0001 |
| MBP (mmHg) | 83.6 ± 7.6 | 88.9 ± 7.2 | < 0.0001 |
| LVEF % | 65.1 ± 4.8 | 64.0 ± 5.2 | 0.0003 |
| LAVi (ml/m2) | 23.8 ± 6.4 | 23.8 ± 7.2 | 0.77 |
| LV mass (g/m2) | 67.3 ± 12.7 | 75.3 ± 13.1 | < 0.0001 |
| RWT | 0.36 ± 0.06 | 0.36 ± 0.06 | 0.65 |
| E/A | 1.47 ± 0.48 | 1.45 ± 0.5 | 0.5 |
| LV EDD (cm) | 4.4 ± 0.4 | 4.7 ± 0.4 | < 0.0001 |
| LV ESD (cm) | 2.7 ± 046 | 2.9 ± 0.4 | < 0.0001 |
BSA: body surface area; BMI: body mass index; DBP: diastolic blood pressure; EDD: end-diastolic diameter; ESD: end-systolic diameter; LAV: left atrial volume indexed by body surface area; LV: left ventricle; LVEDV: left ventricular end-diastolic volume; LVEF: left ventricular ejection fraction; LVESV: left ventricular end-systolic volume; MBP: mean blood pressure; RWT: relative wall thickness; SBP: systolic blood pressure. Results are expressed as mean ± SD.
Reliability of measures
The reproducibility of aortic dimension measurements was very good, with an ICC of 0.77-0.95 for intraobserver and 0.68-0.92 for interobserver variability.
Aortic dimensions
In the analysis of groups according to BMI and gender (Figs. 1 and 2), indexing of aortic diameters at the sinus, STJ and ascending aortic levels by BSA showed significantly lower values in obese and overweight subjects compared to normal weight in their respective gender. For women, sinus diameter indexed to BSA was 1.75 cm/m2 in BMI < 25 versus 1.52 cm/m2 in BMI between 25 and 29.9 versus 1.41 cm/m2 in BMI ≥ 30; at the STJ: 1.53 cm/m2 versus 1.37 cm/m2 versus 1.25 cm/m2; and at the AA: 1.63 cm/m2 versus 1.50 cm/m2 versus 1.37 cm/m2. Overweight and obese men also showed significantly lower values of aortic diameters indexed to BSA: sinus diameter indexed to height was 1.69 cm/m2 in BMI < 25 versus 1.55 cm/m2 in BMI between 25 and 29.9 versus 1.43 cm/m2 in BMI ≥ 30; at the STJ: 1.49 cm/m2 versus 1.36 cm/m2 versus 1.28 cm/m2; and at the AA: 1.57 cm/m2 versus 1.43 cm/m2 versus 1.36 cm/m2. However, these differences disappeared when indexing by height (AHI) in both gender groups (all p = NS; right panels in Figs. 1 and 2).
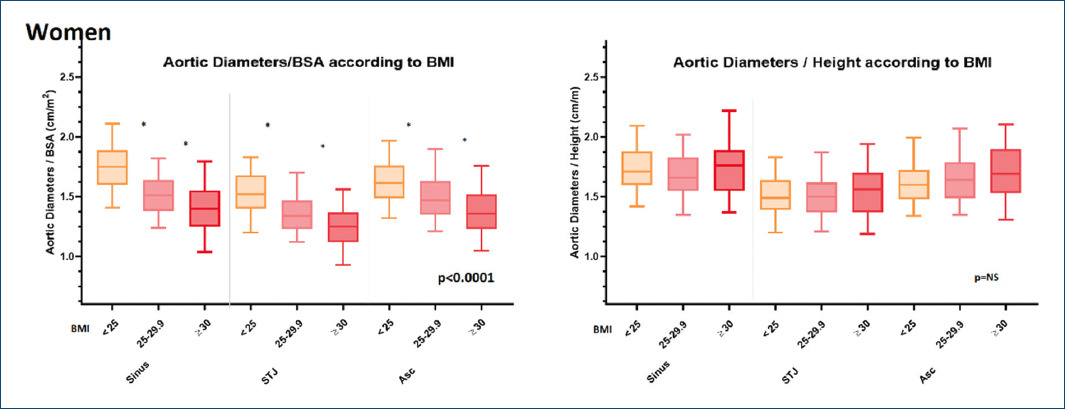
Figure 1 Analysis in women (n = 480). Comparison of mean (P2.5-97.5) aortic diameters at sinus, sinotubular junction, and proximal ascending aorta indexed by BSA or hHeight according to BMI (under 25, 25-29.9, and ≥ 30). Asc: ascending aorta. BMI: body mass index. BSA: body surface area. STJ: sinotubular junction. *Denotes p < 0.05.
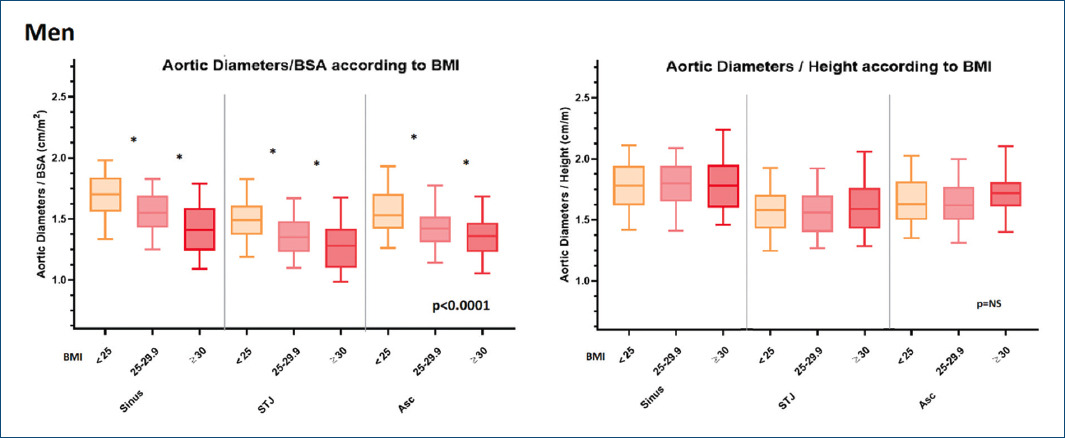
Figure 2 Analysis in men (n = 399). Comparison of mean (P2.5-97.5) aortic diameters at sinus, sinotubular junction, and proximal ascending aorta indexed by BSA or height according to BMI (under 25, 25-29.9, and ≥ 30). Asc: ascending aorta. BMI: body mass index. BSA: body surface area. STJ: sinotubular junction. *Denotes p < 0.05.
Demographic and echocardiogram variables were also compared by gender and BMI category, as shown in supplementary table 2. There were no differences in age, height, LVEF, and E/A relation between obese and overweight subjects compared to normal weight in their respective gender. As expected, weight, BSA, and BMI were greater in obese and overweight subjects compared to normal weight in their respective gender. Women with BMI < 25 showed significantly greater LAVi, while obese and overweight women showed greater LV Mass and RWT.
The AHI UNL (percentile 97.5) of 2.20 cm/m for sinuses of Valsalva, 1.99 cm/m for the STJ, and 2.09 cm/m for the proximal AA allowed to discriminate aortic dilation in the overweight population (Table 3).
Table 3 Aortic height index normal ranges according to BMI and gender
| Thoracic aortic dimensions | Total (n = 879) | Women | Men | ||
|---|---|---|---|---|---|
| BMI < 25 | BMI ≥ 25 | BMI < 25 | BMI ≥ 25 | ||
| LNL-UNL | LNL-UNL | LNL-UNL | LNL-UNL | LNL-UNL | |
| Sinus (cm/m) | 1.35-2.20 | 1.35-2.15 | 1.33-2.22 | 1.38-2.12 | 1.40-2.22 |
| STJ (cm/m) | 1.19-1.99 | 1.16-1.85 | 1.19-1.94 | 1.21-1.97 | 1.24-2.05 |
| Ascending aorta (cm/m) | 1.29-2.09 | 1.27-2.08 | 1.30-2.13 | 1.31-2.08 | 1.29-2.09 |
Lower (LLN) and upper limits of normal (ULN) (Percentiles 2.5-97.5) are bolded. P reflects comparison of ULN between BMI < 25 (normal weight), and BMI ≥ 25 (overweight) BMI: body mass index; BSA: body surface area; LLN: lower normal limit; STJ: sinotubular junction.
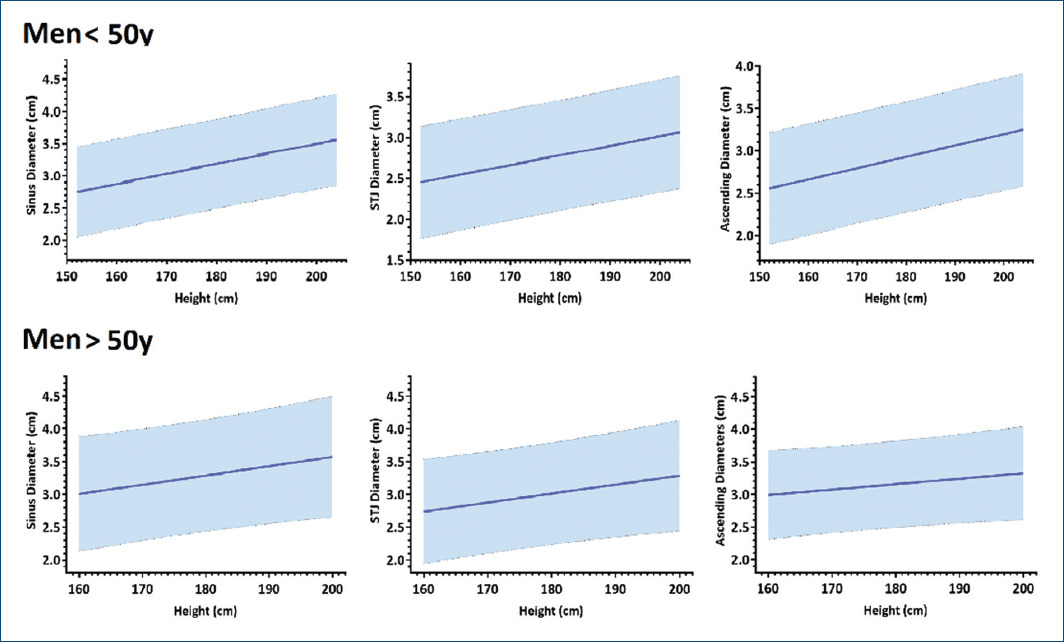
Dedicated nomograms according to height for each gender and age groups (≤ or older than 50 years) are presented to show the implicancies over aortic dimensions generated by age, gender, and body size. They convey in a graphical form a better understanding of aortic dimensions according to gender and age. About 95% normal confidence limits for aortic diameters at the sinuses of Valsalva in relation to height in women younger and older than 50 years are presented in figure 3 and in men in figure 4.
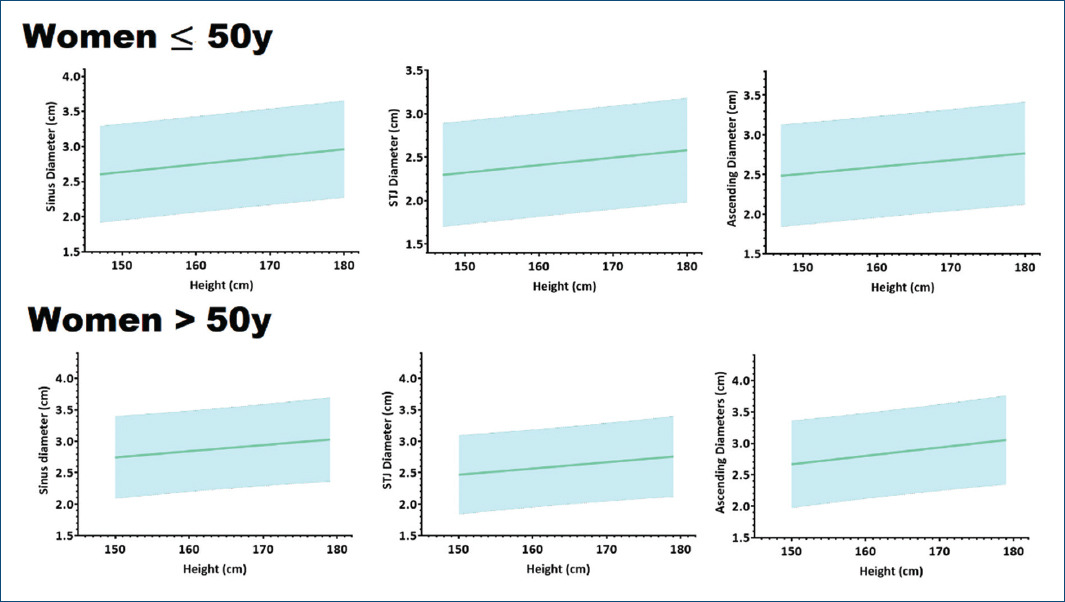
Figure 3 Nomograms of diameters at sinus of Valsalva, sinotubular junction, and proximal ascending aorta according to different heights for women ≤ and older than 50 years. X-axis represents height in centimeters; Y-axis represents aortic diameter in centimeters; STJ: sinotubular junction; y: years.
Correlation analysis
Both sinus and ascending measurements correlated significantly with gender, age, height, and BSA in the univariable analysis.
A correlation analysis was performed between aortic diameters at each level and anthropometric variables such as age, BSA, height, and BMI. After linear regression analysis, height was an independent predictor of aortic diameters at sinus, STJ, and AA even after adjusting for age, gender, and ethnicity (p < 0.05), as shown in tables S3 and S4.
Discussion
In this study, we compared the indexation of aortic dimensions by height and BSA in a subpopulation of the MATEAR registry with and without overweight, adjusting for other significant covariates such as age and gender. We demonstrate that aortic dimensions must be indexed to body size but, as opposed to dimensions indexed by BSA, indexation to height is similar for individuals with normal weight and overweight, suggesting that AHI could be used in populations regardless of their weight.
Dilation of the aortic sinuses and AA has important diagnostic, management, and prognostic consequences in numerous cardiovascular diseases, such as Marfan syndrome and bicuspid aortic valves. Aortic size remains an important criterion for surgical intervention and an accurate predictor of the natural risks of TAA15-18. Aortic dimensions increase progressively and regularly with age at a rate of nearly 1 mm per decade19.
Most studies aiming to define the normal aortic values present limitations such as marked heterogeneity of inclusion criteria, relatively small sample, absence of methodological standardization in echocardiographic measurements, and lack of inclusion of non-Caucasian populations1-4,20-22. Furthermore, most of the studies excluded overweight subjects, representing a serious limitation considering the substantial increase in prevalence of obesity in our modern society.
There is great controversy to define the normal values of the thoracic aorta in both genders, and the best proposed approach is to normalize diameters by body size. As changes in weight modify the BSA but not necessarily the size of aortic structures, the indexation could be more robust if height instead of BSA was used8. Zafar et al. proposed that a patient's weight might not contribute substantially to aortic size and growth9. Moreover, weight fluctuates throughout the lifespan and can be greatly modified by dietary or medical interventions. Nidorf et al. showed a strong linear correlation between each cardiac dimension and body height, suggesting that during development, cardiac dimensions increase primarily in response to skeletal growth8. In effect, Saura et al. showed in multiple linear regression analysis that the model which included height as the independent variable showed a higher regression coefficient than the model with BSA2. Furthermore, indexing aortic dimensions to patient height has been shown to be useful in subjects with bicuspid aortic valve, as well23,24.
Despite the fact that the prevalence and severity of obesity have dramatically increased in the world, we are still indexed with BSA which might be underestimates aortic dilatation in a considerable proportion of patients. Our study was a national, prospective, and multicentric registry that excluded individuals with pathologies that might influence aortic dilatation. The population included in the study is representative of the Argentine and most Latin American populations in terms of age, BSA, height, and weight25. To the best of our knowledge, only two studies assessed the impact of obesity on aortic dimensions. Campens et al. included 81 obese subjects in a cohort of 849 Caucasian subjects21. They showed that obesity had no significant impact on proximal thoracic aortic dimensions when added to multivariate models. However, the fact that only 10% of the subjects were obese, especially in the age group > 70 years, was a limitation of the study. On the other hand, Lam et al. assessed the impact of the increase of BMI on aortic root dimensions and showed that a 5 kg/m2 increase in BMI was associated with a larger predicted aortic root diameter in men (0.78 mm) than in women (0.51 mm), adjusting for age and blood pressure26. In our cohort, we previously showed that in subjects with increased BMI, BSA lost predictive value of aortic dimensions in the Valsalva sinuses, while height was not affected by BMI10. One of the important conclusions of our study was that in overweight subjects (BMI ≥ 25 kg/m2) would be more appropriate to index by height than by BSA to avoid underestimating aortic dilatation and that AHI are similar in individuals at different BMI groups.
It should be taken into account that even though age was comparable between genders when stratifying by BMI, there were differences in LAVi, LV mass, and RWT between obese and overweight versus normal weight women. Analogous with aorta measurements deficits, there is a paucity of data examining how best to index LAV in obese individuals. Davis et al. recently confirmed that using height-based indexing methods to determine LA dilation allowed better prediction of mortality in severely obese populations. They suggest using non-BSA-based indexing techniques in all overweight populations27. Further research is needed to consider indexing of other echocardiographic parameters in overweight and obese populations.
Even though Marfan patients are frequently tall and thin, certain individuals with MFS are clinically obese, that means many uncertainties when we consider indexed aortic dimensions. We excluded genetic aortopathies from our population and height was representative of the Argentine population in terms of age, BSA, height, and weight25. As a consequence, we should not extrapolate this result to patients with Marfan syndrome.
In contrast to the mean trends noted, certain individuals with MFS were clinically obese. This can be of special concern in patients with compromised cardiac function. Individuals with MFS are not constitutionally freed from susceptibilities to excessive weight gain. To explain the atypical habitus of these normal body mass or obese individuals with MFS, it is possible that some mutations in FBN1 have a specifically reduced effect on muscle and fat.
Finally, it is important to take into account that diameters are not the only way to predict risk of aortic complications. In most studies that analyze the normal values of the aorta adjusting for age, sex, and body size, only a quarter of the variance is explained, with coefficients of determination between 0.25 and 0.3016. Therefore, there are biological factors influencing the size of the aorta and not explained only by demographic or anthropometric variables.
In daily practice, echocardiographers evaluate overweight subjects and it remains controversial how to define aortic dilatation in this group. In overweight and obese subjects weight increases without a proportional increase in height. Consequently, changes in weight increase the BSA. As the average weight of the world's population increases, correct definition of aortic dilatation in overweight patients becomes an even more important topic. As changes in weight modify the BSA, indexing aortic diameters by BSA may fail to identify patients at increased risk of acute aortic syndromes. Thus, our results implies the necessity of a change in the cardiologist mindset and encourage them to consider using height indexation instead of BSA-based index to determine aortic dilation in overweight and obese subjects.
Limitations
The present study has some limitations. First, the cross-sectional design of our study did not allow us to predict the influence on aortic diameters of time-dependent changes in parameters, such as body size parameters and blood pressure. Second, the group of individuals older than 65 years was under-represented, as is the case in most cohort studies of healthy individuals, which may limit the applicability of the reference values to elder populations. Third, the results may not extrapolate to patients with any of the exclusion criteria, such as Marfan syndrome and genetic aortopathies with different growth patterns, leading to higher height and impact on BMI. Finally, the applicability of our results should be reproduced in populations of various regions and races around the world and in patients with aortic pathologies.
Conclusions
Using height-based indexing method to determine aortic dilation is not affected by weight in both genders.
As changes in weight modify the BSA, indexing aortic diameters by BSA may fail to identify patients at increased risk of acute aortic syndromes. Therefore, AHI could be used in populations regardless of their weight. Reference normal values for AHI at aortic root, STJ, and proximal AA are provided.
Supplementary data
Supplementary data are available at Archivos de Cardiología de México (DOI: 10.24875/ACM.22000017). These data are provided by the corresponding author and published online for the benefit of the reader. The contents of supplementary data are the sole responsibility of the authors.

