











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Cardiovascular diseases (CVD) are the primary cause of death and disability in adults around the world1. The most frequent form of CVD is atherosclerotic CVD (ASCVD), which is a manifestation of multiple toxic cardiometabolic (CM) risk factors: elevated blood pressure, dysglycemia, dyslipidemia, overweight, obesity, and tobacco usage (smoking, chewing, and vaping). These risk factors induce progressive arterial wall injury by numerous maladaptive responses (endothelial dysfunction, inflammation, prothrombotic, and pro-oxidant state), that begins decades before the occurrence of the first clinical event. Comprehensive CM risk control strategies should optimally treat all CM risk factors.
Based on the foregoing, the ALALIP (Latin American Academy of Lipidology and CM Prevention), together with IASC, IAS, and PCE, convened a group of experts from the Americas, based on their clinical expertise in: cardiology, cardiovascular prevention, and CM diseases, to develop practical recommendations for the optimal evaluation and treatment of CM risk factors in Latin America. The process was well defined to avoid conflicts of interest that could bias the discussion and recommendations.
We use a modified Delphi methodology aims to generate a comprehensive CM risk reduction guideline, using personalized medicine and patient-centered decision considering the cost-benefit ratio, based on three premises2,3:
1) Global vision derived from a multidisciplinary expert discussion to incorporate the best scientific evidence.
2) Developing criteria to identify relevant clinical issues.
3) Define practical pathways to improve daily clinical care.
In suppl. table 1, we made a detailed description of the document preparation process, the guidelines used for the construction of recommendations and the qualification of evidence.
Residual risk (RR) represents the risk which persists despite reaching the proposed treatment goals for the classic CM risk factors according to the current guidelines4. RR applies in primary and secondary prevention scenarios and rises as the individual baseline global risk rises5. The concept emerged from the statin trials. Low-density lipoprotein cholesterol (LDL-C) levels are the primary target in patients with dyslipidemia6. However, despite reaching LDL-C levels as low as < 70 mg/dl, RR often persists, particularly in higher risk individuals. Originally, RR aimed at identifying and treating atherogenic dyslipidemia (AD): elevated triglyceride (TG), low high-density lipoprotein cholesterol (HDL-C) levels, and a higher proportion of small and dense LDL-C (LDL pattern B)7,8. However, the RR concept should extend beyond AD and apply to all other uncontrolled ASCVD risk factors.
The recommendations by this consensus panel are summarized in figure 1 and table 1. RR reduction should consider therapeutic options adapted to specific patient needs, based on five treatment objectives: TG-rich lipoproteins (TgRL), inflammation, impaired glucose metabolism, high blood pressure (HBP), and prothrombotic status. This approach acknowledges various pathophysiological pathways and identifies therapies to consider, with no hierarchical classification, to accomplish an optimal RR reduction, aimed at delivering precise, and personalized medicine9. The pharmacotherapy assessed includes: statins, ezetimibe (EZT)10, proprotein convertase subtilisin/kexin 9 inhibitors (PCSK9i)11,12, eicosapentaenoic acid (EPA)13, canakinumab14, colchicine15-18, metformin, sodium-glucose cotransporter 2 inhibitors (SGLT2i)19,20, glucagon-like peptide-1 (GLP-1) receptor agonists19,20, dual antiplatelet therapy21,22, and rivaroxaban23.
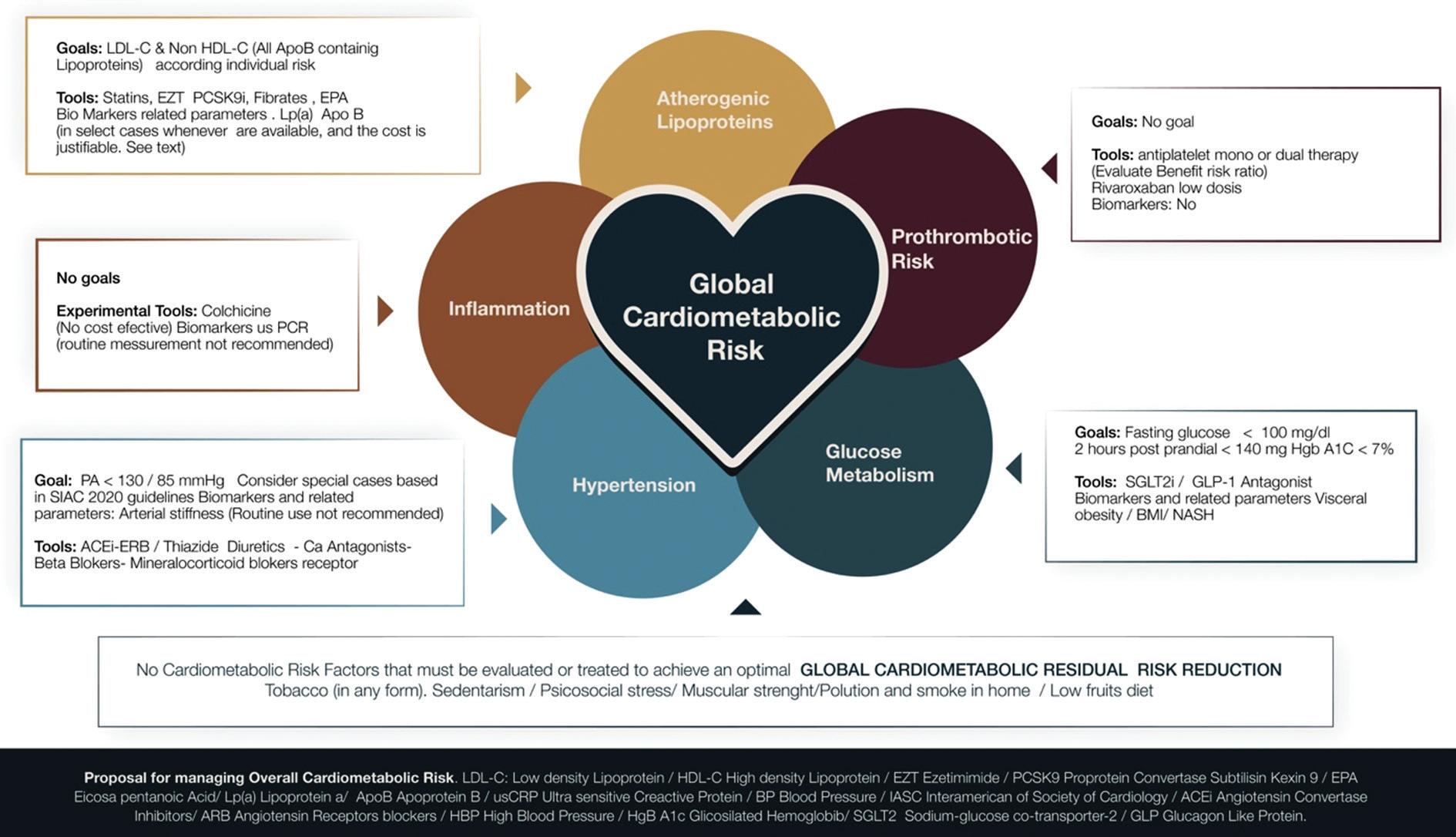
Table 1 Summary of recommendations with level of evidence
| RECOMMENDATIONS | Class | Level | Ref | |
|---|---|---|---|---|
| CMR assessment and management | ||||
| Comprehensive assessment of CMR, including the objectives and their corresponding therapies, benefit-risk ratio, and cost-effectiveness must be discussed with the patient and his/her relatives | I | A | ||
| Optimum treatment should be implemented to achieve the optimal CMR reduction | I | A | ||
| LDL-C goals according to risk category | ||||
| Low risk: LDL-C < 115 mg/dL/Non-HDL-C < 145 mg/dL | I | A | 5-9 | |
| High risk: LDL-C < 70 mg/dL (or at least 50% reduction)/Non-HDL-C < 100 mg/dL | ||||
| Very high risk: LDL-C < 55 mg/dL (or at least 50% reduction)/Non-HDL-C < 85 mg/dL | ||||
| Atherogenic Dyslipidemia: Non-HDL-C (second therapeutic objective after achieving the primary goal: LDL-C based on risk category) | I | A | 4,5,7,8,13,36,37 | |
| In patients that, despite receiving statins at adequate doses and being at the right goal according to their risk profile, experience a recurrent atherosclerotic cardiovascular event, their LDL-C goal may be < 40 mg/dl. | IIb | C | 11-13 | |
| Diagnostic strategies | ||||
| - Routine calculation of Non-HDL-C (surrogate for ApoB): | I | B | 32 52,53 | |
| - Lp(a) measurement to assess risk. Indications: | ||||
| - Premature or progressive ASCVD with maximum lipid-lowering therapy | ||||
| - Familial hypercholesterolemia | ||||
| - Premature or progressive ASCVD with maximum lipid-lowering therapy | ||||
| - Premature ASCVD in family members | ||||
| - Direct relatives with elevated Lp(a) | 52,53 | |||
| - Failure to achieve expected LDL-C reduction with statin therapy | ||||
| - Whenever the means are available and the cost is justifiable, Lp(a) should be measured | IIa | B | ||
| - Measuring Lp(a) in patients not included in the above-mentioned cases is not recommended | III | C | ||
| HDL-C goals or pharmacological therapy not recommended | III | A | 32-34,36 | |
| Therapeutic strategies | ||||
| Risk/Clinical Condition/Goal | ||||
| Non-pharmacological: - Nutrition, exercise, weight loss and smoking cessation | For every patient, regardless of the risk | I | A | 17,21,37,64,69-73 |
| As a strategy to help elevate HDL-C | IIa | C | 17,21,37,64,69-73 | |
| Monotherapy with statins | Initial therapy to the lower LDL-C and achieve the goal based on the risk. Select the molecule and dose according to the percentage reduction required to achieve the goal. Use the maximum tolerable dose with no time limit. | I | A | 26-30 |
| Monotherapy with Ezetimibe | Only in case of proven statin intolerance and requiring less than 20% LDL-C reduction | IIb | C | |
| Statins with Fenofibrate | Primary prevention | IIa | B | 40,41 |
| Secondary prevention | IIb | C | ||
| Statins and gemfibrozil | Contraindicated | III | A | 5,37 |
| Statins and ezetimibe | Initial therapy: If reduction required in LDL-C is > 55% | IIa | C | |
| Second line after potent statins at maximum dose and failure to achieve the LDL-C goal | IIa | B | 10 | |
| Statins and PCSK9i | Second line after potent statins at maximum dose and failure to achieve the LDL-C goal. | IIa | A | 11,12,27,30,33,34 |
| Assess and inform the patient about cost-benefit ratio and make decision together with the patient. | ||||
| Therapeutic strategies in case of high or very high risk after maximum tolerable doses of potent statins | ||||
| Increase the statin dose or switch to a more potent statin | IIa | B | 25,26,30 | |
| Add ezetimibe | IIa | B | 10,48 | |
| Add PCSK9i, if available and there is an acceptable cost-benefit ratio. Inform and decide together with the patient. | IIa | A | 11,12,29,30,33,34,37,48 | |
| PCSK9i triple therapy (Statins + Ezetimibe + PCSK9i) High risk and failure to achieve the goal with dual therapy. The potential of familial hypercholesterolemia must be assessed. | IIa | C | 48 | |
| EPA (4 g/d) for patients with established ASCVD or high risk diabetic patients already on a statin and with TG > 135 mg/dl. | IIa | B | 13,48 | |
| Maintain lipid lowering treatment for an indefinite period of time, at the dose and with the initial regimen, in order to achieve optimum goals based on individual risk estimation, unless unequivocal side effects develop | I | C | 49-51 | |
| Fenofibrate 160 mg/d/High-risk diabetics with at least one RF TG ≥ 200 mg/dl and HDL-C ≤ 40 mg/dl and LDL-C on target based on risk under statin therapy | IIb | C | 40,41 | |
| Diabetic patients - glucose lowering medications as an option to reduce cardiometabolic risk | ||||
| CV risk reduction should be a primordial goal in patients with T2DM, in addition to achieving a proper HbA1c reduction | I | A | 54-56 | |
| It is necessary to discuss the cost-benefit ratio of these novel drugs with the patients before prescribing them | I | A | 54-67 | |
| SGLT2i (empagliflozin, canagliflozin, and dapagliflozin) may be prescribed as a first line drug for the purpose of controlling glycemia and reducing CV risk in patients with CVD, HF, CKD, or high to very high CM risk | I | B | 58-67 | |
| SGLT2i could be a second line option after stable doses of metformin | IIa | B | 58-67 | |
| In patients with HF and CKD, with or without T2DM, the use of SGLT2I must be considered | I | A | 62-64 | |
| GLP-1 (Liraglutide, semaglutide, and dulaglutide) Prior to the use of insulin or together with basal insulin to prevent insulin intensification. As first line therapy in overweight/obese patients with no insulin indication. | IIa | B | 20,65-67 | |
| GLP-1 (Liraglutide, semaglutide, and dulaglutide) Clinical evidence of ACSVD or high to very high cardiometabolic risk, after metformin | IIa | B | 20,65-67 | |
| Hypertension | ||||
| The use of a fixed-dose combination is recommended in moderate and high-risk patients as a strategy to improve adherence | I | A | 68 | |
| Inflammation | ||||
| Despite being an important component in pathophysiology and residual risk, there is no recommendation to measure or treat pro-inflammatory risk. | III | C | 14,15,69 | |
| Colchicine could be a useful anti-inflammatory strategy when started early in a post MI scenario and in patients with evidence of stable coronary disease, after treatment with statins, aspirin and ACEI/ARB | IIb | B | 15-18 | |
| Hs-CRP as a routine approach to lower RCR is not recommended | III | C | ||
| Prothrombotic risk | ||||
| Aspirin (prior bleeding assessment) in high to very high-risk patients | IIa | A | 21 | |
| Aspirin stable CAD and non-cardioembolic ischemic stroke or TIA | I | A | 22,23,71 | |
| Following ACS or after a percutaneous arterial intervention, patients should receive dual antiplatelet therapy for as long as necessary, depending on the setting and clinical judgment | I | A | 70 | |
| For ACS, rivaroxaban 2.5 mg BID may be considered, after discontinuation of parenteral anticoagulation, in addition to aspirin and clopidogrel, for 1 year, in the absence of previous TIA or stroke, and with low risk of bleeding | IIb | B | 72 | |
| Patients with atherosclerosis in ≥ 2 vascular beds or two additional risk factors (current smoking, diabetes, renal insufficiency, HF, or non-lacunar ischemic stroke ≥ 1 month), rivaroxaban 2.5 mg BID may be considered | IIb | B | 72 | |
| Clopidogrel/severe PAD of the lower extremities | IIa | B | 71,72 | |
| Rivaroxaban 2.5 mg BID + aspirin 100 mg OD Severe PAD of the lower extremities (low risk of bleeding) | IIa | B | 72 | |
| Recently vascularized PAD (low risk of bleeding) | I | B | 72 | |
| With all antithrombotic and anticoagulant strategies, bleeding is an important risk; therefore, the net clinical benefit must to be carefully considered in every patient before prescribing them. | I | A | 19-21,72 | |
| Behavioral and Lifestyle-associated Cardiometabolic Risk factors | ||||
| Obesity, lack of physical activity, inadequate diet, alcohol abuse, and smoking are all risk factors to consider and assess and to intervene in patients with CMR and in the assessment of RCR | I | A | 24,73-77 | |
| Compliance assessment as an overall risk component must be evaluated in every patient | IIa | B | 73 | |
| In patients with low or non-adherence, implement strategies that have proven to be helpful, such as using fixed-dose combinations, and polypill based on availability in each country could be an effective choice | IIa | B | 73-77 | |
| General considerations | ||||
| Social determinants for CVD or social risk in Latin America must be assessed, since these are basically related to the level of education, income, environmental pollution, models of and access to healthcare services | IIa | A | 24,39,68 | |
| We strongly recommend the formation of global cardiometabolic risk units to accomplish these goals. This strategy will reduce cardiovascular morbidity-mortality, establishing global cardiometabolic risk protocols that will enable the development of healthy habits, as well as an articulated treatment of all risk factors. | IIa | A | 24,39,68 | |
CM risk: cardiometabolic risk; RF: risk factor; RCR: residual cardiometabolic risk; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; Non HDL-C: non-high density lipoprotein cholesterol; Lp(a): lipoprotein a; ASCVD: atherosclerotic cardiovascular disease; PCSK9i: proprotein convertase subtilisin/kexin type 9 inhibitors; EPA: eicosapentaenoic acid; TG: triglyceride; SGLT2i: sodium/glucose cotransporter 2 inhibitors; GLP-1: glucagon-like peptide 1; ACEI: angiotensin convertase enzyme inhibitors; ARB: angiotensin receptor blocker; Hs-CRP: high sensitivity C-reactive protein; CAD: coronary artery disease; TIA: transient ischemic attack; ACS: acute coronary syndrome; HF: heart failure; PAD: peripheral arterial disease.
CM risk enhancing factors should be assessed routinely, including smoking, physical inactivity, psychosocial stress, inadequate diet, muscle strength, and environmental pollution, which contribute to the risk of CV disease and CV death, in particular, in middle- and low-income countries24. CM risk goes beyond the traditional risk factors and, hence, ASCVD prevention involves the proactive evaluation of all of these risk factors.
Based on the above discussion, this consensus recommends a comprehensive assessment of CM risk (IA). Once the risk factors are identified, treatment should be implemented to achieve the optimal CM risk reduction (IA). The heightened risk persists as long as all of the factors are not systematically screened and treated. All treatment options must be discussed with the patient and, where appropriate, with his/her family (IA).
Dyslipidemia
The final goal of lipid-related CM risk is to decrease concentrations of all circulating pro-atherogenic ApoB containing lipoproteins (IC)25. Achieving the LDL-C risk-stratified target is the primary goal in treating patients with dyslipidemia. Evidence with statin and non-statin therapies, including gastroileal bypass, in different populations with different baseline LDL-C levels and varying risks, has shown a robust association between the reduction of LDL-C and the decline in CM risk26-30.
This consensus recommends reducing LDL-C as the primary objective for RRR (IA).
However, it has been observed that, in patients treated with statins, there is a persistent RR secondary to several causes, including:
1) Use of inadequate, low doses of statins.
2) Failure to achieve an optimal LDL-C target.
3) Persistently elevated TgRL concentrations despite adequate LDL-C goal with statin therapy31.
Lp(a) definitely could be considered a fourth lipid cause of persistent RR, see below in paragraph 1.4 for specific recommendations and management.
Suppl. Table 2 summarizes the results of recent trials that tested different types of drugs as adjuvant therapies with statins in patients with high and very-high CVR. The LDL-C values achieved in the trials with EZT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT), PCSK9i Further Cardiovascular Outcomes Research with PCSK9i in Subjects with Elevated Risk (FOURIER), and Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment With Alirocumab (ODYSSEY), are the lowest reported in the history of clinical trials10,11,12. LDL-C values as low as ≤ 10 mg/dl were achieved, accompanied by a significant and safe incremental CVR reduction over and above that observed with statin therapy. These findings suggested that "lower is better, but lowest is best"11-13,32.
There is no known LDL-C threshold below which there is physiological hazard; in fact, many genetic polymorphisms that give rise to the lower LDL-C are protective against the development of atherosclerosis. Meta-analyses show that there is no increased risk for either ischemic or hemorrhagic stroke with the achievement of very low LDL-C. Moreover, the EBBINGHAUS (Evaluating PCSK9i Binding Antibody Influence on Cognitive Health in High Cardiovascular Risk Subjects) trial demonstrated no heightened risk for cognitive impairment even when attaining ultra-low LDL-C of < 10 mg/dL32,33.
In these trials, the ARR was small, which may be due to the fact that most patients were being treated with high statin doses, and their baseline LDL-C was relatively low, as compared to the previous statin monotherapy trials. However, ARR significantly improves as the risk of patients increases34.
Therefore, to be cost-effective, it is indispensable to select patients based on their risk and use these therapies in those patients most likely to benefit from them. The patient and, when appropriate, the family, should be included in the decision-making process.
Based on our analysis, to achieve an optimal RRR level, the members of this consensus recommend the following targets for LDL-C (IA):
- Low risk: LDL-C < 115 mg/dl/Non-HDL-C < 145 mg/dl
- Moderate risk: LDL-C < 100 mg/dl/Non-HDL-C < 130 mg/dl
- High risk: LDL-C < 70 mg/dl (or at least 50% reduction)/Non-HDL-C < 100 mg/dl
- Very high risk: LDL-C < 55 mg/dl (or at least 50% reduction)/Non-HDL-C < 85 mg/dl
In patients failing to attain these values, a RR associated with insufficiently reduced LDL-C levels will persist. In patients that, despite receiving statins at adequate doses and being at the right goal according to their risk profile, experience a recurrent atherosclerotic cardiovascular event, their LDL-C goal is < 40 mg/dl. (IIbC)
1.1. TgRL, Remnants, and HDL - Recently published evidence, which includes prospective longitudinal cohorts, Mendelian randomization studies, and randomized clinical trials, shows that TgRL are a component of residual CM risk. Therefore, this panel considers that non-HDL-C, that represent every apoB atherogenic particles including cholesterol remnants, must be assessing. LDL-C overlooks the atherogenic potential of remaining apoB particles; even lipoprotein (a) also carrying apoB is included in the LDL cholesterol measurement. Indeed, cholesterol remnants as all the TgRL, cause ASCVD just like LDL35. This may be especially important in individuals treated with statins, in obese patients, and in patients with DM or Pre DM in whom cholesterol content in C- LDL is lower than other remnants apoB-containing particles and more cholesterol is transported in TgRL. In those situations, apoB and also non-HDL cholesterol identifies patients with an increased number of cholesterol-containing TG-rich apoB-containing particles, these patients continue to be at high risk of ASCVD events even with C-LDL in target.
That's why we, consider that Non HDL-C should be considered as a secondary goal, once the LDL-C target has been reached36-40 (IA), and lowering the non-HDL-C to risk-stratified levels as a second therapeutic objective (IA), since it represents all of the Apo-B-carrying proatherogenic lipoproteins39,40.
Apo-B and remnants measurement is expensive and not widely available all Latin American countries. Non-HDL-C determination is simple, cost-effective, and has an excellent correlation with TgRL levels, ApoB containing particles and remnants; hence, it can be used as a surrogate marker for Apo B36. This consensus recommends a routine calculation of non-HDL-C in all patients (IB) as an Apo B surrogate. In the locations where the measurements of ApoB are possible and it is affordable for the patient, it could be measure after a cost benefit discussion with the patients (IIb).
Epidemiological studies have shown an inverse relationship between low levels of HDL-C and CVR, but it should not be treated since the CCTs that have tested pharmacological strategies to raise levels of HDL-C to the lower the risk CV events have failed to demonstrate any efficacy41,42. This consensus statement does not recommend pharmacological therapy for low HDL-C and agrees that there should not be any HDL-C goals at the present time (IIIA).
1.2. Adjuvant pharmacological therapies to statins to treat TgRL Achieving the therapeutic goals of all circulating pro-atherogenic ApoB containing lipoproteins25,36 is necessary to achieve optimal CM risk reduction. In many subjects, particularly in those at high and very-high risk, the goals are not achieved with statin monotherapy and, hence, adjuvant therapies should be used. Combination therapy is a common strategy in other conditions such as HBP and T2DM and results in higher rates of therapeutic goal attainment.
A critical analysis based on the levels of evidence available for the various therapeutic classes was conducted, regarding their ability to reduce RR when combined with statins. This consensus panel focused on omega-3 fatty acids (O3FA) and fibrates as adjunctive therapy to treat residual CM risk related to high Tg levels.
FIBRATES: According to available evidence from secondary endpoint analyses, fenofibrate is the only molecule with enough evidence of reducing CM risk and may be indicated for both primary (IIaB) and secondary prevention (IIbC)43,44. The combination of statins with gemfibrozil is contraindicated (IIIC) since gemfibrozil inhibits their glucuronidation and can lead to myopathy and rhabdomyolysis. Ciprofibrate should not be used due to lack of evidence (IIIC).
O3FA: eicosapentaenoic acid and docosahexaenoic acid (EPA/DHA) have the ability to reduce TG and have been tested in several CCTs with divergent or inconclusive results45-47. The REDUCE-IT trial, with a highly purified EPA ethyl ester, demonstrated a significant MACE reduction and reduced CV mortality in patients at high and very high risk, treated with statins, with LDL-C at target but Tg > 150 mg/dl13.
Simplified drug combination algorithm to accomplish therapeutic goals (Fig. 2), the class of drugs with the most conclusive and robust evidence are the statins; consequently, they are indicated as first line agents, using the maximum tolerated dose (IA) (Suppl. Table 3).
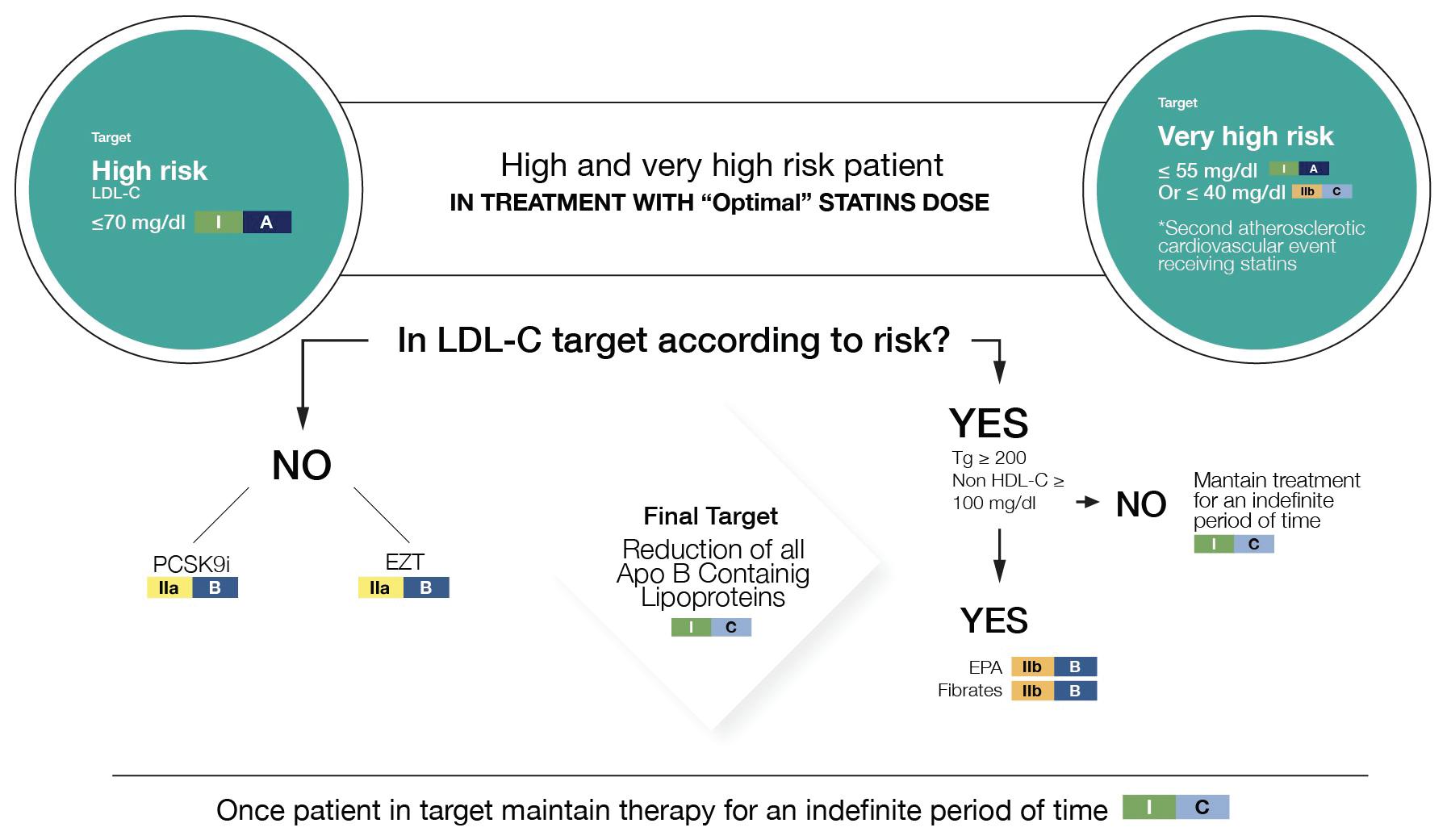
Only in the event of a proven statin intolerance and requiring < 20% LDL-C reduction can we recommend monotherapy with EZT (IIbC).
The drugs recommended for use in combination with statins are: EZT and PCSK9i48 (IIaA).
In patients with an LDL-C > 55% above the goal, EZT could be in the initial combination (IIbC), or as a second-line adjuvant therapy following high dose potent statins and failing to accomplish the LDL-C goal (IIaB).
In high- or very high-risk patients failing to accomplish the goals after treatment with statin, the following may be recommended:
- Increase doses or switch to a more potent statin (IIaB)
- Add EZT(IIaB)
- Add PCSK9i, if available and cost-effective (IIaA)
- In patients achieving the LDL-C goal, but with a fasting Tg > 150 mg/dl, (after lifestyle changes for 6 weeks), EPA dose of 4 g/d could be prescribed (IIaB)
- In patients who persist with Tg > 200 mg/dl, fenofibrate could be prescribed at a dose of 160 mg (IIbC)
- Among high risk patients (with established ASCVD or diabetic with multiple risk factors) with TG > 150 mg/dl, icosapent ethyl can be prescribed at a dose of 2.0 g twice daily (IIa).
1.3. Lipid-lowering treatment duration atherosclerotic disease is a systemic immune inflammatory process that is progressive secondary to exposure of the arterial wall to various risk factors with damage accruing over time.
The 20 year follow-up of "West of Scotland Coronary Prevention Study" showed a 24% reduction in myocardial infarction (MI), 18% in coronary events, and a 35% decrease in HF-related hospital admissions. No reduction was observed in non-CV deaths or stroke49. Prospective studies on the impact of discontinuing statins have reported a 33% increase in CVE and a risk of hospital admissions with 42% increase in stroke, after 1 year of treatment discontinuation50,51.
When combining outcomes data with cost-effectiveness data, we conclude that the use of statins for long-term treatment is efficacious and justified.
This consensus panel recommends the prescription of statins for an indefinite time, at the dose necessary to achieve optimal LDL-C goals based on individual risk (IC), unless unequivocal side effects develop such as myalgia or myopathy, although these are relatively infrequent.
1.4. Lipoprotein (a) Lp(a) a unique apo(a) and an apoB-containing lipoprotein particle is one of the most important genetically determined risk factors for CVD. Mendelian randomization studies provide strong support for causality for Lp(a) as a causal risk factor for ASCVD, aortic stenosis, and heart failure. Roughly 25% of the general white population have Lp(a) > 30 mg/dL, level associated with high risk. In Latin America it is important to realize that it is demonstrated pronounced differences between ethnic groups (is highest in black people), and differences may depend of standardization of assays, characteristics of population and sample52,53.
Based on the evidence available, the consensus agreed that Lp(a) is a cause of residual CM risk Many epidemiologic studies confirm that elevated serum levels of Lp(a) herald risk for ASCVD (IB).
The object of measuring Lp(a) is not to provide treatment, but its assessment to reclassify patients to a higher risk group. Consequently, this consensus panel recommends that whenever the means are available and the cost is justifiable, Lp(a) should be measured (IIaB).
Clinical conditions in which Lp(a) measurement is recommended (IB):
- Early onset or progressive ASCVD with maximum lipid lowering therapy
- Familial hypercholesterolemia
- Early onset of ACVD in family members
- Direct relatives with elevated Lp(a).
Measuring Lp(a) in patients not included in the above-mentioned cases is not recommended. (IIIC)
2. GLOBAL CM RISK REDUCTION The "Prospective Urban Rural Epidemiology" (PURE) trial24 showed that over 70% of CVD may be attributed to a small number of CM risk factors: HBP, TgRL, diabetes, pre-diabetes, and abdominal obesity. Hence, this consensus emphasizes the necessity for a comprehensive control of all of these factors for an optimal CM risk reduction.
3. GLUCOSE METABOLISM Individuals with T2DM or prediabetes have a higher CM risk; their primary cause of death is CVD54. T2DM medical therapy includes glycemic control to avoid acute metabolic complications and long-term strategies to reduce the risk of micro- and macro-vascular events.
There is a continued need for the development of new antidiabetic drugs and to assess their impact on CM risk and CV safety in adequately designed CCT. Historically, clinical trials taught us that the intensive reduction in HbA1c (< 7%) has a significant impact on microvascular complications, but not on macrovascular events55,56. However, the development of newer antiglycemic agents has now provided physicians with the therapeutic means to reduce glycemic indices and reduce risk for macrovascular events, such as MI, ischemic stroke, and CV mortality.
Based on the above discussion, this consensus recommends that CV risk reduction should be a primordial goal in patients with T2DM, in addition to achieving a proper HbA1c reduction (IA).
3.1. SGLT2 inhibitors Sodium-glucose cotransporter 2 inhibitors (SGLT2i): dapagliflozin, empagliflozin, and canagliflozin, induce glucosuria by inhibiting the uptake of glucose along the proximal tubule, reduce serum glucose levels, promote diuresis and sodium elimination, lower BP, and serum uric acid and are associated with weight loss. Other effects include lowering intraglomerular pressure and proteinuria, preventing tubulo-interstitial and glomerular injury, inhibiting the sodium-proton exchanger, and increasing hematocrit, serum beta-hydroxybutyrate, and angiotensin 1-757. These medications have a low risk for hypoglycemia.
These drugs have been tested in several clinical trials (Suppl. Table 4) and have demonstrated consistent cardio-renal-vascular protection, regardless of the diagnosis or not of T2DM58-67.
Based on the results of these clinical trials, this consensus panel recommends:
1) In patients with T2DM and established CVD, HF, CKD or high to very high CM risk, SGLT2i may be prescribed as a first-line drug for the purpose of controlling glycaemia and reducing CV risk (IB).
2) SGLT2i may be used as a second line option after metformin. (IIaB)
3) In patients with HF and/or CKD, with or without T2DM, the use of SGLT2I should be considered (IA).
4) Regard chronic kidney disease emerging evidence derived from RCTs and meta-analyses demonstrate a cardio-protective and nephro-protective effects of SGLT2i. We recommend their use in patients with baseline eGFR up to 30 mL/min/1.73 m2.
3.2. GLP-1 receptor agonists Glucagon-like peptide-1 receptor agonists are the only injectable non-insulin therapy for controlling T2DM, with high glucose-lowering power (with low risk of hypoglycemia), and significant weight loss20.
Liraglutide, semaglutide, and dulaglutide have been proven to reduce the risk of MACE (Suppl. Table), whereas lixisenatide and extended-release exenatide have a neutral effect65-67.
This consensus recommends GLP-1 receptor agonists (liraglutide, semaglutide, and dulaglutide) as a treatment option in patients with evidence of ASCVD who are at high risk after metformin, or before the use of insulin, or together with basal insulin to prevent insulin intensification; this could be a parenteral first line therapy in overweight patients with no insulin indication (IIaB). Availability of and accessibility to these medications should be considered and it is necessary to discuss the cost-benefit ratio with the patients before prescribing (IA).
Hypertension
HBP is the risk factor with the highest attributable risk; BP control is critical in reducing CM risk. A detailed discussion about the BP goals and treatment regimens is beyond the scope of this paper (refer to the IASC Statement)68.
Pharmacological therapy should start at BP ≥ 140/90 mm Hg; the recommended goals should be < 130/85 mm Hg. The recommended drug classes are: ACE inhibitors/angiotensin receptor blockers, thiazide diuretics, calcium antagonists, and beta-blockers. Mineralocorticoid receptor blockers may be prescribed in difficult to manage cases or refractory HBP. The use of fixed dose combination therapy is recommended in moderate- and high-risk patients as a strategy to improve BP control and long-term adherence (IA).
Inflammation
Plays a pivotal role in atherogenesis, acute plaque rupture, and ASCVD-related events9. Therefore, inflammation is a significant factor to consider as a cause of RR.
Three pharmacological strategies have been tested in trying to show that, by selectively and independently reducing vascular inflammation, a decline in RR is achieved.
a) Canakinumab: The CANTOS trial reported a significant benefit; it is a drug with an extremely high cost and hence it is not recommended for the treatment of patients with an elevated RCR (IIIC)14. It is also not approved for this indication.
b) Colchicine: An affordable anti-inflammatory drug has been tested targeting inflammation to reduce CV risk15-18. Colchicine Cardiovascular Outcomes Trial (COLCOT) demonstrated a beneficial impact of low-dose colchicine (0.5 g/d) in the post-MI setting. A recent analysis shows that early initiation of colchicine within the first 3 days after MI is associated with a greater reduction of the primary endpoint15.
In LODOCO 2 (a trial which used low doses of colchicine), the primary end point was reduced significantly17. Low-dose therapy was not associated with any serious adverse effects.
Results of the Colchicine in Patients with Acute Coronary Syndrome (COPS) trial showed that colchicine does not improve CV outcomes in patients with ACS. The differences with the previous results could be in part due to the size of the cohort studied18.
5.3. Methotrexate: The Cardiovascular Inflammation Reduction Trial (CIRT) observed that, at low doses, it failed to reduce the risk of CV events69.
The major implications of these findings are that it may be possible to reduce the risk of CV events in patients with stable coronary disease by targeting inflammation. This consensus recommends that:
a) Colchicine could be a useful anti-inflammatory strategy if started early in a post MI scenario and in patients with evidence of stable coronary disease, after treatment with statins, aspirin, and ACEI/ARB (IIbB).
b) This consensus does not recommend assessing inflammation hs-CRP as a routine approach to the lower RCR (IIIA).
Prothrombotic status
Effective and safe anti-thrombotic therapy using antiplatelet21,22 and anticoagulation drugs70-72 is essential to reducing RCR. This consensus recommends the use of an antithrombotic therapy, depending on the drug type and patient's clinical scenario:
a) In patients with high or very-high cardiovascular risk, assess the risk of bleeding and consider aspirin therapy (IIaA).
b) All patients with stable coronary disease and non-cardioembolic ischemic stroke or TIA should receive aspirin (75-81 mg) (IA).
c) Following ACS or after a percutaneous arterial intervention, patients should receive dual antiplatelet therapy for as long as necessary, depending on the setting and clinical judgment (IA)21,22.
d) For ACS, rivaroxaban 2.5 mg BID may be considered, in addition to aspirin and clopidogrel, for 1 year, in patients with an elevated risk of ischemia, in the absence of the previous TIA or stroke, and with low risk of bleeding (IIbB)23,72.
e) In patients with severe lower extremity PAD, clopidogrel may be considered (IIaB).
f) In patients with severe PAD of the lower extremities and with low risk of bleeding, the combination of rivaroxaban 2.5 mg BID plus aspirin 100 mg/day could be considered (IIaB)71.
g) In patients with recently vascularized PAD and low risk of bleeding, the combination of rivaroxaban 2.5 mg BID plus aspirin 100 mg/day is recommended (IB)70.
Behavioral And Lifestyle-Associated CM Risk Factors
Obesity, physical inactivity, inadequate diet, alcohol abuse, and smoking are enhancing risk factors to consider for evaluation in patients with CM risk and in the assessment of RCR (IA)24,73-77.
Poor compliance and lack of long-term adherence are behavioral attitudes that are additional risk factor in patients with CM risk. Depression and anxiety could increase the lack of adherence to drugs and lifestyle modifications. Therefore, it is mandatory to inquire about poor adherence as an overall risk component, usually associated with the number of pills prescribed. This consensus recommends the implementation of strategies to improve compliance and hence reduce risk, such as using fixed-dose combinations in patients prescribed individual components, based on availability in each country (IA).
Table 2 summarizes the recommendations for these risk factors in all patients.
Table 2 Recommendations for managing lifestyle changes
| Risk factor | Goal | Type of therapy |
|---|---|---|
| Obesity | BMI < 25 | Indicate: |
| WAIST-HIP RATIO | · Lifestyle changes | |
| Males: < 0.90 | · Diet 800-1500 Kcal/day | |
| Females: < 0.84 | · Exercise 200-300 min/week | |
| · Metabolic surgery in patients with a BMI > 35 and two comorbidities or a BMI > 40 | ||
| Potential recommendation: | ||
| · Orlistat | ||
| Smoking | Smoking cessation | Recommended: |
| · Psychotherapy | ||
| · Chewing gum | ||
| · Drug therapy | ||
| · Bupropion, Varenicline | ||
| Tobacco in any form not allowed (Vaping, inhaling chewing, etc.) | ||
| HBP | <140/90 | Indicated: |
| · Lifestyle changes | ||
| · Salt intake 7.5-12 g/day | ||
| · Physical activity 200-300 min/week with 40% strength | ||
| Recommended | ||
| Dysglycemia | Hba1c < 5.7 | · Fiber-rich diet and reduced intake of refined carbohydrates |
| DM | Hba1c < 7 | · Physical activity at least 150 min/week with 40% strength |
To minimize the incidence of CVD in the population, as well as to reduce RCR, physicians must be aware of the importance of risk factors and lifestyles, so that they may routinely and systematically explain them to the patient, their family, including children and adolescents, at each visit.
What has been described as the social determinants for CVD or social risk in Latin America must be assessed, since these are basically related to the level of education, income, and access to health-care services (IA). Finally, this consensus wants to underscore the need to evaluate and treat CM risk in a comprehensive and integrated way to achieve an optimal control of all risks. In this respect, we strongly recommend that global CM risk units be formed to accomplish this goal. This strategy will reduce cardiovascular morbidity-mortality; establishing global CM risk prevention protocols that will enable the development of healthy habits, as well as an articulated treatment of all risk factors (IA).

