Artículos de investigación
Idioventricular rhythm and shock after a honeybee
sting
Ritmo idioventricular y shock después de un piquete de
abeja
Desireé Franco-Lugo1
*
Denise A. Uribe-Vallarta1
Karen D. Bernal-Contreras1
Valerie P. Vargas-Abonce2
Enrique Soto-Pérez-De-Celis3
Jaime Rivera-Figueroa4
Daniel Cuevas-Ramos5
Francisco J. Gómez-Pérez5
Miguel Á. Gómez-Sámano5
1Universidad Anáhuac México Norte, Ciudad de
México, México
2Universidad Autónoma Metropolitana Unidad
Xochimilco, Ciudad de México, México
3Department of Geriatrics, Instituto Nacional de
Ciencias Médicas y Nutrición Salvador Zubirán, Ciudad de México,
México
4Department of Cardiology and Electrophysiology,
Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Ciudad de
México, México
5Department of Endocrinology, Instituto Nacional
de Ciencias Médicas y Nutrición Salvador Zubirán, Ciudad de México,
México
Abstract
Objective:
The objective of this study was to describe the case of a 19-year-old male
presenting with bradycardia and hypotension after a honeybee sting making a
review of the literature and pathophysiology of the cardiovascular and
electrocardiogram (EKG) changes after a bee sting.
Methods:
The patient’s airway was inspected and secured. Electrocardiogram with an
idioventricular rhythm at 41’ bpm. Oxygen was administered, an intravenous
access was established, and the transcutaneous pacemaker leads were placed
on the chest of the patient, then published guidelines management was
induced.
Results:
The EKG showed idioventricular rhythm at a rate of 41 beats/min that resolved
to a normal sinus rhythm after treatment.
Conclusions:
A full and prompt cardiovascular evaluation should be performed in all
patients presenting to the emergency department after a bee sting, and
published guidelines regarding the management of bradycardia and anaphylaxis
should be followed to achieve successful outcomes.
Key words Honeybee sting; Idioventricular rhythm; Bradycardia
Resumen
Objetivo:
Describir el caso de un paciente masculino de 19 años que presenta
bradicardia e hipotensión después de una picadura de abeja haciendo una
revisión de la literatura y fisiopatología de los cambios cardiovasculares y
electrocardiográficos después de una picadura de abeja.
Métodos:
Se inspeccionó y aseguró la vía aérea del paciente. Un rastreo de ECG
realizado al ingreso reveló ritmo idioventricular a una ritmo de 41 latidos
por minuto. Se administró oxígeno, se estableció un acceso IV y se colocaron
los cables del marcapasos transcutáneo en el tórax del paciente, luego se
indujo el manejo de las guías publicadas.
Resultados:
El electrocardiograma mostró un ritmo idioventricular a una frecuencia de 41
latidos por minuto que se resolvió a un ritmo sinusal normal después del
tratamiento.
Conclusiones:
Se debe realizar una evaluación cardiovascular completa y rápida en todos los
pacientes que se presentan al departamento de emergencias después de una
picadura de abeja, y se deben seguir las pautas publicadas sobre el manejo
de la bradicardia y la anafilaxia para lograr resultados exitosos.
Palabras clave Picadura de abeja; Ritmo idioventricular; Bradicardia
Introduction
We describe the case of a 19-year-old male patient who presented with an
idioventricular rhythm after a honeybee sting. The literature review has shown that
the venom content of Apis mellifera can cause from local
non-allergic to anaphylactic shock reactions.
Case presentation
A previously healthy 19-year-old man was admitted to our emergency department with
generalized paresthesias, dyspnea, facial edema, and a rash in his neck and both
upper extremities. On arrival, the patient was conscious and able to move his
extremities.
Patient history before admission
Our patient had been stung by a honeybee in the neck 30 min before admission; he
reported a previous anaphylactic shock following a bee sting 7 years earlier. On
admission, his blood pressure was 60/40 mmHg, his pulse was regular at a rate of 40
beats/min, and his temperature was 37°C and pulse oximetry in 92%.
Hospital management
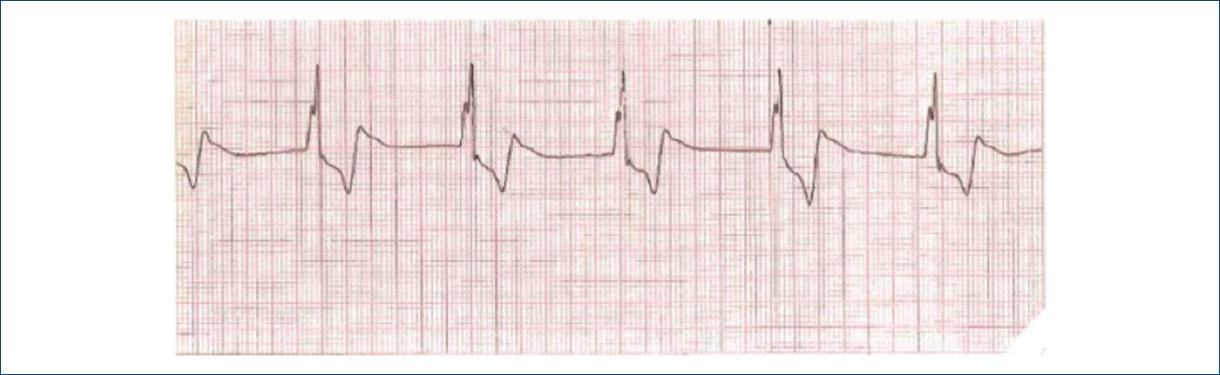
The patient’s airway was inspected and secured. An electrocardiogram (EKG) tracing
taken on admission revealed idioventricular rhythm at a rate of 41 beats/min (Fig. 1). Oxygen was administered, an intravenous
(IV) access was established, and the transcutaneous pacemaker leads were placed on
the chest of the patient; then, atropine was administered at a dose of 0.5 mg IV,
producing a change in the EKG tracing, which showed P waves and a heart rate of 65
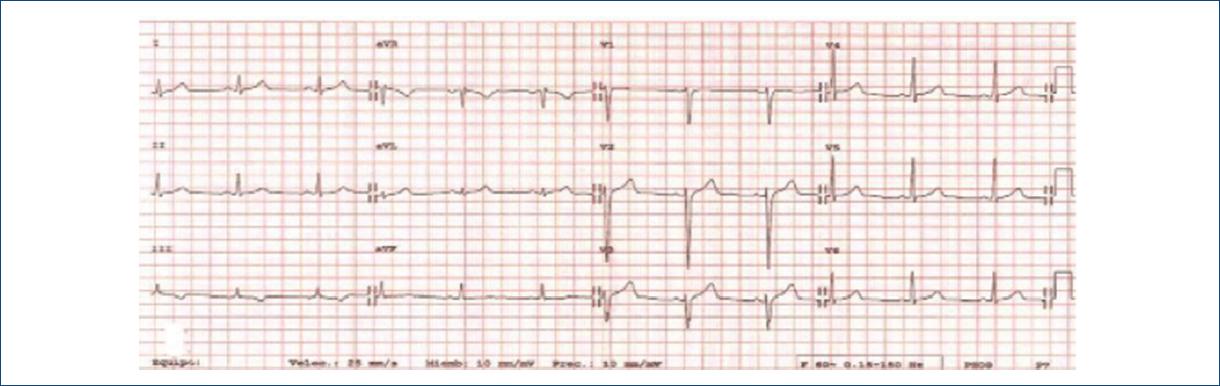
beats/min. Two liters of normal saline, hydrocortisone, ranitidine, and
chlorpheniramine were also administered intravenously. After these, the 12 lead EKG
showed normal sinus rhythm at a rate of 65 beats/min (Fig. 2) and blood pressure rose to 120/70 mmHg. Blood test results were
all within the normal range. The patient remained under observation for 24 h, after
which he was uneventfully discharged home.
Discussion
Honeybee (Apis mellifera) venom can cause a variety of reactions
ranging from local non-allergic reactions (pain and erythematous lesions) to
anaphylactic (laryngeal edema, bronchospasm, and hypotension)1 or in some rare cases toxic reactions (myocardial infarction,
acute renal injury, and encephalopathy)2, the
local effects are due to the toxic component of the venom, while the most severe
reactions are related to an allergic systemic response3. In the United States, hornets, bees, and wasps are the cause of 70%
of all venomous animal-related fatalities, causing an average of 48 deaths/year4. In Mexico between 1998 and 2009, there were
480 deaths associated with bee stings5.
Cardiovascular events after bee stings have mostly been described in relation to
anaphylactic shock, although several reports have underlined the relevance of the
direct action of the venom on the heart and the coronary circulation, even causing
myocardial infarction6-9.
Honeybee venom is composed of a mix of peptides, amines, and enzymes that include
apamin (a small neurotoxin that blocks Ca2+ dependent K+
channels)10, adrenaline, noradrenaline,
histamine, serotonin, and tertiapine, which may provoke myocardial ischemia and
intense hypotension11. It could also be the
cause of an allergic or non-allergic local reaction, anaphylaxis, or a systemic
toxic reaction such as vomiting or edema12.
Animal studies have proven that on the injection of bee venom, an intense bradycardic
response is elicited which, at least in part, contributes to the fall in blood
pressure that characterizes anaphylaxis. This response is probably related to the
direct effect of toxins on the pacemaker of the heart and is transitory and fully
reversible13. In small concentrations,
bee venom caused a decrease in the heart rate of an isolated toad heart and
elongation of the PR interval, with marked electrocardiographic changes that
included depression of the ST segment, atrioventricular conduction disturbances, and
atrial arrhythmia14.
Bee stings usually cause temporary electrocardiographic changes, given the local
vasoactive, cardiotoxic, or anaphylactic effects contained in their venom6.
The clinical manifestations of bee stings can be local or generalized. Local
reactions mainly include pain, swelling, and pruritus at the site of the sting and
are self limiting15. Generalized reactions,
including anaphylactic shock and cardiovascular effects, usually present within the
first 30 min after the sting and can cause urticaria, rash, breathlessness,
wheezing, airway edema, weakness, anxiety, and confusion16.
Treatment
Recommendations for the treatment go from the inspection of the site to remove any
residue as they can form a portal for entry of germs and bacteria, cold ice, or
compresses which should be administered to control the local reaction, as well as
the administration of oxygen and fluids intravenously to avoid shock and
hypotension17. The antihistaminics and
epinephrine should be administered; in case, the patient has a known allergy. Some
patients have required permanent pacemaker after a bee sting18. In the case of our patient, atropine was administered
initially to treat the rhythm abnormalities observed in the EKG tracing, with
successful results. Continuous observation for 24 h revealed no further EKG
abnormalities and the rest of the manifestations caused by the bee sting resolved
after the administration of histamine receptor blockers. It is important to know
that bee stings can present with idioventricular rhythm.
Conclusions
Although bee stings are seldom lethal, they represent the first cause of death from
venomous animal exposure in the United States. A full and prompt cardiovascular
evaluation should be performed in all patients presenting to the emergency
department after a bee sting, and published guidelines regarding the management of
bradycardia and anaphylaxis should be followed to achieve successful outcomes.
Acknowledgments
MAGS would like to acknowledge Luz del Carmen Abascal Olascoaga for her support.
References
1. Ciszowski K, Mietka-Ciszowska A. Hymenoptera stings. Prz Lek.
2007;64:282-9.
[ Links ]
2. Mingomataj EÇ, Bakiri AH, Ibranji A, Sturm GJ. Unusual reactions
to hymenoptera stings:what should we keep in mind?Clin Rev Allergy Immunol.
2014;47:91-9.
[ Links ]
3. Brown TC. Reactions to honeybee stings:an allergic prospective.
Curr Opin Allergy Clin Immunol. 2013;13:365-71.
[ Links ]
4. Langley RL. Animal-related fatalities in the United States-an
update. Wilderness Environ Med. 2005;16:67-74.
[ Links ]
5. Becerril-Ángeles M, Núñez-Velázquez M, Arias-Martìnez MI, Grupo
del Programa de Control de la Abeja Africanizada, SAGARPA. Mortality related to
honey-bee stings in Mexico from 1988 to 2009. Rev Alerg Mex.
2013;60:58-62.
[ Links ]
6. Puvanalingam A, Karpagam P, Sundar C, Venkatesan S, Ragunanthanan
S. Myocardial infarction following bee sting. J Assoc Physicians India.
2014;62:738-40.
[ Links ]
7. Scherbak D, Lazkani M, Sparacino N, Loli A. Kounis syndrome:a
stinging case of ST-elevation myocardial infarction. Heart Lung Circ.
2015;24:e48-50.
[ Links ]
8. Puttegowda B, Chikkabasavaiah N, Basavappa R, Khateeb ST. Acute
myocardial infarction following honeybee sting. BMJ Case Rep.
2014;2014:3.
[ Links ]
9. Murat SN, Karasu BB, Akdemir R, Kilic H, Ornek E, Ozcan O. Acute
coronary syndrome triggered by honeybee sting:a case report. Emerg Med J.
2009;26:754-5.
[ Links ]
10. Lazdunski M. Apamin, a neurotoxin specific for one class of
Ca2+-dependent K+channels. Cell Calcium. 1983;4:421-8.
[ Links ]
11. Knulst AC, de Maat-Bleeker F, Bruijnzeel-Koomen CA. Wasp and bee
venom allergy. Ned Tijdschr Geneeskd. 1998;142:889-92.
[ Links ]
12. Nisahan B, Selvaratnam G, Kumanan T. Myocardial injury following
multiple bee stings. Trop Doct. 2014;44:233-4.
[ Links ]
13. Guimarães JV, Costa RS, Machado BH, dos Reis MA. Cardiovascular
profile after intravenous injection of Africanized bee venom in awake rats. Rev
Inst Med Trop Sao Paulo. 2004;46:55-8.
[ Links ]
14. Nabil ZI, Hussein AA, Zalat SM, Rakha MK. Mechanism of action of
honey bee (Apis mellifera L.) venom on different types of
muscles. Hum Exp Toxicol. 1998;17:185-90.
[ Links ]
15. Przybilla B, Ruëff F. Hymenoptera venom allergy. J Dtsch
Dermatol Ges. 2010;8:114-27.
[ Links ]
16. Valentine MD. Allergy to stinging insects. Ann Allergy.
1993;70:427-32.
[ Links ]
17. Ridolo E, Martignago I, Passalacqua G, Mauro M, Incorvaia C.
Evaluation of the safety of a protocol for switching venom immunotherapy
products. Ann Allergy Asthma Immunol. 2018;120:429-30.
[ Links ]
18. Gupta PN, Kumar BK, Velappan P, Sudheer MD. Possible
complication of bee stings and a review of the cardiac effects of bee stings.
BMJ Case Rep. 2016;2016:bcr2015213974.
[ Links ]
Copyright: © 2021 Instituto Nacional de Cardiología Ignacio
Chávez.












 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink