











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Coronary angiography is the gold standard technique for the diagnosis of coronary atherosclerosis. At present, the access of choice for coronary angiography is transradial access1,2. Despite the progressive reduction in coronary procedural complications that have occurred over time, the existence of complications persists and can generate serious consequences1,2. The administration of radiological contrast may lead to the development of adverse events such as contrast-induced nephropathy (CIN) or allergic reactions3-5. Furthermore, the induction of radial spasm is related with cross-over to transfemoral access and further vascular complications6,7. Traditional technique for coronary angiography, by transradial access, uses independent catheters for the cannulation of each coronary artery, inducing radial spasm and requiring additional fluoroscopy time and contrast injections for the correct engage of coronary ostia. Nevertheless, the performance of a coronary angiography with a one-catheter strategy by multipurpose coronary catheters, like TIGER catheters, could simplify procedures decreasing radial spasm, procedural time, and radiological contrast consumption, and currently, it is the usual practice to perform trans-radial coronary angiographies.
In recent years, multiple studies have been published about the benefits of the one-catheter strategy, highlighting greater benefit in observational studies8-11 than in controlled studies12-16, which may entail a bias in the perception of the real benefits of this strategy, especially regarding radiological contrast saving. However, to date there are no studies that integrate the information derived from randomized clinical trials (RCT) to adequately quantify the advantages of the one-catheter strategy.
Therefore, we performed the first systematic review and meta-analysis of RCT evaluating one-catheter strategy versus two-catheter strategy to compare the amount of iodinated contrast, the induction of radial spasm and fluoroscopy and procedural time, between these two strategies for coronary angiography by transradial access.
Methods
Search strategy, endpoints, and data extraction
Two reviewers (DFR and JCM) independently searched PubMed, CINALH, and CENTRAL databases until November 2017. To be included, published studies should be randomized comparisons between one- and two-catheter strategies for diagnostic coronary angiography. Furthermore, articles had to report on the primary endpoint of our investigation and should be written in English language. The following terms or keywords were used: (one-catheter odds ratio [OR] single catheter OR TIGER catheter OR multipurpose catheter) AND (coronary angiography OR cardiac angiography) AND (controlled study OR randomized study OR RCT). Reference lists of included studies were scanned to retrieve additional relevant studies.
Primary endpoint was total volume of contrast administrated in coronary procedures. Secondary endpoints, evaluating coronary catheterization performance, included radial spasm (definitions according to each study in the Supplementary Material: Table 1), fluoroscopy time, and total procedural time.
Table 1 Design, type of multipurpose catheter, and endpoints of original randomized clinical trials
| Study year | Design | Type of catheter | Operators (n) | 1C (n) | 2C (n) | Contrast (mL) Mean ± SD Median (IQR) | Radial spasm n (%) | Fluoroscopy (sec) Mean ± SD Median (IQR) | Procedural time (sec) Mean ± SD Median (IQR) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1C | 2C | 1C | 2C | 1C | 2C | 1C | 2C | ||||||
| Turan et al. (2016)12 | RCT | Judkins Left | 3 | 103 | 103 | 50 ± 12 | 51 ± 13 | 13 (12.6%) | 23 (22.3%) | 157 ± 83 | 131±92 | 402 ± 126 | 474 ± 198 |
| Chen et al. (2016)13 | RCT | TIGER II | 7 | 57 | 53 | 48 ± 16 | 53 ± 19 | 3 (5.3%) | 3 (5.7%) | 184 ± 91 | 238 ± 131 | 337 ± 382 | 434 ± 137 |
| Erden et al. (2017)1414 | RCT | Modified Judkins Left | 2 | 194 | 193 | 49 ± 13 | 52 ± 18 | 22 (11.3%) | 42 (21.7%) | 120±138 | 138 ± 90 | 342 ± 186 | 372 ± 150 |
| Tarighatnia et al. (2017)15 | RCT | TIGER II | - | 128 | 128 | 51 ± 12 | 54 ± 16 | - | - | 152 ± 83 | 203 ± 121 | 570 ± 192 | 684 ± 240 |
| Xanthopoulou et al. (2017)16 | RCT | TIGER II | 10 | 320 | 320 | 67 (54-82) | 73 (60-94) | 52 (16.3%) | 93 (29.1%) | 121 (79-188) | 134 (90-210) | 331 (250-439) | 411 (309-578) |
RCT: randomized clinical trial; 1C: one-catheter strategy; 2C: two-catheter strategy; mL: milliliter; sec: seconds; SD: standard deviation; IQR: inter-quartile range. *Numerical data regarding iodinated contrast, fluoroscopy time and procedural time were rounded to the nearest unit to facilitate the understanding of the table.
RCT were selected if included information about volume of iodinated contrast and the following items were extracted from each selected article: year of publication, type of study design, type of catheter used, number of operators, sample size, total volume of contrast (mL), presence of radial spasm, fluoroscopy time (sec), total procedural time (sec), and baseline clinical characteristics. The authors of the original studies were not required to expand the information referred to such works. Disagreements regarding inclusion or exclusion criteria were resolved by consensus (Fig. 1).

Statistical analysis
These systematic review and meta-analysis were conducted in accordance with the criteria reported in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) consensus document (PRISMA)17.
Statistical analysis and forest-plot diagrams were performed using the Comprehensive Meta-Analysis software (Biostat, Englewood, NJ, USA). Pooled difference in means (DiM) or OR were used as summary statistics. All p-values were two-tailed, with statistical significance set at 0.05. The results were presented with a 95% confidence interval (95% CI). The authors assessed statistical heterogeneity using the I2 test. A fixed-effect model was used in absence of heterogeneity, and a random-effects model was used in case of detecting heterogeneity between studies (I2 statistic > 50%). Therefore, a fixed-effect model was used for the radial spasm and a random-effects model for the other endpoints. Sensitivity analyses for primary endpoint were conducted excluding one trial at a time.
Assessment of study quality and publication bias
Two authors (JC and KR) evaluated the selected RCT studies to assess their quality and possible biases, and in case of discrepancies, they were resolved by consensus. The quality and possible biases of RCT were evaluated using the validated criteria of Juni18. For the primary endpoint (volume of contrast administered), the publication bias was assessed using the Eggers statistical test for publication bias and visual inspection of the funnel plot19.
Results
In the literature review, a total of 670 articles were obtained. After reviewing all the titles and abstracts, 20 full-text articles were selected. Fifteen articles, from the total of selected articles, were excluded for the following reasons: four of them were observational studies, three articles informed about guiding catheters designed for combined procedures (diagnostic and therapeutic interventions), four papers were related with alternative arterial approaches to trans-radial access, and one article compared two types of universal dedicated catheters for right trans-radial approach in a one versus one-catheter strategy. It is noteworthy that three RCT comparing one versus two-catheter strategy were not included for the final analysis because one article did not inform about the primary endpoint of the study (volume of contrast administered)20 and two articles were not written in English language21,22 (Fig. 1). Finally, five studies met the inclusion criteria12-16.
These five RCT contained data on 1599 patients. Eight-hundred two patients underwent to one-catheter strategy and 797 patients to two-catheter strategy. Tables 1 and 2 depict main characteristics of the studies. Quality of studies was also evaluated (Table 3).
Table 2 Baseline clinical characteristics of original randomized clinical trials
| Turan et al. (2016)12 | Chen et al. (2016)13 | Erden et al. (2017)14 | Tarighatnia et al. (2017)15 | Xanthopoulou et al. (2017)16 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1C (n = 103) | 2C (n = 103) | 1C (n = 57) | 2C (n = 53) | 1C (n = 194) | 2C (n=193) | 1C (n = 128) | 2C (n = 128) | 1C (n = 320) | 2C (n = 320) | ||
| Age (Years), Mean ± SD | 59.7 ± 13.6 | 61.0 ± 11.1 | 65.2 ± 12.7 | 67.5 ± 9.9 | 57.9 (12.9) | 59.6 (13.1) | 59.5 ± 11.5 | 59.2 ± 10.0 | 66.2 ± 11.4 | 66.4 ± 11.7 | |
| Sex female, n (%) | 40 (38.8%) | 36 (34.9%) | 24 (42%) | 17 (32%) | 80 (41.2%) | 76 (39.4%) | 46 (35.9%) | 46(35.9%) | 91 (28.4%) | 86 (26.9%) | |
| BMI (Kg/m2), Mean ± SD* | 28.6 ± 4.9 | 28.9 ± 5.0 | 31.6 ± 7.7 | 30.9 ± 7.8 | 28.4 | 29.2 | 27.3 ± 4.8 | 27.7 ± 4.2 | 28.4 ± 4.8 | 28.4 ± 4.5 | |
| Medical history | Hypertension, n (%) | 59 (57.3%) | 61 (59.2%) | 49 (86.0%) | 42 (79.2%) | 123 (63.4%) | 126 (65.2%) | - | - | 192 (60.0%) | 193 (60.3%) |
| Dyslipidemia, n (%) | 36 (35.0%) | 34 (33.0%) | 44 (77.2%) | 38 (71.7%) | 84 (43.2%) | 88 (45.5%) | - | - | 170 (53.1%) | 157 (49.1%) | |
| Diabetes, n (%) | 39 (37.9%) | 43 (41.7%) | 20 (35.1%) | 22 (41.5%) | 66 (34.0%) | 69 (35.7%) | - | - | 86 (26.9%) | 81 (25.3%) | |
| Smoker, n (%) | 31 (30.1%) | 33 (32.0%) | 13 (22.8%) | 6 (11.3%) | 62 (31.9%) | 59 (30.5%) | - | - | 150 (46.9%) | 144 (45.0%) | |
| Previous PCI, n (%) | 31 (30.1%) | 28 (27.2%) | - | - | 56 (28.8%) | 58 (30.0%) | - | - | - | - | |
| Technical events | Supplemental catheter, n(%) | 35 (34.0%) | 1 (0.97%) | 8 (14.0%) | 0 (0%) | 21 (10.8%) | 5 (2.6%) | - | - | 57 (17.8%) | 68 (21.3%) |
| Severity of coronary artery disease | No disease, n (%) | 33 (32.0%) | 39 (37.9%) | - | - | 71 (36.7%) | 71 (33.5%) | - | - | 164 (51.2%) | 155 (48.4%) |
| 1 vessel disease, n (%) | 39 (37.9%) | 34 (33.0%) | - | - | 69 (35.5%) | 70 (36.2%) | - | - | 79 (24.7%) | 77 (24.1%) | |
| 2 vessel disease, n (%) | 20 (19.4%) | 19 (18.4%) | - | - | 32 (16.4%) | 38 (19.6%) | - | - | 42 (13.1%) | 35 (10.9%) | |
| 3 vessel disease, n (%) | 11 (10.7%) | 11 (10.7%) | - | - | 22 (11.3%) | 20 (10.3%) | - | - | 35 (10.9%) | 53 (16.6%) | |
1C: one-catheter strategy; 2C: two-catheter strategy; SD: standard deviation: BMI: body mass index.
*SD in BMI was not reported in Erden article.
Table 3 Quality assessment for randomized clinical trials included in the systematic review (Juni Criteria)
| Studies | Turan et al. (2016)12 | Chen et al. (2016) 13 | Erden et al. (2017) 14 | Tarighatnia et al. (2017) 15 | Xanthopoulou et al. (2017)16 |
|---|---|---|---|---|---|
| Selection | |||||
| 1. Was allocation adequate? Mean-central site, numeric code, opaque envelopes, drugs prepared by pharmacy | Yes | Yes | Yes | Yes | Yes |
| 2. Was an adequate method of randomization described? | Yes | Yes | Yes | Yes | Yes |
| 3. Were groups similar at the start of the study? | Yes | Yes | Yes | Yes | Yes |
| Performance | |||||
| 4. Were the patients/caregivers blinded to the intervention? | No | No | No | No | No |
| Detection | |||||
| 5. Was the outcome ascertained blindly? | Yes | Yes | Yes | Yes | Yes |
| Attrition | |||||
| 6. What percentage was lost at follow-up? | 0% | 0% | 0% | 0% | 0% |
| 7. Were all patients analyzed in the group to which they were assigned (intention-to-treat analysis)? | No | Yes | No | Yes | Yes |
Regarding to the total volume of contrast used, all five studies12-16 were used for the pooled analysis. A significant difference was observed in the total volume of contrast administered favorable to one-catheter strategy (DiM [95% CI]; −3.831 mL [−6.165 mL-−1.496 mL], p = 0.001). A random-effects model was used because the presence of significant heterogeneity (I2 test = 59.1%) (Fig. 2). Publication bias was not detected based on visual inspection of the funnel plot and Eggers regression test for small study effect. Volume of contrast comparison is provided as an example which showed symmetrical funnel plot (Supplementary Fig.1) and p = 0.35 for Eggers test. The sensitivity analysis by excluding one study at a time did not change direction of the pooled effect sizes.

Figure 2 Forest-plot representing volume of contrast administrated. mL: Milliliters. CI: Confidence interval. 1C: One-catheter strategy. 2C: Two-catheter strategy.
Four controlled trials12-14,16 informed regarding radial spasm, including 674 patients in the 1C group and 669 patients in the 2C group. 1C group presented less induction of radial spasm (OR [95% CI]; 0.484 [0.363-0.644], p < 0.001). A fixed-effects model was used because the absence of heterogeneity (I2 test = 0.0%) (Fig. 3).

Figure 3 Forest-plot representing radial spasm. CI: Confidence interval. 1C: One-catheter strategy. 2C: Two-catheter strategy.
In the analysis related to fluoroscopy time, all five RCT12-16 were included for the analysis. No differences were detected on fluoroscopy time was detected between groups (DiM [95% CI], −19.193 s [−41.425 s to −3.039 s], p = 0.091). It is noteworthy that a random effects model was performed to the significant heterogeneity (I2 test = 82.3%) (Fig. 4).

Figure 4 Forest-plot representing fluoroscopy time. sec: Seconds. CI: Confidence interval. 1C: One-catheter strategy. 2C: Two-catheter strategy.
All five randomized trials12-16 informed regarding the total procedural time. A significant difference was observed (DiM [95% CI], −72.471 s [−99.694 s to-45.249 s], p < 0.001). Because the heterogeneity, a random effects method was used (I2 test = 58.2%) (Fig. 5).
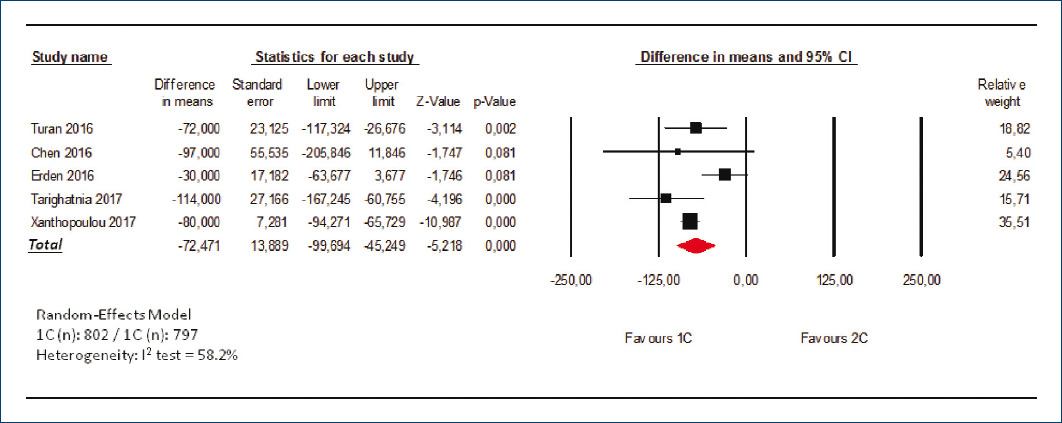
Discussion
The main findings in our investigation were that of one-catheter strategy is associated with a minimal reduction in the volume of iodinated contrast used in coronary angiography procedures and a better performance in diagnostic coronary catheterization, evaluated as radial spasm and procedural time, in comparison with conventional two-catheter strategy.
Radiological contrast administration
One of main complications of invasive coronary procedures is the development of CIN. This condition could reach one-third of patients undergoing coronary procedures and is one of the more common causes of acute kidney injury in cardiological patients3,4,23,24. Furthermore, CIN is related with prolongation of the hospitalization, the death at short- and long-term3,4 and increments in direct and indirect costs25. Because of the amount of iodinated contrast used in angiographic procedures is closely linked to CIN26,27, the implementation of any technique that could reduce the administration of radiological contrast is very much appreciated by interventional cardiologists.
Pooled results show a consistent reduction in the primary endpoint of the study (volume of radiological contrast used in coronary diagnostic procedures). Nevertheless, the reduction in contrast administration is minimal in the joint analysis of RCT (DiM [95% CI]; −3.831 mL [−6.165 mL-−1.496 mL], p = 0.001). A recent observational study with a large number of patients observed a reduction in contrast administration, by one-catheter strategy, reaching 20 mL of radiological contrast28. However, the study of Langer et al.28 could perhaps overestimate the effect of the one-catheter strategy on contrast saving, since it was an observational and retrospective study. This could also be motivated because in the participating centers, the standard catheter for performing coronary angiography in the usual clinical practice was the Tiger multipurpose catheter and the two-catheter strategy was used less frequently and this fact could penalize the two-catheter strategy.
The main finding of our study, which only analyzes randomized studies, is that the amount of contrast saved by the one-catheter strategy is very small. This fact implies that the preference of the one-catheter strategy over the two-catheter strategy at the time of performing coronary procedures would not be mediated by the supposed saving of radiological contrast but by other aspects related to the catheterization performance as we explain below.
Coronary catheterization performance
Radial spasm is a relatively common complication on transradial access with a variable incidence, ranging from 5% to 30%, depending on the definition29-33. Radial spasm induces patient discomfort and reduces procedural success29,30. In cases with need for conversion to transfemoral access is related with an increase in vascular complications1,34.
Many factors, such as age, female gender, multiple radial punctures, and radial diameter are related with radial spasm.6,7,30-32. Furthermore, exchange of catheters during by transradial access has been linked to radial spasm induction, probably in relation to the repeated stimulation of the radial artery6. Likewise, the prolonged duration of coronary procedures may favor the development of arterial spasm and reduces patient comfort in trans-radial procedures, associating with greater probability of complications6,7,30-32.
Our results show an important reduction in radial spasm (OR [95% CI], 0.484 [0.363-0.644], p < 0.001). Furthermore, one-catheter strategy produces a small reduction in procedural time (DiM [95% CI], −72.471 s [−99.694 s-−45.249 s], p < 0.001) in comparison with conventional strategy, but no significant differences between groups were detected on fluoroscopy time despite the favorable trend to one-catheter strategy (DiM [95% CI], −19.193 s [−41.425 s to −3.039 s], p = 0.091).
These facts make us hypothesize that one-catheter strategy, by reducing radial spasm development, simplifies the manipulation of coronary catheters resulting in slightly shorter times to complete diagnostic procedures and could decrease potential complications associated with radial spasm.
Limitations
The present study is limited by the presence of heterogeneity for some of the outcomes, which can be explained in part by the variation in the study design. However, random-effects models were used to mitigate this limitation if heterogeneity was detected. Due to lack of access to primary data, analyses based on patient characteristics regarding primary and secondary endpoints could not be performed. Nevertheless, our work is the first one performing a pooled analysis of RCT evaluating one-catheter strategy for diagnostic coronary angiography which ensures the high quality of the studies included in the combined analysis.
Furthermore, individual studies included were not blinded to operators. This fact could influence operators regarding technical aspects like the final number of angiographical views, the fluoroscopy time or the total amount of contrast used. However, because the studies were protocolized randomized trials, the chances that the lack of blinding of the studies could affect the results are minimized.
Conclusions
One-catheter strategy for trans-radial coronary angiography induces only a minimal reduction on radiological contrast administration. Nevertheless, one-catheter strategy improves coronary catheterization performance, by reducing arterial spasm, and procedural time, as compared to two-catheter strategy.

