











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkA 64-year-old male with no medical background was admitted to the ER after 1 week of epigastric pain. At his arrival was found in acute pulmonary edema, electrocardiogram revealed sinus tachycardia, negative ST-segment deviation in V4-V6, and positive deviation in aVR. He developed cardiogenic shock. Coronary angiography showed multivessel disease with the left circumflex artery as the culprit artery. A transthoracic echocardiogram was performed, reporting a left ventricle ejection fraction of 48%, hypokinesia of inferolateral wall in the basal segment, the mitral valve showed normal leaflets but with closure limitation conditioning important mitral regurgitation with suspected rupture of the papillary muscle. On continuous Doppler interrogation of the mitral regurgitant jet, the spectral signal had a peculiar sound such as goose croak and a linear fragmentation of the image on the Fourier register resembling “tiger stripes” suggesting an oscillating intracardiac structure, in this case, posteromedial papillary muscle rupture (Fig. 1), which was confirmed with a transesophageal echocardiogram (Fig. 2).

Figure 1 Transthoracic echocardiography showing continuous Doppler interrogation of the mitral regurgitant jet showing fragmentation on the Fourier Register.
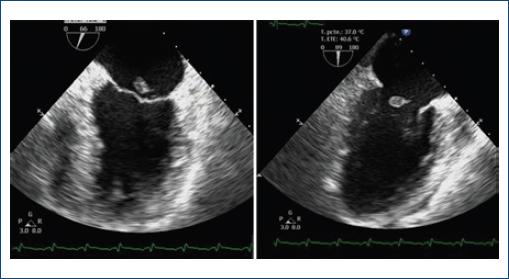
Figure 2 Transesophagic echocardiogram in midesophageal two chamber view showing rupture of the posteromedial papillary muscle.
The causes of mitral regurgitation after acute myocardial infarction include ischemic papillary muscle dysfunction, left ventricular dilatation or true aneurysm, and papillary muscle or chord rupture1-2. Transesophageal echocardiography is essential for confirmation. These band-like signals appear to be associated with intracardiac oscillating structures with the first band (lowest frequency on the Doppler recording) representing its fundamental frequency. These structures vibrate with a single frequency with several harmonic overtones. Differential diagnosis of “tiger stripes” includes valve regurgitation, flail prosthetic valve leaflet, and possibly Lambl’s excrescences as previously reported1-3.

