











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkInfluenza virus infection has incidence rates of up to 350 cases/100,000 population in the authors setting. However, influenza virus myocarditis is still an uncommon complication. We presented the case of a 35-year-old-man, smoker and occasional cocaine consumption, who presented with pericardial chest pain and respiratory infection signs related to influenza virus-positive serology. Initial echocardiogram showed severe ventricular dysfunction (left ventricular ejection fraction; LVEF, 24%) and mild pericardial effusion. Due to progression to cardiogenic shock, he was admitted to the Acute Cardiologic Care Unit with a diagnosis of fulminating influenza A myocarditis and treatment with oseltamivir and vasoactive support with dobutamine and norepinephrine was instituted. Despite this, and given the presence of resistant cardiogenic shock (INTERMACS 1), implanting a venoarterial extracorporeal membrane oxygenation (ECMO) device was decided, whereby the improvement of hemodynamic and analytical parameters was achieved. At 12 h of the implant, the patient experienced new hemodynamic deterioration, and the echocardiogram revealed pericardial effusion progression with signs consistent with cardiac tamponade, which prompted urgent pericardiocentesis to improve the clinical situation. Subsequent evolution was good, with progressive biventricular function improvement until normalization and withdrawal of the device on the 7th day. This case illustrates the most serious complications related to influenza myocarditis, such as progressive and deep cardiogenic shock, with biventricular dysfunction complicated with cardiac tamponade; regarding the latter, restoring the hemodynamic situation was possible thanks to VA-ECMO early implantation, which reversed the catastrophic situation and favored the recovery since the procedure involved an acute and potentially reversible triggering factor.
Cardiac compromise secondary to influenza virus infection can occur in different clinical forms, ranging from acute pericarditis to cardiac tamponade or takotsubo syndrome1.
We present the case of a 35-year-old male with a history of alcohol and cocaine use, usual tobacco, and marijuana smoker, who sought medical attention for chest pain. He referred to previous symptoms of cough, expectoration, and diffuse myalgia in the previous 5 days. Three days before admission, he started experiencing stabbing chest pain, radiating to the back, which increased with inspiration and decubitus, and progressive clinical deterioration. On physical examination, sinus tachycardia (120 beats/min), hypotension (systolic blood pressure of 95 mmHg), fever (37.5ºC) and data consistent with peripheral hypoperfusion (cold skin) were evident.
Analyses revealed leukocytosis with neutrophilia (18 × 103/μL leukocytes with 9.5 × 103 neutrophils), coagulopathy (spontaneous INR, 1.4; APTT, 38 s; and PT, 17.6 s), liver damage (total bilirubin, 2.46 mg/dL; GOT/AST, 86 IU/L; GPT/ALT, 85 IU/L; GGT, 107 IU/L; LDH, 310 IU/L; and alkaline phosphatase, 115 IU/L) and hyperlactacidemia (lactic acid, 4.5 mg/mL). The electrocardiogram showed sinus tachycardia without repolarization alterations or signs of acute ischemia. Transthoracic echocardiogram showed a non-dilated left ventricle (left ventricular end-diastolic volume, 45 mm) with an edematous appearance and thicknesses at the upper limit of normal (12 mm) and global hypokinesia, which caused a highly depressed ventricular function (biplanar left ventricular ejection fraction, LVEF, 25%), transmitral filling with wave fusion and filling pressures elevation with an E/E ratio of 16, preserved right ventricular function (TAPSE, 18 mm; S wave, 12.5 cm/s), a pulmonary systolic pressure of 45 mmHg and mild pericardial effusion (10 mm on the right ventricular free wall); no significant valve disease was observed. The patient was admitted with a diagnosis of acute myocarditis and the test for influenza A virus was positive, with the rest of microbiological determinations being negative, and thus, treatment with oseltamivir was initiated.
During the first few hours, the patient developed progressive hemodynamic deterioration, with hypotension and tissue perfusion worsening (surveillance with Swan-Ganz catheter; mean BP, 70 mmHg; HR, 130 bpm; CO, 3.1 L/min; CI, 1.8 L/min/m2; CVP, 20; SVR 1,290 dynes/m2; and central venous saturation, 57%), and oligoanuria, with increasing doses of vasoactive treatment with dobutamine and norepinephrine administration being required, as well as orotracheal intubation and ventilatory support. Despite these measures, the patient still developed signs of low output resistant to the instituted measures; serial echocardiograms showed biventricular function progressive deterioration (biplanar LVEF, 15%; TAPSE, 10 cm; RV S-wave, 7.5 cm/s; and CAF, 30%). In view of the INTERMACS 1 cardiogenic shock scenario (critical cardiogenic shock)2, ventricular assist venoarterial extracorporeal membrane oxygenation (ECMO, CARDIOHELP, MAQUET Cardiopulmonary AG, Germany) implantation was decided, thanks to which hemodynamic parameters rapid improvement was achieved, with diuresis and laboratory values recovery, and hyperlactacidemia correction until normalization.
After 12 h of the device implantation, the patient experienced rapidly-progressing hemodynamic deterioration, with central venous pressure elevation and ECMO support attenuation. Echocardiogram revealed the presence of severe pericardial effusion with data consistent with cardiac tamponade (right atrial partial collapse, 45% transtricuspid flow respiratory variation, and dilated inferior vena cava without respiratory collapse) (Fig. 1), as well as the presence of spontaneous echo-contrast inside the left cavities, in relation to filling pressures elevation and afterload increase. Consequently, an evacuating pericardiocentesis was performed, which drained 500 ml of serous fluid, which is consistent with inflammatory exudate, and an intra-aortic counterpulsation balloon pump was implanted, which contributed to improve ventricular discharge. With these measures, the patient recovered hemodynamic stability, which he maintained for the next few days and only required support with norepinephrine for a certain vasoplegia (mean BP, 55 mmHg; CO, 4.3 L/min; and SVR, 800 dynes/m2). Endomyocardial biopsy showed minimal inflammatory infiltrate (Fig. 2). Subsequent evolution was good, with biventricular function progressive improvement until normalization, and the device was removed on the 7th day. Subsequently, he could be discharged under optimized medical treatment.
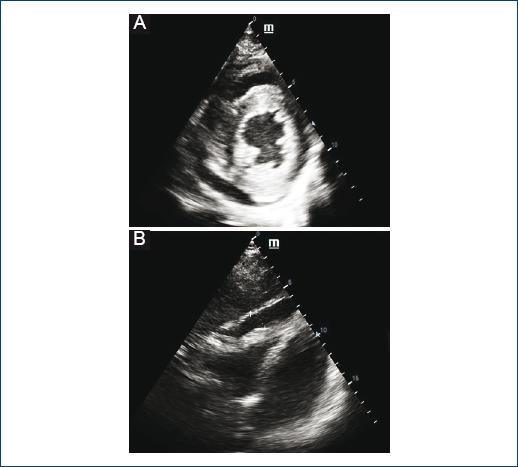
Figure 1 A: Transthoracic echocardiogram (parasternal plane, short axis) revealing circumferential pericardial effusion. B: subcostal plane delineating pericardial effusion on right ventricular free wall.

Figure 2 A: Endomyocardial biopsy showing inflammatory interstitial infiltrate. B: endomyocardial biopsy immunohistochemistry revealing CD3+ cells infiltrating the tissue.
Case series of fulminant myocarditis due to the influenza virus, especially in children, most with acute presentation and rapid progression, have been described in the literature, with the predisposing factors currently not being known3. VA-ECMO-type circulatory assistance provides hemodynamic and respiratory support, which ensures adequate peripheral perfusion in patients with catastrophic cardiogenic shock that is resistant to other measures (INTERMACS 1); an early implant is a essential measure and preferred over other circulatory assistance devices, particularly in case of biventricular failure4-6. The use of these devices has contributed to reduce mortality in this situation and can be used as a transition to recovery, as in this case, or as a bridge to heart transplantation or another type of assistance6.
This case illustrates the most serious complications associated with influenza myocarditis, such as progressive and deep cardiogenic shock, with severe biventricular dysfunction and appearance of progressive pericardial effusion, which gives rise to cardiac tamponade development and ventricular filling compromise and, in this case also normal functioning of assistance. VA-ECMO early implantation managed to re-establish patient hemodynamic situation by reversing the cardiogenic shock that he was in and to promote his recovery, given that this is an acute and potentially reversible trigger4,5,7.

