











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkA 32-year-old male was referred to the cardiology outpatient clinic of our institution for follow-up of dilated cardiomyopathy. At the age of 3 months, he had presented significant dyspnea and an enlarged cardiac silhouette had been discovered at the chest X-ray. Echocardiography had showed the left atrium (LA) and left ventricle (LV) dilation with severely depressed LV ejection fraction (LVEF). A diagnosis of dilated cardiomyopathy was made at that time. He had been treated transitorily with loop diuretics and permanently with angiotensin-converting enzyme inhibitors and beta-blockers. He was stabilized and evolved in New York Heart Association functional Class II/IV reaching the adulthood.
His last transthoracic echocardiography showed markedly LA and LV dilation, moderately reduced (43%) LVEF and trabeculated areas at the LV apical segments. Coronary artery disease was ruled out by a normal coronary angiography.
With the suspicion of non-compaction cardiomyopathy, a cardiac magnetic resonance (CMR) was requested. The cine steady-state free precession images demonstrated enlarge left cavities with moderately depressed LVEF, normal interventricular wall thickness, and right and left apical ventricular hypertrabeculation, although not fulfilling non-compaction criteria (Fig. 1).

Figure 1 Cardiac magnetic resonance: cine steady-state free precession. Left atrium and left ventricle (LV) dilation with RV and LV trabeculation. (A) Four chamber view. (B) Midventricular short-axis view.
At late gadolinium images, a diffused subendocardial late gadolinium hyperenhancement involving the basal and midsegments of the LV in a circumferential pattern was present (Fig. 2). At that time, etiological diagnosis of endocardial fibroelastosis (EFE) was performed.
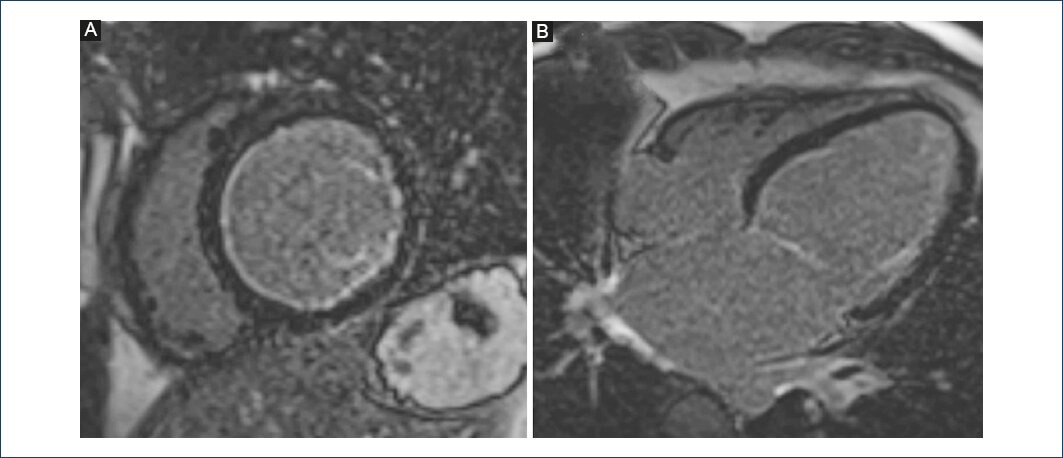
Figure 2 Cardiac magnetic resonance: late gadolinium enhancement sequence. Diffused subendocardial hyperenhancement. (A) Midventricular short-axis view. (B) Four chamber view.
EFE is a rare condition, whose primary form manifests most frequently during the 1st month of life. It consists of a thickening of the endocardium by collagen and elastic fibers1. Its secondary form is mostly related to hypereosinophilia and lymphoproliferative disorders2. Primary EFE is mostly manifested with dilation and systolic impairment of the LV. However, there are primary EFE cases with features of other conditions such as restrictive cardiomyopathy3. A great number of cases have poor prognosis and require heart transplantation during childhood, some of them misdiagnosed mostly as dilated cardiomyopathy4.
There are not unified diagnostic criteria for this disease, what rends the diagnosis difficult during the adult age. A high grade of suspicion, comprehensive clinical history, and histological evidence of fibrosis either by biopsy or at the CMR are mandatory.
In our particular case, clinical history with onset at 3 months of age and diffused EFE evidenced at CMR enabled this diagnosis.

