











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkParavalvular leak (PVL) is a common and challenging problem that has existed since prosthetic cardiac valves were first implanted. PVL occurs in 7-17% of mitral valve replacements (MVRs) and 5-10% of aortic valve replacements (AVRs)1 and can be associated with disabling symptoms related to heart failure or hemolysis2. Repeat surgery to repair PVL is associated with significant mortality and morbidity3. Tissues around PVL are often calcified and friable, and therefore, leaks may recur4. Conservative management of mild-to-moderate leaks is also associated with high adverse event rates because leaks tend to deteriorate over time5. Despite the varied morphologies of PVLs, it is clear from all the series that oblong devices are preferentially selected by implanting cardiologists for closing PVLs in all the countries6. Due to the lack of specifically designed devices for PVL (mitral and aortic) in Mexico, we report on the first use in our country of such a device in two patients with PVL.
Case report
Case 1
A 61-year-old male with history of hypertension, dyslipidemia, and rheumatic valvular disease, underwent AVR 18 years ago. Due to rheumatic mitral disease, 8 years ago underwent MVR using a St. Jude mechanical valve. He was admitted in our hospital with shortness of breath and decrease in functional capacity. Blood pressure: 130/80 mmHg, heart rate: 110 bpm. There was an atrial fibrillation rhythm on electrocardiogram (ECG). He had hemolytic anemia due to important hemolysis requiring blood transfusions. Two- and three-dimensional transesophageal echocardiography (TEE) detected severe mitral PVL. The site of the leak was identified at the anterior border of the St. Jude mitral valve. Due to his higher surgical risk, a transcatheter approach was offered to the patient. A percutaneous closure of mitral PVL was performed with a CERA™ muscular ventricular septal defect (VSD) occluder (14 mm) with mild residual paravalvular leakage as a result.
After 2-year, ambulatory follow-up persisted with deteriorated functional capacity and hemolytic anemia. Two- and three-dimensional TEE detected a new site of PVL at the posterior border of the St. Jude valve. A transcatheter approach was offered once again. Due to the previous lack of a specifically designed device for leaks, the patient was offered to have his leak closed using an Occlutech™ Paravalvular Leak Device (PLD) (Occlutech GmbH, Jena, Germany) designed specifically for this valvar complication.
Procedure
The procedure was performed under general endotracheal anesthesia. An 8 Fr sheath was inserted in the right femoral vein. With a Brockenbrough needle (Medtronic, Santa Rosa, California), the transseptal puncture was made (Fig. 1A) and a Mullins 9 Fr sheath (Medtronic, Santa Rosa, California) was placed in the left atrium (Fig. 1B), after this, a 5 Fr AL-2 curve catheter was introduced. Under fluoroscopic and TEE guidance, a hydrophilic guidewire was manipulated across the leak and the catheter was advanced over the wire to the left ventricle (Fig. 1C). Then, the catheter was replaced with a 7 Fr delivery sheath (Fig. 1D). A rectangular PVL device with an ellipsoid waist of 12 × 5 mm from Occlutech™ was delivered under fluoroscopic and TEE guidance first deploying a disc in the left ventricle and the second disc in the left atrium (Fig. 1E and F). Repeat TEE revealed the device to be in good position and minimal flow was present. Therefore, the device was released, and few minutes later, repeat TEE revealed good position and no residual shunt. Sheath was removed and the venous access was closed in the usual fashion with a Perclose ProGlide device (Abbott Vascular, Santa Clara, California). The patient was discharged home in few days on antiplatelet therapy (Aspirin) in addition to Coumadin. On follow-up, at 6 months, he has been asymptomatic with no signs of hemolysis or dyspnea. TEE demonstrated the device to be in good position and no PVL.
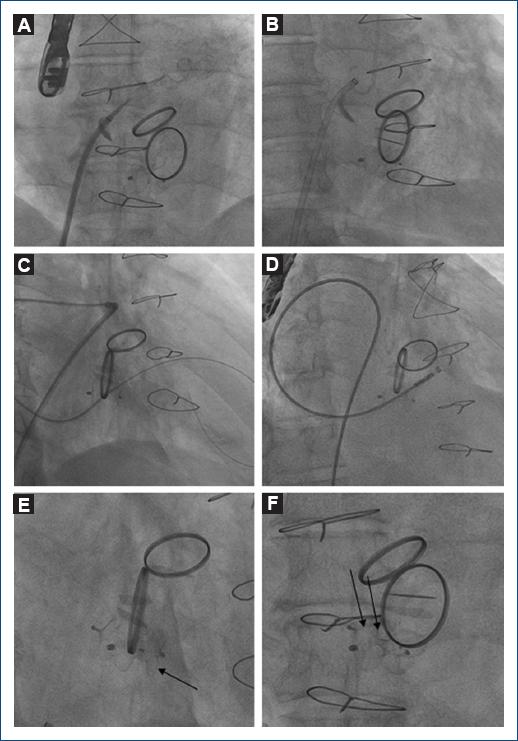
Figure 1 Step by step of percutaneous closure of mitral paravalvular leak through a transseptal approach: A: transseptal puncture was made with a Brockenbrough™ needle through the left atrium. B: A Mullins™ 9 Fr sheath was placed in the left atrium, after this, a 5 Fr AL-2 catheter was introduced. C: Under fluoroscopic guidance, a hydrophilic guidewire was manipulated across the paravalvular leak. D: A 7 Fr delivery sheath is advanced through the left ventricle cavity. E: Fluoroscopic control in RAO projection: an Occlutech™ Paravalvular Leak Device (PLD) rectangular device (ellipsoid waist of 12 mm × 5 mm) was delivered next to the previous device (arrow). F: Fluoroscopic control in anteroposterior projection: PLD device (arrows) was released in good position. See text for further details.
Case 2
A 64-year-old male with history of hypertension. Due to rheumatic heart disease, 4 years ago underwent AVR using a CarboMedics Mechanical Valve was admitted with shortness of breath and decrease in functional capacity. Blood pressure: 110/70 mmHg, heart rate: 100 bpm. There was a sinus rhythm on ECG. He had hemolytic anemia due to severe hemolysis requiring blood transfusions. Two- and Three-dimensional TEE detected severe aortic PVL. The site of the leak was identified at the posterior border of the CarboMedics valve. Due to his higher surgical risk (hostile thorax, reoperation, and high surgical mortality risk), a transcatheter approach was offered to the patient. It was offered to have his leak closed using an Occlutech™ PLD (Occlutech GmbH, Jena, Germany).
Procedure
The procedure was done under general endotracheal anesthesia and TEE guidance, the right femoral artery was accessed using a 10 Fr short sheath. An ascending aorta angiogram was done and revealed the presence of severe paravalvular aortic regurgitation (Fig. 2A). Under fluoroscopic and TEE guidance, a hydrophilic guidewire was manipulated across the leak and the 9 Fr delivery sheath was advanced to the left ventricle cavity (Fig. 2B). A rectangular PVL device with a waist of 12 × 5 mm from Occlutech™ was delivered under fluoroscopic and TEE guidance (Fig. 2C). Repeat ascending aorta angiogram revealed good device position and mild residual shunt (Fig. 2D), few minutes later, repeat TEE revealed the device to be in good position and minimal flow was present (Fig. 2E and F). The patient is also doing well with no signs of hemolysis or dyspnea at 6-month follow-up. TEE demonstrated good device position and mild PVL.
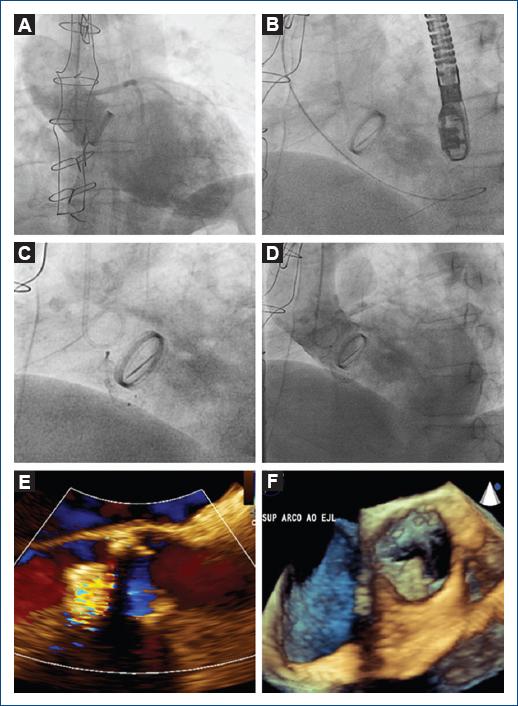
Figure 2 Step by step of percutaneous closure of aortic paravalvular leak through a transfemoral approach: A: ascending aorta angiogram revealed severe paravalvular aortic regurgitation. B: Under fluoroscopic and transesophageal echocardiography (TEE) guidance, a hydrophilic guidewire crossed the leak to the left ventricle cavity. C: A rectangular 12 mm × 5 mm Occlutech™ PLD device was delivered under fluoroscopic and TEE guidance. D: Repeat ascending aorta angiogram revealed good device position and mild residual shunt. E: Transthoracic echocardiogram in parasternal long-axis revealed a mild residual retrograde flow. F: Three-dimensional transesophageal echocardiogram demonstrated good device position. See text for further details.
Discussion
Transcatheter approach has been reported for the 1st time in 1992 using umbrella-type devices with acceptable results7. Since then, multiple devices have been used to close paravalvular mitral and aortic leaks. The major issue using such devices that were designed to close different defects (atrial septal defect, persistent ductus arteriosus, and VSD) for the purpose of closing such leaks is the high incidence of residual shunt4,6,7. Therefore, having a device specifically designed to close such leaks brings with it lower incidence of residual shunt8.
The Occlutech™ PVL device is designed with all the eligible criteria to achieve complete closure. The device can be delivered from various approaches using small delivery catheters. In addition, this device together with the Amplatzer™ Vascular Plug III (AVP III) is the only devices that have obtained the European CE Mark for the closure of PVLs9. Compared with the Occlutech™ PLD device, AVP III device is available in smaller sizes (largest long-axis diameter of 14 mm compared with PLD range of 11.5-28 mm) and has narrower overhanging rims. Unless multiple AVP III devices are used, it is only suitable for small PVLs. The design and particularly the larger size ranges of the rectangular Occlutech™ PLD are suited to the most frequently encountered large crescentic leaks in symptomatic patients, being this the rationale of using the Occlutech™ device in these two cases of large PVLs.
These two cases performed for the 1st time in our country highlight the versatility of this device. In both cases, rectangular shape devices were important to cover the crescent shape defect and in both complete closures were achieved. In our cases, given the available large sizes of rectangular devices, none of the individual leaks needed more than one device for occlusion, minimizing the risk of device embolization.
The Occlutech™ range of PLD occluders is designed to tackle a large range of PVL sizes and morphologies. In our series of cases, the devices performed well when implanted through a transfemoral and transseptal approach. This is the first experience with these devices in Mexico and part of the accumulated experience in our center with the different occluders available.
Financing
The authors did not receive any payment or economic benefit for the preparation and execution of this article.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.

